We sought to investigate whether older paternal age at the time of birth is associated with schizophrenia and other schizophrenia spectrum disorders among the offspring. Several lines of evidence support a relation between older paternal age and schizophrenia spectrum disorders. First, most previous studies that examined this relationship have demonstrated positive associations
(1–
5), although these studies have been criticized for methodologic limitations. Most recently, Malaspina et al.
(1), in a large Israeli birth cohort, demonstrated a robust and “dose-related” effect of paternal age on risk of schizophrenia and related disorders, a finding that was unaltered after adjusting for maternal age.
A second reason for examining paternal age in relation to schizophrenia is that older age of the father at the time of birth has been associated with several congenital disorders
(6–
10). The etiology of these associations is believed to involve new, autosomal dominant mutations in the male germ cell line. If a disruption of fetal development plays a role in the pathogenesis of schizophrenia, then new mutations secondary to advanced paternal age may operate to increase the risk of this disorder by adversely affecting brain development.
In the present investigation, we used data from the birth cohort of the Prenatal Determinants of Schizophrenia study
(11) to address the relation of paternal age to schizophrenia. We hypothesized that the risk of schizophrenia would increase with advancing paternal age.
The Prenatal Determinants of Schizophrenia study had several design advantages that permitted us to address significant limitations of previous studies. First, most prior studies relied on exposure data from a variety of sources, some of questionable reliability. In contrast, the Prenatal Determinants of Schizophrenia study offered prospectively acquired data on paternal age from a direct interview, serving to diminish the likelihood of exposure misclassification. Second, most prior studies relied on case series to identify patients for study; the present investigation addressed this limitation by employing a cohort design that included continuous follow-up for ascertainment of cases of schizophrenia. These first two features help to minimize selection bias, as well as biases arising from the use of prevalent rather than incident cases of schizophrenia spectrum disorders. Third, previous investigations generally relied on chart diagnoses of schizophrenia spectrum disorders by older and less reliable diagnostic systems, or on hospital registry data; in our study, most cases were identified by means of face-to-face standardized research interviews and consensus procedures that used modern diagnostic criteria. Fourth, most prior studies did not control for maternal age, and nearly all failed to adjust for other confounders; the comprehensive data set of our study permitted us to control for these factors. Finally, unlike previous studies, our study assessed and confirmed biological paternity of the offspring in the majority of subjects.
Method
Subjects
The subjects for the present investigation consisted of the birth cohort of the Prenatal Determinants of Schizophrenia study. The design of this study has been described in full by Susser et al.
(11) and will therefore be only briefly summarized here. The Prenatal Determinants of Schizophrenia study is a continuous follow-up of schizophrenia in the Child Health and Development Study cohort. The Child Health and Development Study recruited nearly all pregnant women in Alameda County, California, who received prenatal care from the Kaiser Foundation Health Plan, a large prepaid health care plan. The 19,044 live births to these women from 1959–1967 constituted the Child Health and Development Study cohort. The members of the Kaiser Foundation Health Plan were racially, educationally, and occupationally diverse, although there was some underrepresentation of the extremes of income
(12).
Kaiser Foundation Health Plan maintained records of all psychiatric and medical care received by members; beginning in 1981, the records were computerized. These records were used to ascertain potential cases of schizophrenia spectrum disorders. Accordingly, the Prenatal Determinants of Schizophrenia study cohort consists of the subsample of 12,094 subjects who were born into the Child Health and Development Study cohort and were members of the Kaiser Foundation Health Plan from January 1, 1981, through the last date for case ascertainment in the Prenatal Determinants of Schizophrenia study, which was December 31, 1997. The youngest cohort members were aged 14 to 30 years, and the oldest cohort members were aged 22 to 38 years during this period. The median follow-up time among comparison subjects was 30 years.
Data Collection
At the time of the enrollment of pregnancies in the Child Health and Development Study, each mother was administered an interview that included questions on parental birth dates. Data on parental age were recorded only for gravidas that were married, which included virtually the entire sample. Parental ages on the birth dates of their offspring were calculated in years.
