The period from late adolescence to the mid-20s, known as the transition to adulthood, is marked by high rates of major depression
(1). Previous research has demonstrated that youth experiencing depression during this life stage often suffer from significant levels of postdepression dysfunction
(2,
3) and face substantial risk for recurrent depressive episodes in adulthood
(2,
4). It is therefore vital to identify childhood and adolescent predictors so that appropriate prevention and therapeutic programs can be designed to reduce the impact of the disorder before a chronic course is established.
Although prior research has identified multiple childhood and adolescent factors associated with the development of major depression, few studies have focused specifically on predictors of depression occurring in the transition to adulthood. This transition period is a pivotal time in which youth negotiate many developmental tasks, including strengthening and expanding self-concepts, forming stable intimate relationships, making career decisions, and achieving independence from parents
(5). Resolution of these challenges is necessary for the successful assumption of adult roles. However, experiencing major depression may interfere with the acquisition of these skills and lead to poor adjustment in adulthood
(3,
4).
The purpose of this study was to identify childhood and adolescent factors associated with the occurrence of major depression in the transition to adulthood (ages 18–26). The familial and behavioral-emotional domains were selected for study because they have previously yielded potent markers for later depression
(3,
6,
7). In examinations of family characteristics, some studies have indicated that lower socioeconomic status increases the risk for developing major depression
(2,
8), while others have shown an ambiguous association
(3,
9). Aspects of family composition linked to depression include larger family size, later birth order, and older parental age at birth
(7,
10). In addition, family history of psychopathology is an important predictor that may exert its influence through both genetic and environmental pathways
(11). Several indices of family dysfunction, such as conflict, children’s perceptions of being devalued in the family, and family abuse, have been associated with increased risk for depression
(7,
9,
12–14). Behavioral-emotional characteristics include internalizing behavior problems
(15) and anxious or dependent behavior in childhood
(7,
16). Researchers have also found that depressive symptoms are often present several years before the onset of the disorder
(17).
Many studies have documented a significant gender difference in the prevalence of major depression. Starting in adolescence, the proportion of people who experience the disorder is higher for females than for males
(18). Some research, however, has indicated that the gender difference temporarily diminishes in early adulthood
(3,
18,
19).
Finally, there is mounting evidence of the importance of the adolescent period in treating youth vulnerable to depression
(20), and results from intervention trials that have succeeded in forestalling and reducing depressive symptoms in adolescents are encouraging
(21). It is therefore essential to identify high-risk youth to avoid the onset of a potentially chronic cycle of depression
(4).
In light of the critical need to identify factors that place youth at risk for experiencing depression in adulthood, the following research questions were addressed. First, what family and behavioral-emotional factors in childhood and adolescence predict depression from ages 18 to 26? Second, what are the most salient factors from these domains in predicting depression during the transition to adulthood?
Method
In the present analyses we used data from a community-based study that has traced the life course of a single-age cohort from childhood to adulthood. Data were collected from multiple informants, including mothers and participants, at seven major time points: age 5 (1977), age 6 (1978), age 9 (1981), age 15 (1987), age 18 (1990), age 21 (1993–1994), and age 26 (1998). This report focuses on identifying childhood and adolescent predictors (up to age 15) of major depression experienced between ages 18 and 26.
Participants
The 354 participants in these analyses included 170 men and 184 women, almost all of whom (98.0%) were Caucasian. At age 26 they were predominately working or lower-middle class
(22). Most (98.0%) had completed at least a high school education, and 35.9% had 4-year college degrees. Nearly all (90.7%) were employed, with a median income of $25,000. Nearly one-fourth (24.3%) were married, and 20.6% had children.
The original 1977 sample included all youth (50.5% boys) entering kindergarten within one public school system participating in state-mandated preschool testing of developmental, academic, and behavioral factors (N=763). The school district was located in a predominately Caucasian, working-class community in the northeastern United States, and the original sample reflected the composition of the community at that time. Two-thirds of the households were working class or lower-middle class, and nearly all youth were Caucasian (99.3%). Between 1977 and 1998, attrition occurred primarily at the end of kindergarten, when students transferred from the public school system to parochial and private schools. Because data collection occurred within the public schools, those who transferred out of this school system after kindergarten were purposely excluded from follow-up
(23). Overall attrition for the 21-year period was 27.6% of the youth remaining in public schools through grade 3.
