A review of structural magnetic resonance imaging (MRI) studies in schizophrenia noted that all studies that specifically examined gray matter of the superior temporal gyrus showed volume reductions, suggesting that the superior temporal gyrus may be a fundamental abnormality in schizophrenia
(1). Studies of schizophrenic subjects may be difficult to interpret, given the potential effects of neuroleptics on MRI volumes measured
(2). The study of alternate subject groups free of the confounds of medications, such as subjects with schizotypal personality disorder
(3,
4), has been helpful in defining important MRI abnormalities. Our laboratory previously reported smaller left superior temporal gyrus volumes in male subjects with schizotypal personality disorder
(5), reinforcing the hypothesis that smaller superior temporal gyrus volumes were key to the development of schizophrenia spectrum disorders.
This MRI study examines the superior temporal gyrus in female subjects with schizotypal personality disorder recruited from the community and age-matched comparison subjects. If the hypothesis is correct that a gray matter abnormality in the superior temporal gyrus is critical to the development of schizophrenia spectrum disorders, then female subjects with schizotypal personality disorder should also exhibit this abnormality. However, if the potential ameliorating effect of gender is strong, then superior temporal gyrus abnormalities may be attenuated or not present.
Results
Subject Demographics
One-way ANOVA revealed no difference between the women with schizotypal personality disorder and the healthy women in terms of age (mean=28.4 years [SD=8.1] and 30.4 years [SD=9.2], respectively; F=0.61, df=18, p=0.44), IQ (mean=115.6 [SD=10.6] and 119.5 [SD=9.4]; F=1.83, df=1, 47, p=0.18), or parental socioeconomic status (F=0.21, df=1, 48, p=0.65). Despite the similar IQ, however, subjects with schizotypal personality disorder completed fewer years of education (mean=15.1, SD=1.9) than did the healthy subjects (mean=16.4, SD=1.6) (F=7.69, df=1, 48, p=0.008) and had a lower socioeconomic status (F=14.8, df=1, 48, p<0.0009).
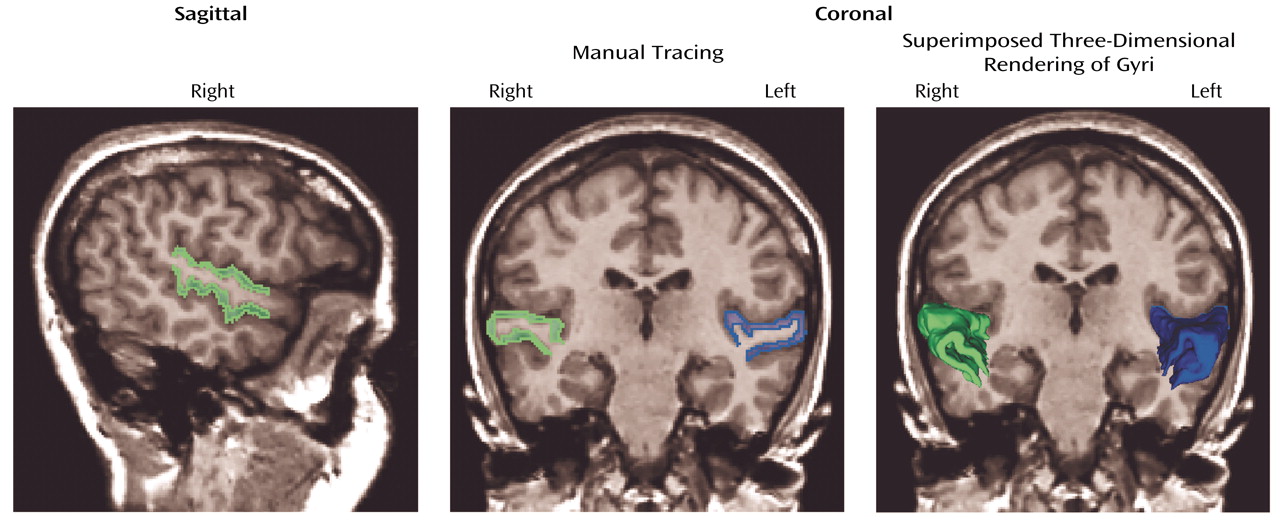
Superior Temporal Gyrus Measures
ANOVA with the repeated measure of hemisphere revealed no main effect of side (F=0.102, df=1, 48, p<0.76; effect size [η
2]=0.002) or interaction effect between diagnostic group (schizotypal personality disorder versus comparison) and hemisphere (F=0.785, df=1, 48, p=0.38; η
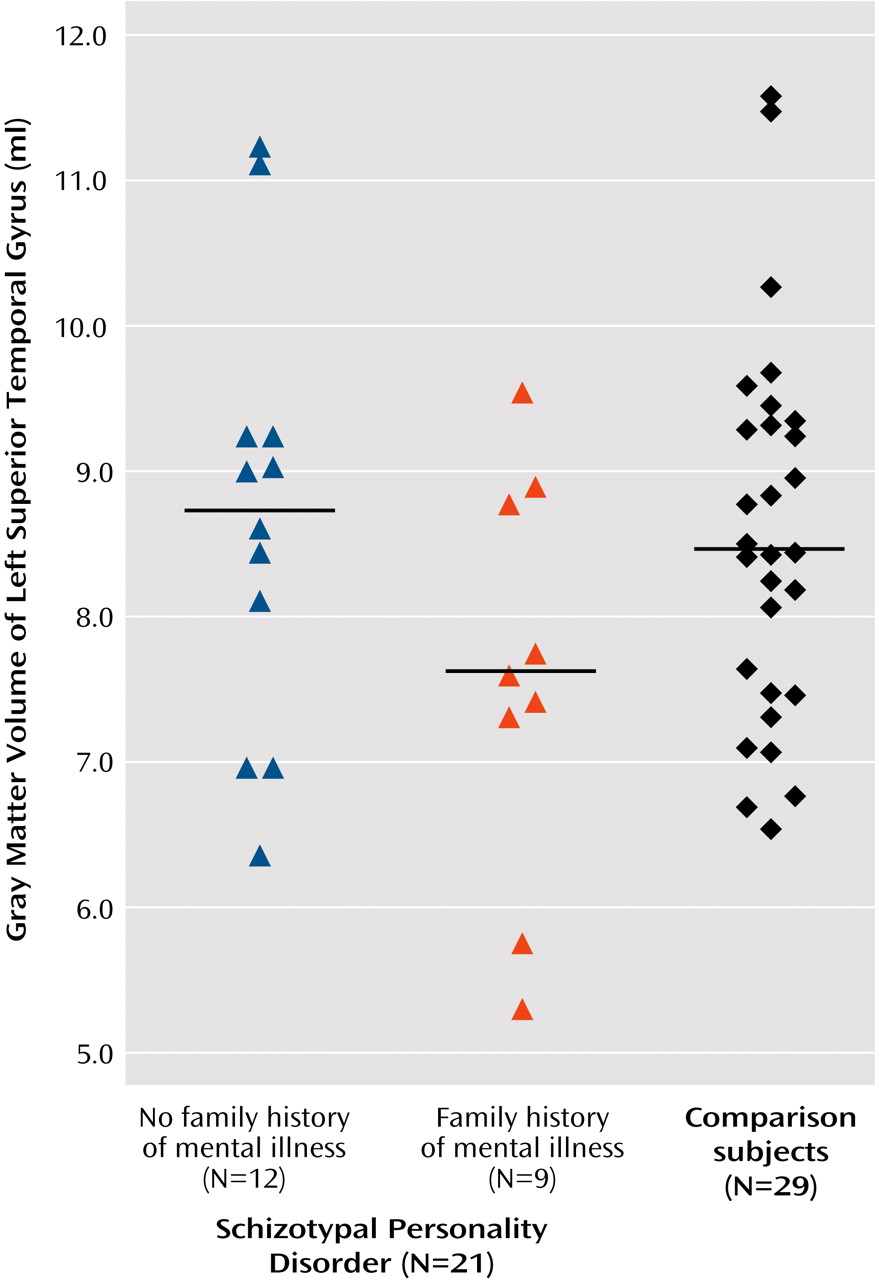
2=0.016). Within the schizotypal personality disorder group, ANOVA with repeated measures of hemisphere revealed no main effect of hemisphere (F=1.8, df=1, 19, p<0.20; η
2=0.09), but there was an interaction effect for hemisphere and family history (F=5.1, df=1, 19, p<0.04; η
2=0.21). Follow-up one-way ANOVA for each hemisphere separately revealed a difference that approached significance for the left superior temporal gyrus gray matter (F=3.276, df=1, 19, p<0.09; η
2=0.15) but not the right superior temporal gyrus gray matter (F=0.26, df=1, 19, p<0.62; η
2=0.014). Paired t tests on left–right superior temporal gyrus volumes within those subjects with schizotypal personality disorder and a family history of mental illness revealed a difference (t=–2.313, df=8, p<0.05) that was not present in those subjects without a family history (t=0.721, df=11, p<0.49) (
Figure 2).