Ascertainment and Diagnosis
Ascertainment
The protocol for ascertainment and diagnosis of cases of schizophrenia spectrum disorders is fully described elsewhere
(11). Briefly, schizophrenia spectrum disorders included the following disorders: schizophrenia, schizoaffective disorder, delusional disorder, psychotic disorder not otherwise specified, and schizotypal personality disorder
(13,
14). Ascertainment and diagnosis were accomplished by a three-step procedure. First, all individuals in the cohort treated for psychiatric disorders during Kaiser Foundation Health Plan membership were ascertained by means of the Kaiser Foundation Health Plan computerized inpatient and outpatient registries and a registry of outpatient pharmacy use. The inpatient registry, which began in 1981, included all psychiatric hospitalizations of Kaiser Foundation Health Plan members. The outpatient registry was also introduced in 1981 and included all outpatient contacts for psychiatric care. Supplementary data were provided by the Kaiser Foundation Health Plan outpatient pharmacy registry in order to ascertain cohort members prescribed antipsychotic medications; this registry commenced in 1992.
Second, subjects ascertained by these case registries were screened to identify potential cases of schizophrenia spectrum disorders. Subjects ascertained by means if the inpatient registry were initially screened by using ICD-9 diagnoses 295–299, followed by a review of medical and psychiatric records of all subjects with these diagnoses by two experienced psychiatric diagnosticians. For subjects in the outpatient registry, any subject with an ICD-9 diagnosis of 295–299 was considered to potentially have a schizophrenia spectrum disorder. In addition, all individuals prescribed antipsychotics were considered to potentially have a schizophrenia spectrum disorder. All of the subjects who potentially had these disorders (N=183) were targeted for a face-to-face diagnostic assessment. Among these, 13 were deceased by the time of data collection.
Contact for interview
The remaining 170 potential subjects with schizophrenia spectrum disorders were contacted for a diagnostic interview by using addresses and telephone numbers in Kaiser Foundation Health Plan files or other sources of data, including telephone directories and department of motor vehicle records. Among the 170, 146 (86%) were contacted.
Diagnosis
Potential subjects with schizophrenia spectrum disorder were administered the Diagnostic Interview for Genetic Studies
(15). All subjects provided written, informed consent before administration of the Diagnostic Interview for Genetic Studies. This instrument was administered by a clinician with a minimum of a master’s degree in a mental health-related field, trained to reliability. All psychiatric diagnoses were made with DSM-IV criteria by consensus of three psychiatrists on the basis of a review of the written Diagnostic Interview for Genetic Studies narrative, the medical records, and a discussion with the interviewer. Of the 146 contacted subjects, 107 (73%) completed the Diagnostic Interview for Genetic Studies. The 76 potential subjects with schizophrenia spectrum disorders who could not be interviewed were diagnosed by means of a chart review conducted by experienced psychiatric/psychologic clinicians fully trained in chart review diagnosis.
These procedures yielded a total of 71 subjects with schizophrenia spectrum disorders (for 44 subjects, the diagnosis was determined after the Diagnostic Interview for Genetic Studies; for 27 subjects, the diagnosis was made by chart review). The diagnostic breakdown was: 43 with schizophrenia, 17 with schizoaffective disorder, one with delusional disorder, five with schizotypal personality disorder, and five with other schizophrenia spectrum psychoses (subjects for whom a specific schizophrenia spectrum psychosis diagnosis could not be made).
Data Analysis
The analytic sample
The sample comprised 12,094 subjects who were Kaiser Foundation Health Plan members after December 31, 1980. Seventy-one subjects were ascertained to have a schizophrenia spectrum disorder, and 12,023 subjects were not so ascertained. Because many of the study analyses required data obtained from maternal interviews, those without maternal interview data were excluded, leaving 9,682 subjects. Since siblings represent nonindependent observations, only one sibling per family was included in the analyses. Toward this end, all siblings of subjects with schizophrenia spectrum disorders who did not themselves have a schizophrenia spectrum disorder were excluded from the analyses, and one sibling per family was selected at random from sets of siblings in which the proband did not have a schizophrenia spectrum disorder. Finally, the original group of 71 subjects with schizophrenia spectrum disorders included one set of two siblings from the same family. One of these siblings was excluded from the analytic sample. After these exclusions were applied, a total of 7,793 subjects—70 subjects with and 7,723 subjects without schizophrenia spectrum disorders—remained. For paternal age, data were missing for two subjects with and 82 subjects without schizophrenia spectrum disorders, leaving 68 subjects with and 7,641 subjects without schizophrenia spectrum disorders for the analysis.