The participants at age 26 did not differ significantly from those lost from the initial 1977 group on factors known to be associated with the development of psychiatric disorders. These factors include key demographic, academic, health, and behavioral-emotional characteristics, such as gender (χ2=0.45, df=1, p=0.50), parental socioeconomic status (χ2=2.01, df=1, p=0.73), nurse-rated health (t=0.58, df=700, p=0.56), and mother-rated anxious-depressed behavior (t=1.07, df=725, p=0.29) and attention problems (t=1.24, df=756, p=0.22). These results strongly suggest that the sample was not compromised by selective attrition. After a thorough description of the study at each time point, written informed consent was obtained from the mothers and, starting at age 15, from the participants.
Depression in Transition to Adulthood
The participants were interviewed at ages 18 and 21 by using the National Institute of Mental Health Diagnostic Interview Schedule (DIS), version III, revised
(24), to provide diagnoses of DSM-III-R major depression. They were subsequently interviewed at age 26 with version IV of the DIS
(25) to derive DSM-IV diagnoses. Participants were considered to have depression in the transition period if they met the criteria for major depression between ages 18 and 26 at any of these three assessment points. Administration of the interviewer-rated Global Assessment of Functioning Scale (GAF) (DSM-IV, p. 32) at age 26 provided information about functional impairment.
The DIS has been used in prior community-based studies of psychiatric disorders, and validity studies have shown significant agreement between DIS diagnoses and other measures
(26). This structured interview was administered by graduate-level professionals with clinical and/or research experience. DIS-certified staff conducted a rigorous 2-week training and ongoing monitoring of interviewers. High rates of agreement (98%–99%) were found between the interviewers and staff on practice and in-field interviews over the multiple assessments.
Family Factors
The measures of family factors included demographic information, psychiatric histories of parents and siblings, and indexes of family functioning.
Demographic information, determined from interviews with the mother at age 5, included a measure of family socioeconomic status based on the Hollingshead two-factor index of social position (five categories; 1=highest, 5=lowest)
(22). A family composition index was also constructed and included four interrelated factors (r=0.44 to r=0.68, all p<0.05) present at the time of birth: older mother (30 years or older), older father (35 years or older), larger family size (≥4 children), and being third or later in the birth order.
DSM-III-R major depression and substance use disorders in first-degree relatives, evidenced before the participants were age 15, were determined from combined reports of the mother and the participant at age 26 on the Family History Assessment Module
(27,
28). Combined reports also provided information about whether a parent or sibling had ever been hospitalized for a psychiatric problem or attempted suicide.
Dichotomous measures of family functioning included self-reports of violence (directed toward the participant or between other family members) by age 15 and the occurrence of abuse by parents or siblings. Reports of abuse were based on retrospective accounts during the interview at age 21 of physical or emotional abuse occurring by age 15. The participants’ views of their role in the family at ages 9 (alpha=0.54) and 15 (alpha=0.47) were measured by seven family-related items from the Piers-Harris Children’s Self-Concept Scale
(29), such as “I am a disappointment to my family”
(7). Family cohesion at age 15 (alpha=0.82) was measured by the cohesion subscale of the Family Adaptability and Cohesion Evaluation Scales
(30).
Behavioral-Emotional Characteristics
Reports of childhood and adolescent behaviors were prospectively obtained at ages 9 and 15 and relied on the perspectives of the participants and their mothers.
Participant reports at ages 9 (alpha=0.84) and 15 (alpha=0.83) on the Piers-Harris Children’s Self-Concept Scale provided an index of anxious-depressed behavior. At age 15, depressive symptoms were measured by the Children’s Depression Inventory (alpha=0.85)
(31). The Youth Self-Report was also used at age 15 to gather information about behavior problems
(32). The internalizing (alpha=0.88) and externalizing (alpha=0.86) scales were used.
At ages 9 (alpha=0.73) and 15 (alpha=0.80), mother-rated anxious-depressed behavior was assessed with the Simmons Behavior Checklist
(33). At age 15, the mothers also completed the Child Behavior Checklist
(34), the parent version of the Youth Self-Report, to provide information about internalizing (alpha=0.89) and externalizing (alpha=0.89) difficulties their adolescents had experienced in the past 6 months.