Clinical/Cognitive Characteristics Correlated With Superior Temporal Gyrus Measures
For the subjects with schizotypal personality disorder, there was a statistically significant negative correlation between the degree of impairment due to odd speech assessed by the interviewer (one of the criteria for diagnosis of schizotypal personality disorder) and volume of the left superior temporal gyrus (rs=–0.46, p<0.04). There was no correlation between Thought Disorder Index scores and superior temporal gyrus volumes, although the Thought Disorder Index score was elevated (mean=26, SD=23.1).
Discussion
This report examining a group of female schizotypal personality disorder and comparison subjects found that, contrary to predictions, the schizotypal personality disorder group did not show volume abnormalities in the superior temporal gyrus. This is not due to insufficient study group size, given the small effect size. To our knowledge, this is the first MRI study that has focused specifically on female schizotypal subjects.
Within the schizotypal personality disorder group, there was left-right difference in superior temporal gyrus volumes in those subjects with a positive family history of mental illness and a tendency for the left superior temporal gyrus gray matter volume to be smaller that was not present in those subjects who did not have a family history of mental illness. Note that the number of subjects in these two groups are small, so the data must be interpreted in that light. Moreover, most of the subjects reported a first-degree relative with affective disease, not schizophrenia, but that might be expected to dilute the finding. However no independent confirmation was available. It is possible that some of these relatives may have had comorbid schizotypal personality disorder, given the high rates of comorbidity
(9). Nonetheless, it may be that female subjects with schizotypal personality disorder and a positive family history of major mental illness may have anatomical features similar to male subjects with schizotypal personality disorder.
Of note, however, subjects with schizotypal personality disorder with more odd speech had more reduced left superior temporal gyrus volumes. The qualities of the odd speech by definition include speech that is vague or overinclusive. In addition, pilot data suggested that female subjects with schizotypal personality disorder demonstrate formal thought disorder.
These results point to a neuroanatomical difference between male and female subjects with schizotypal personality disorder, since male subjects demonstrated frank superior temporal gyrus abnormalities
(4,
5) whereas female subjects did not. This finding suggests that the interaction between gender and disease may play a pivotal role in the generation of abnormal brain morphometry and clinical symptoms in the schizophrenia spectrum. Similar to our data, Gur et al.
(10) demonstrated gender differences in the superior temporal gyrus in schizophrenic subjects, with female subjects exhibiting normal volumes. Bryant et al.
(11) showed a gender effect for the whole temporal lobe for male schizophrenia subjects who had reduced volumes compared with male comparison subjects, but no difference between female schizophrenia subjects and their gender-matched comparison subjects. No gender effect on superior temporal gyrus was noted, however, in that publication, although as the authors noted themselves, gray and white matter were not analyzed separately, which many consider key for the evaluation of this brain region
(1). Some of the differences in findings also may be due to the overlap of volumes between subject groups and inherent measuring difficulties due to greater variability in the surface morphometry of the superior temporal gyrus in schizophrenic subjects relative to comparison subjects
(12). Moreover, the effect of gender on the volume of superior temporal gyrus is not clear. Even within healthy nonpsychiatric populations, some investigators report a main effect of gender on the superior temporal gyrus
(13) while others do not, when using surface-based modeling approaches
(14), or when using semiautomatic volume measures
(15). Nonetheless, the current data and clinical data suggest that there is heterogeneity within the schizophrenia spectrum and that gender appears to be a critical factor in producing divergence.
Although the superior temporal gyrus was of normal volume in this group of female subjects with schizotypal personality disorder, it may not be functioning normally, as evinced by the correlation with odd speech. Functional MRI studies of this population may be an intriguing way of testing this hypothesis.