Analytic strategy
To examine the association of paternal age at the time of birth and subsequent risk of schizophrenia spectrum disorders or schizophrenia, proportional hazards regression—a type of survival analysis—was used. This method accounts for varying duration of follow-up among subjects and permits adjustment for potential confounding variables. Essentially, proportional hazards regression models the relationship between an exposure and an outcome, where outcome is defined as the time from a well-defined starting point until the occurrence of the outcome of interest, or until the end of observation for subjects without the outcome. In this study, proportional hazards analysis was used to model the relationship between paternal age at the offspring’s birth and the occurrence of schizophrenia spectrum disorders in the offspring. The primary outcome was schizophrenia spectrum disorders; a second set of analyses was performed by using data from the subset of subjects with schizophrenia only. To calculate survival time for either outcome, date of birth was considered the starting point for follow-up. Actual age at onset of disorder was not available for many of the subjects. Age at first treatment or hospitalization for schizophrenia spectrum disorders was substituted for age at onset, since this was reliably ascertained for all subjects with a disorder. Subjects without a diagnosis of schizophrenia spectrum disorders were censored as of their last day of membership in the Kaiser Foundation Health Plan or at the end of study follow-up (Dec. 31, 1997).
The primary exposure variable was paternal age at the time of the offspring’s birth. We examined paternal age first as a continuous measure and then as a categorical measure (to allow for a general, nonlinear effect of paternal age on the logarithm of the rate of schizophrenia spectrum disorders). For the categorical analyses, paternal age was divided into four age categories: 15–24 years (considered to be the referent category), 25–34 years, 35–44 years, and ≥45 years. This scheme afforded natural groupings by decade of age, with the oldest category coinciding with the age for a marked increase in the rate of de novo mutations
(16).
Covariates
Because the correlation between paternal age and maternal age is high, and maternal age has been associated with schizophrenia spectrum disorders in previous work
(3,
5), a primary objective was to rule out confounding by maternal age of the relationship between schizophrenia spectrum disorder risk and paternal age. Like paternal age, maternal age was defined first as a continuous measure, then as a categorical measure. We categorized maternal age into two categories (<30 and ≥30), owing to sample size considerations.
Other covariates selected a priori to be potential confounders included paternal education, paternal race/ethnicity, and parity. Paternal education was defined categorically: less than high school, high school graduate (referent category), some college, or college graduate. Paternal race/ethnicity comprised three groups: white (referent category), black, and other. Parity was treated as a continuous measure. Among these other potential confounders, all were associated with either paternal age and with schizophrenia spectrum disorders, but none were associated with both variables. Thus, the main adjusted analysis included only maternal age as a covariate; however, in the interest of completeness, we also tested a model that included maternal age plus the three additional covariates.
Regression modeling
Proportional hazards regression
(17,
18) was used to analyze the data. This method allowed comparison of the exposure and covariate measurements of each subject at his/her age of first treatment with the average measurements of the population at risk at that time. The population at risk consisted of all subjects who were still Kaiser Foundation Health Plan members and still at risk of failure (diagnosis of schizophrenia spectrum disorders) on the date at which the subject first received treatment. The output from a proportional hazards model includes estimated regression coefficients (interpreted as log rate ratios) and their standard errors for all predictor variables, from which estimated rate ratios, confidence intervals (CIs), and test statistics were generated.
Regression modeling began by fitting paternal age as the only predictor of time until first treatment for schizophrenia spectrum disorders. Subsequent models adjusted for maternal age, and the other covariates were fitted to remove any potential confounding bias in the paternal age effect. When adjusting for maternal age, paternal age and maternal age were consistently defined, i.e., both were treated as categorical or both as continuous in any regression model.