Statistical Analyses
Since previous studies have indicated that pathways to depression may differ for males and females
(3,
35), an initial series of bivariate analyses tested for gender-by-depression interactions in predictors. For factors measured on a continuous scale, two-way analyses of variance with gender and depression as grouping factors were performed, and the F value for the interaction term was evaluated. For dichotomous variables, the Breslow-Day test of homogeneity of odds ratios, in conjunction with the Cochran-Mantel-Haenszel chi-square test, assessed whether associations between predictors and depression differed by gender. No gender interactions were found in these initial analyses. In subsequent bivariate tests conducted to identify family and behavioral-emotional factors associated with depression, gender was included as a control factor in analyses of covariance (for continuous measures) and Cochran-Mantel-Haenszel chi-square tests (for dichotomous indicators). Adjusted odds ratios (controlling for gender) with 95% confidence intervals (CIs) were also computed. Finally, a multivariable logistic regression analysis determined the most salient subset of predictors. Gender interactions were also tested in the regression model.
Results
Prevalence of Major Depression
Two groups were identified on the basis of DSM diagnosis of major depression: 1) participants experiencing major depression between ages 18 and 26 and 2) those who did not have the disorder during this developmental period. Twenty-two participants with bipolar disorder were excluded. We did not, however, exclude participants who had other psychopathology from ages 18 to 26. We were generally interested in identifying markers distinguishing those who experience any major depression during the transition to adulthood from those who do not.
In this sample, 23.2% (N=82) met the diagnostic criteria for depression in the transition to adulthood, while the majority of participants (76.8%, N=272) did not. At age 26, the group with major depression had significantly lower GAF scores than the group without major depression (t=–3.92, df=351, p<0.0001). And in keeping with previous findings