For models with the continuous paternal age variable, the coefficient of paternal age represented the log of the ratio of the rate of schizophrenia spectrum disorders (or schizophrenia) corresponding to a 1-year increase in paternal age. Although the analysis was performed on a continuous variable, we have reported the results in terms of a 10-year increase in paternal age for ease of interpretation. For models that used the categorical paternal age variable, the coefficient for each indicator variable represents the log rate ratio for that category versus the referent category (15–24 years).
Results
Incidence of Schizophrenia Spectrum Disorders
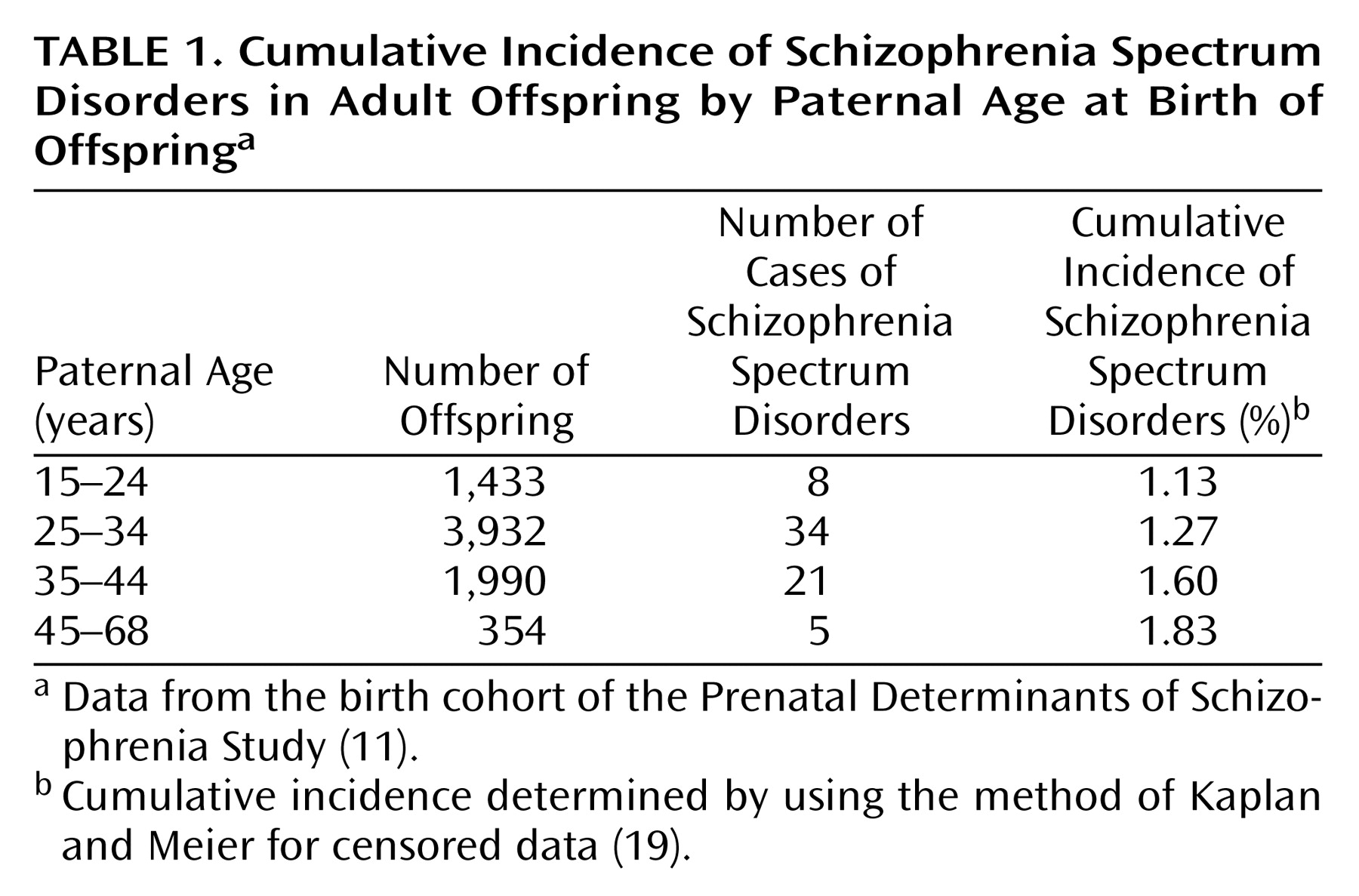
In
Table 1, we report the cumulative incidence of schizophrenia spectrum disorders by father’s age. A graded increase in the cumulative incidence of schizophrenia spectrum disorders (calculated by using the method of Kaplan and Meier for censored data
[19]) is observed with advancing paternal age.
Paternal Age as a Continuous Variable
We first examined paternal age modeled as a continuous variable in relation to risk of schizophrenia spectrum disorders in adult offspring. The analysis revealed a strong trend toward an association between advancing paternal age and risk of adult schizophrenia spectrum disorders. The change in the rate ratio associated with each 10-year increase in paternal age in this unadjusted model is 1.35 (95% CI=0.99–1.83, z=1.93, p=0.053).
In the primary analysis, which adjusted for maternal age, there was a positive and significant association between paternal age and schizophrenia spectrum disorders. The adjusted rate ratio associated with each 10-year increase in paternal age was 1.86 (95% CI=1.20–2.87, z=2.79, p=0.005), indicating nearly twice the rate of adult schizophrenia spectrum disorders in children of men who were 10 years older at the child’s birth, holding all other factors constant. The rate ratio changed only slightly (rate ratio=1.71, 95% CI=0.96–3.07, z=1.82, p<0.07) when adjustment was made for maternal age, paternal education, paternal race/ethnicity, and parity.
Paternal Age as a Categorical Variable
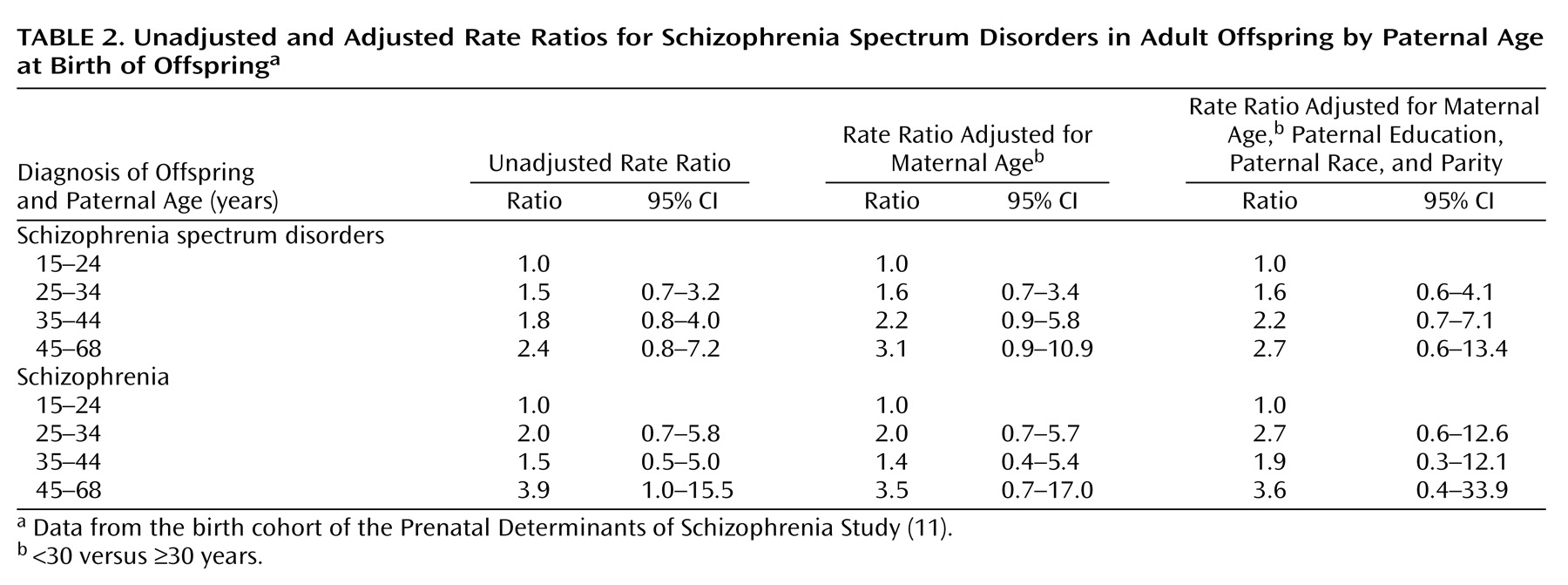
Having demonstrated a positive association between risk of schizophrenia spectrum disorders and increasing paternal age on a continuous scale, we then examined the effect of paternal age on schizophrenia spectrum disorders risk using the aforementioned 10-year age categories. The unadjusted rate ratios for each of these categories, relative to the 15–24-year age group, are presented in
Table 2. There was a steady, monotonic increase in the rate of schizophrenia spectrum disorders with advancing categories of paternal age. The monotonic increase in risk of schizophrenia spectrum disorders with advancing paternal age categories was similar when adjustment was made for maternal age only, and for maternal age, paternal education, paternal race, and parity.