(3,
18), there was no significant difference in the prevalence rates for males and females (21.2% versus 25.0%).
Bivariate Associations
Potential familial and behavioral-emotional predictors of depression were selected from the literature and prior analyses. These candidate predictors and their bivariate associations with depression are summarized in
Table 1 and
Table 2. Twelve significant markers were identified, and all associations were in the theoretically predicted direction.
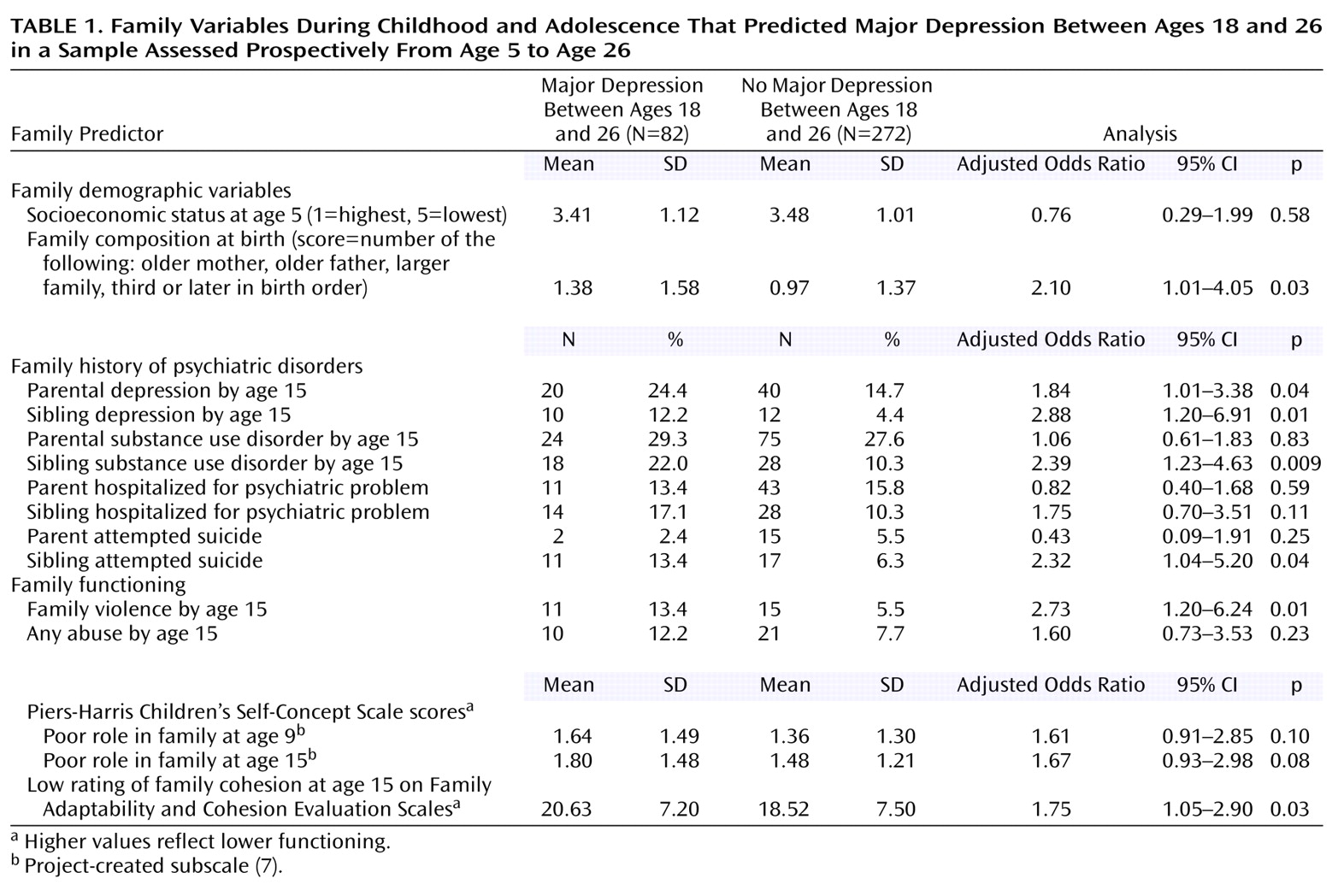
In the family domain (
Table 1), having a depressed parent or sibling was significantly related to experiencing depression in the transition period. Having a sibling with a substance use disorder by age 15 and having a sibling who attempted suicide were also significantly associated with depression. Furthermore, being born into a large family and/or to older parents was a significant risk factor. Self-reports of family violence and low family cohesion were also significant markers.
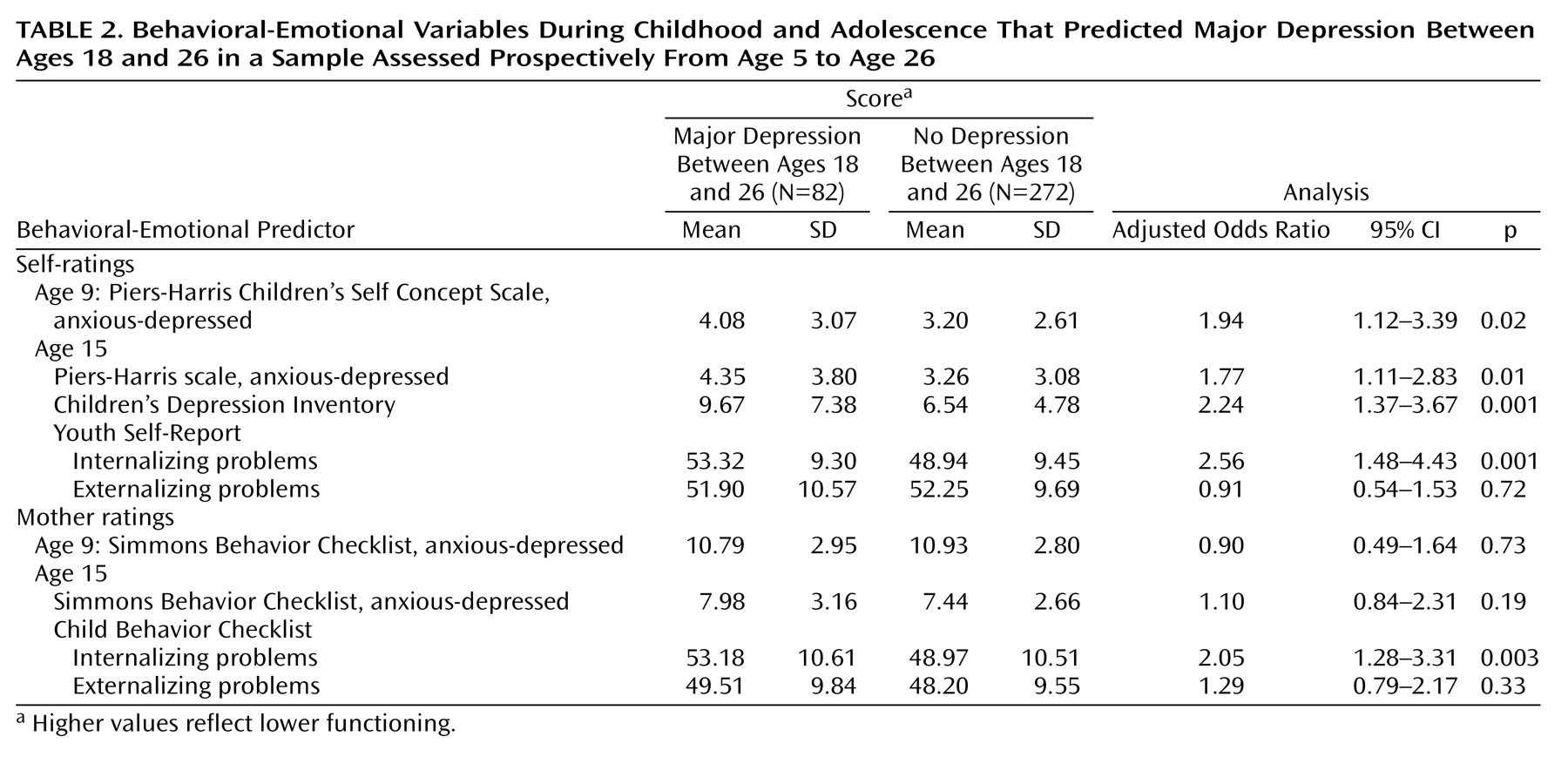
Significant behavioral-emotional characteristics included both participant- and mother-rated internalizing problems at age 15 (
Table 2). Self-reports of anxious-depressed behavior at ages 9 and 15 proved to be significant indicators, as were self-reports of depressive symptoms in midadolescence.
Because of concerns that anxiety and depressive symptoms in midadolescence might be early manifestations of, rather than potential risk factors for, later depression, we reexamined the bivariate associations between depression and the remaining predictors while controlling for the effects of both self-rated anxiety and depressive symptoms at age 15. The adjusted estimates were not attenuated and were of similar magnitude to those found in the unadjusted bivariate analyses. This suggests that self-reported anxiety and depressive symptoms at age 15 were not early manifestations of later major depression, and these variables were therefore included in the subsequent multivariable analyses.