Risk of Schizophrenia
We further examined whether the findings persisted when the outcome was restricted to schizophrenia. For the effect of paternal age, modeled as a continuous variable, on risk of schizophrenia, the unadjusted rate ratio for each 10-year increase in paternal age was 1.41 (95% CI=0.95–2.09, z=1.69, p<0.10). In the analysis adjusting for maternal age, the rate ratio was 1.89 (95% CI=1.08–3.32, z=2.22, p<0.03). Modeled as a categorical variable, paternal age showed a similar dose-related increase for risk of schizophrenia as that found for schizophrenia spectrum disorders (
Table 2).
Discussion
In a prospective birth cohort study, we have demonstrated a relationship between increasing paternal age at the time of the offspring’s birth and the risk of adult schizophrenia spectrum disorders. This effect persisted after adjustment for maternal age, as well as other potential confounders.
Several previous studies have examined the relation between paternal age and schizophrenia. In the Israeli study by Malaspina et al.
(1), the overall pattern and magnitude of the relationship between paternal age and schizophrenia and related disorders was similar to that found in the present investigation, with a relative risk of nearly threefold for paternal age >50 years. That study had many strengths, including a prospective cohort design and large number of subjects with schizophrenia and related disorders. Our study furthers this finding by incorporating several additional methodologic advantages. First, we recorded parental age by direct interview of the mother during pregnancy, rather than relying on varying sources of information, as was done in the earlier study
(1). Second, diagnoses of schizophrenia spectrum disorders were made by using a directly administered, research-based diagnostic assessment complemented by psychiatric records, in contrast to the reliance on hospital registry diagnoses. This permitted us to demonstrate that the association was present for schizophrenia analyzed separately from other schizophrenia spectrum disorders. Third, biological paternity was confirmed in the vast majority of our subjects, and this measure also permitted us to create a data set of independent subjects for analysis. Fourth, our study offered continuous follow-up of the entire cohort, thereby permitting us to define precisely the population at risk at the time each case was first treated. Finally, the replication in a United States birth cohort of the results of the study by Malaspina et al.
(1) adds to the generalizability of the findings.
Our findings are also consistent with those of other earlier studies. Hare and Moran
(2), in England and Wales, demonstrated a significant increase of paternal age in cases of schizophrenia, a finding that persisted despite adjustment for maternal age. Significant increases in paternal age were also found in Ontario
(3) and Sweden
(4) and in a second study in England
(5). However, two earlier studies failed to replicate the association between advanced paternal age and schizophrenia
(20,
21). These earlier studies were limited, however, by the use of clinical case series to derive schizophrenia cases, retrospectively acquired data on paternal age, and no adjustment for potential confounders.
Potential Explanations
We discuss three potential explanations for the observed relation between advancing paternal age and risk of schizophrenia spectrum disorders.
De novo mutations
Advanced paternal age has been associated with major congenital malformation syndromes and isolated birth defects, including Apert’s syndrome
(8), craniosynostosis
(22), situs inversus
(6), syndactyly
(10), cleft lip and/or palate
(9,
23), hydrocephalus
(9), and neural tube defects
(7). Several of these disorders are known to be caused by autosomal dominant mutations.