Multivariable Logistic Regression Model
A multivariable analysis was conducted to determine the most salient subset of predictors for experiencing depression between ages 18 and 26. All 12 variables associated with the outcome in the bivariate analyses were considered in a stepwise selection procedure. The final model was obtained by examining individual Wald test statistics for each factor and including only those with p<0.10. Because predictors of depression might be gender specific, interactions of gender with selected factors were also examined. For variables with quantitative scales, the assumption of linearity on the logistic scale was assessed.
Noteworthy predictors from the multivariable analyses included family violence, family composition, self- and mother-rated internalizing problems at age 15, and lower family cohesion. More specifically, participants exposed to family violence by age 15 were approximately four times as likely (odds ratio=3.88, 95% CI=1.56–9.64) to have major depression in the transition period. Also, those with a score of 4 on the family composition index (i.e., older mother, older father, larger family size, and later in birth order) were almost three times as likely (odds ratio=2.73, 95% CI=1.29–5.81) to meet the criteria for major depression as were adolescents with a score of 0. Both the self- and mother-based ratings of internalizing problems (on the Youth Self-Report and Child Behavior Checklist, respectively) were significant predictors. Participants who were approximately 1 SD (or 10 units) above the mean for internalizing problems were twice as likely (Youth Self-Report: odds ratio=2.00, 95% CI=1.08–3.64; Child Behavior Checklist: odds ratio=2.00, 95% CI=1.29–3.96) to meet the criteria for the disorder as were participants whose scores were 1 SD below the mean. Last, the adolescents who scored approximately 1 SD above the mean (or 7.5 units) on the measure of lack of family cohesion were nearly twice as likely (odds ratio=1.70, 95% CI=0.97–3.07) to meet the criteria for depression as were those scoring 1 SD below the mean.
Discussion
Major depression occurring in the transition to adulthood may curtail the attainment of occupational and interpersonal developmental tasks appropriate for full adult status. The manifestation of depression during this period creates heightened risk for recurrence
(36) and has negative implications for subsequent functioning
(2,
3).
In the current study, multiple childhood and adolescent predictors clearly identified participants who experienced depression in the transition period. These distinct profiles point to avenues for prevention and early intervention, particularly during the critical adolescent “window of opportunity”
(20). This concept, originally applied to depressed adolescents, can be expanded to include youth who exhibit early warning signs of later depression and are in need of early clinical intervention.
This study highlights the importance of both biological-genetic and environmental factors in the family domain. Parental and sibling depression and sibling substance use disorders manifested by the time the participants reached age 15 point to the strong role of biological and genetic factors. Yet the family violence and lack of cohesion characterizing the households of the depressed respondents confirmed the interaction of familial psychopathology within a dysfunctional family environment. Such findings have been documented in prior studies
(6,
36–38).
The importance of family composition at birth reflects earlier findings with our community group
(3). Other researchers have found that later-born children in large families report estrangement from parents and perceive their families as punitive and unsupportive
(39). Later-born children are also at risk for depression, anxiety, and lower self-concept
(10).
As early as age 9, the respondents who later experienced depression rated themselves as more anxious and depressed than their peers. At age 15, moreover, both adolescents and mothers reported those in the depression group as having more internalizing behavior problems. In midadolescence, those depressed between 18 and 26 also self-reported significantly higher levels of depressive symptoms, an important precursor of subsequent major depression
(17).
The most salient predictors emerging from the multivariable analyses again highlight the strong influence of the family milieu. The likelihood of being depressed from ages 18 to 26 was four times as high if family violence was reported by age 15. Thus, a chaotic and unsafe family environment in adolescence was most important in predicting depression during the transition to adulthood. Internalizing problems emerged as the most prominent behavioral-emotional factor. The finding that both adolescents and mothers reported internalizing problems is important to note as clinicians seek to identify adolescents in need of early intervention.
The ability of adolescents to reflect on their own inner distress as well as report on negative aspects of their family milieu can serve to alert physicians, educators, and other adults to their vulnerability. This developmental readiness to communicate affective states bodes well for both the identification of vulnerable youth and their readiness for interventions, opening windows of therapeutic opportunity
(20).
There is general agreement that active depression can be effectively treated by both medication and psychosocial treatment
(40,
41). Increasingly, however, cognitive-behavioral preventive interventions have targeted youngsters with early symptoms of depression
(42,
43). Outcomes of these interventions have included symptom reduction and improved functioning
(43–
45). Positive results have also been reported for family-centered preventive programs targeting high-risk offspring of depressed parents
(40). The emergence of potentially efficacious therapeutic interventions makes early identification of vulnerable youth more compelling.
In interpreting the results of this study, several limitations should be considered. First, because the cohort is from a predominately Caucasian, working-class community, our findings may not be generalized to more racially and economically diverse populations. Second, whereas the use of multiple statistical comparisons may have increased the risk for type I error, the small number of subjects in the diagnostic group may have increased the risk for type II error. The strengths of the study, however, include the prospective nature of data gathered from childhood to adulthood in a single-age cohort. Repeated administration of standardized instruments from multiple informants over 20 years offers a perspective few studies can match.
In summary, major depression occurring in the transition to adulthood has the potential of resulting in chronicity and impaired functioning later in adult life. It is therefore important to identify, treat, and monitor youth who express anxiety and depressive symptoms in adolescence
(36). Our findings suggest clear markers apparent in childhood and adolescence, presenting opportunity to those working with and treating this population. The identification of these predictors provides an ideal moment to break the cycle of psychopathology.