The most widely accepted proposed mechanism underlying these congenital anomalies is known as the “copy error” hypothesis, first proposed by Penrose
(24). After puberty, spermatocytes divide every 16 days; by age 35, approximately 540 cell divisions have occurred. As a result, de novo genetic mutations resulting from replication errors and defective DNA repair mechanisms are believed to propagate in successive clones of spermatocytes, and these mutations accumulate with advancing paternal age. For the male germ cell line, the mutations are believed to largely consist of single base substitutions
(25).
New mutations may also explain associations between advanced paternal age and some adult-onset disorders, including sporadic Alzheimer’s disease
(26) and cancers of the prostate
(27) and the nervous system
(28). It has been similarly hypothesized that de novo point mutations play a role in the etiology of schizophrenia
(29). If such mutations in the male germ cell line are responsible for the paternal age association with schizophrenia, then this provides one explanation for how this disorder, which has a large genetic component, can be maintained in the population despite reduced reproduction. Excessively mutable single nucleotides in genes critical for brain development or function, such as the fibroblast growth factor receptor 3 gene, may be involved
(30,
31).
Parental constitutional factors
Conceivably, parental constitutional factors, such as schizophrenia spectrum disorders in either of the parents, may also explain the association between increased paternal age and schizophrenia. Previous studies of schizophrenia have demonstrated reduced marriage rates and delayed age at marriage
(32–
35), which may be more prevalent in men than women, and decreased fertility and fecundity
(34–
38), although the latter two findings are disputed
(37). Although studies have generally shown only a 5%–6% morbid risk of schizophrenia spectrum disorders in the parents of subjects with these disorders
(39), others have shown substantially higher risks
(40). It is also possible that the older fathers were more likely to have heritable traits of schizophrenia without meeting diagnostic criteria.
Environmental deprivation
Conceivably, the children of older fathers may undergo higher levels of psychosocial stresses, such as physical illness in the father and/or loss of the father in childhood. In our study, however, it is likely that only a minority of the fathers for whom the age effect on schizophrenia risk was strongest (i.e., those aged >44 years at the time of birth) would have developed serious physical illnesses when their offspring were passing through childhood. There is also no solid evidence that loss of a parent during childhood increases the risk for schizophrenia
(41).
Limitations
There are several limitations of the present study. First, currently there is insufficient information to delineate the relative contributions of biological, genetic, and psychosocial factors to our findings. Data on schizophrenia spectrum disorder diagnoses among the parents and on factors reflecting genetic predisposition to this disorder, including the age of marriage, are necessary to address the hypothesis that confounding by genetic vulnerability to schizophrenia spectrum disorders may explain our finding. This possibility can be at least partially addressed by obtaining data on schizophrenia spectrum disorder diagnoses in relatives of our cohort members, although genetically mediated traits that do not meet the threshold criteria for schizophrenia might prove difficult to assess. Second, because the size of the study group was modest, we were unable to examine the paternal age categories as finely as was done in the study by Malaspina et al.
(1), which included a substantially larger number of subjects. Nonetheless, our results are consistent with those of that study. Third, while the ascertainment for schizophrenia was good, it is likely that a number of cases of schizotypal personality disorder were missed, because only treated cases were ascertained and patients with schizotypal personality disorder are less likely to have been treated. Finally, given the high correlation between paternal and maternal age, it is conceivable that our findings could be explained by factors associated with a greater deviation in ages between the father and mother. However, Malaspina et al.
(1) found a robust effect of paternal age on risk of schizophrenia spectrum disorders after excluding offspring in which the difference between paternal and maternal age was greater than 10 years. Additional research will be necessary to disentangle the effects of paternal age and parental age difference on schizophrenia risk.
Conclusions
We have demonstrated a significant, dose-dependent association between advancing paternal age and risk of schizophrenia and other schizophrenia spectrum disorders in a prospective birth cohort study with several methodologic advantages compared with previous work. The findings persisted after adjustment for maternal age and were present when schizophrenia was examined separately from schizophrenia spectrum disorders. De novo mutations in the male germ cell line may be responsible, at least in part, for the observed association. While further work is necessary to confirm this interpretation, our study nonetheless provides further evidence that advanced paternal age is a risk factor for schizophrenia spectrum disorders. If the de novo mutation hypothesis can be confirmed by future studies, this discovery may lead to the identification of candidate genes for this disorder.