It is estimated that somewhere between 200,000 and 1,000,000 Americans make nonfatal suicide attempts each year
(1). Because of the magnitude of the problem, the Surgeon General outlined a plan that called for the identification of populations at high risk for suicidal behavior, the enhancement of intervention programs and services, and the advancement of relevant scientific methods
(2). In accordance with the Surgeon General’s recommendations to identify specific high-risk populations, the present investigation focuses on multiple suicide attempters (individuals who have made two or more suicide attempts in their lifetimes) as a unique group, distinct from single suicide attempters (individuals who have made one lifetime suicide attempt). Although investigators have tended to place all suicide attempters into a single category, several lines of research have begun to emerge that suggest that there are important differences between multiple suicide attempters and single suicide attempters.
Rudd et al.
(3) provided some of the clearest findings on the topic to date. They compared 68 multiple suicide attempters to 128 single suicide attempters (and to 134 suicide ideators) and found that multiple suicide attempters displayed elevated suicidal ideation, depression, hopelessness, and perceived stress, as well as poorer social problem-solving skills. Additionally, multiple suicide attempters had a greater number of axis I diagnoses, as well as an earlier onset of the first psychiatric disorder. In related work conducted in Canada, Reynolds and Eaton
(4) compared 364 single suicide attempters to 99 multiple suicide attempters (defined as three or more attempts). They found that multiple suicide attempters were more likely to have had family histories of suicidal behavior, showed poorer coping histories, and demonstrated a longer duration of psychiatric symptoms, alcohol and drug abuse, and depression. Differences between multiple suicide attempters and single suicide attempters also have been found in adolescent populations, with multiple suicide attempters consistently demonstrating greater levels of psychopathology
(5–
7).
The purpose of the present research was to replicate and extend previous work on adult multiple suicide attempters by examining a group of recent suicide attempters. In accordance with previous findings, it was predicted that multiple suicide attempters would exhibit greater severity of psychopathology (depression, hopelessness, substance abuse, psychosis, and number of axis I diagnoses), suicidality (ideation, intent, lethality, and reaction to attempt), and interpersonal deficits than single suicide attempters. The present study extends previous work in several important respects, such as by using a group that is more representative of the typical adult suicide attempter seen in urban psychiatric settings in the United States. The study by Rudd et al.
(3) included only young adults on active duty in the military who had no psychotic disorders or serious substance abuse problems. The present group of suicide attempters was obtained from a large urban hospital and included virtually all individuals between ages 18 and 65 who entered the emergency room within 48 hours of making a suicide attempt, including those with psychosis or substance abuse problems. Second, the present study included an expanded range of variables on which multiple and single attempters could be compared. Third, the current study allowed for the examination of differences between multiple and single suicide attempters, with control for a diagnosis of borderline personality disorder. If differences between multiple suicide attempters and single suicide attempters emerge even when borderline personality disorder status is controlled, then the importance of considering multiple suicide attempters as a unique subgroup of individuals is heightened.
Replication and extension of this research is important because the identification of multiple suicide attempters is a potentially powerful clinical tool that has not yet been well developed. If the findings are replicated, the status of multiple suicide attempters could function to represent an important general marker of serious behavioral dysfunction in a broad number of domains. In contrast to many other psychiatric classifications (such as a diagnosis of borderline personality disorder) that are complex, time-intensive, and frequently unreliable
(8,
9), the assessment of whether or not a patient has made multiple suicide attempts is a simple behavioral indicator that can be readily assessed. Of great clinical use would be the ability to quickly and consistently identify a subpopulation of suicidal patients who are particularly likely to be experiencing high levels of psychopathology, are at high risk for future suicidal behaviors, and are in strong need of focused clinical attention.
Discussion
Building on prior work
(3,
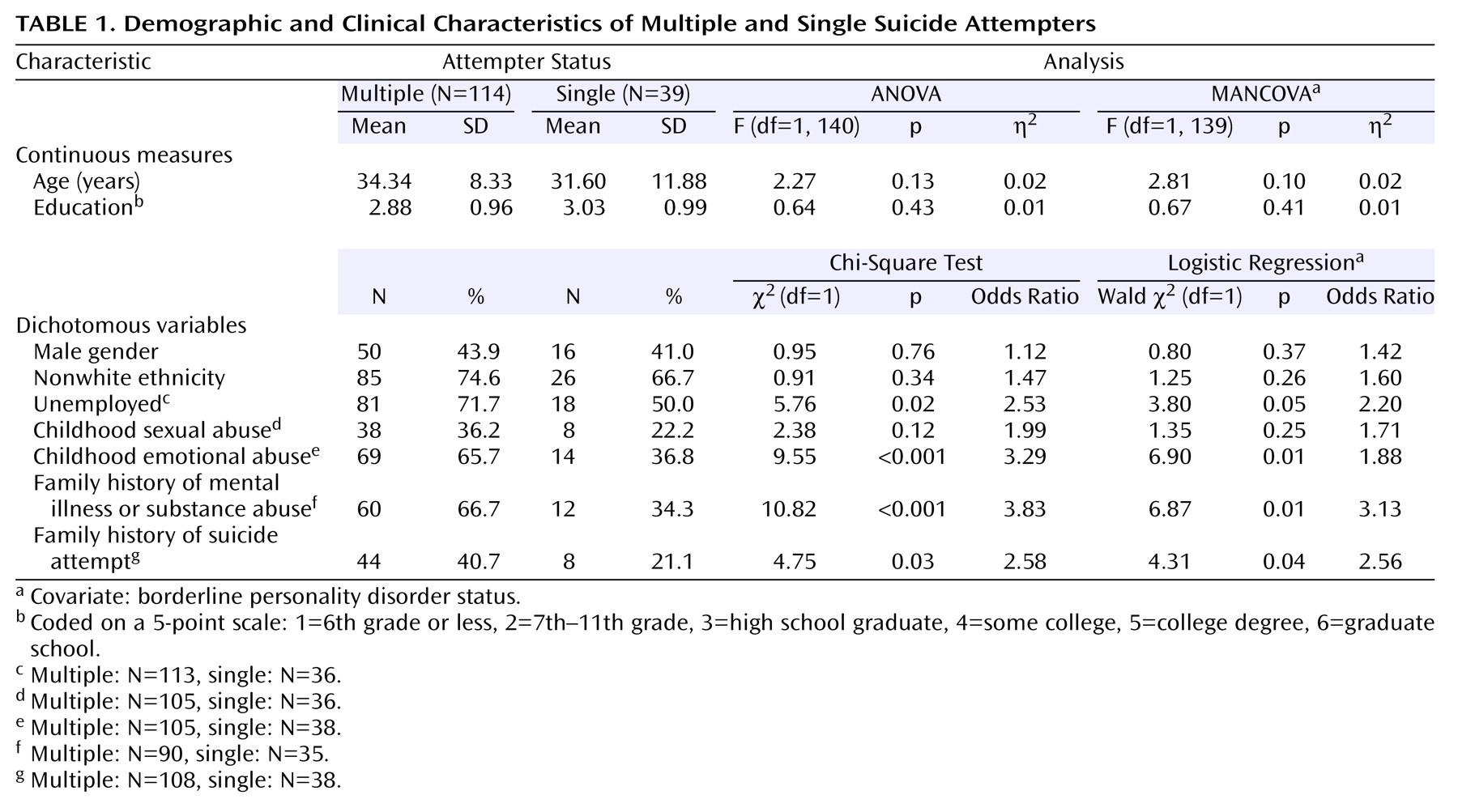
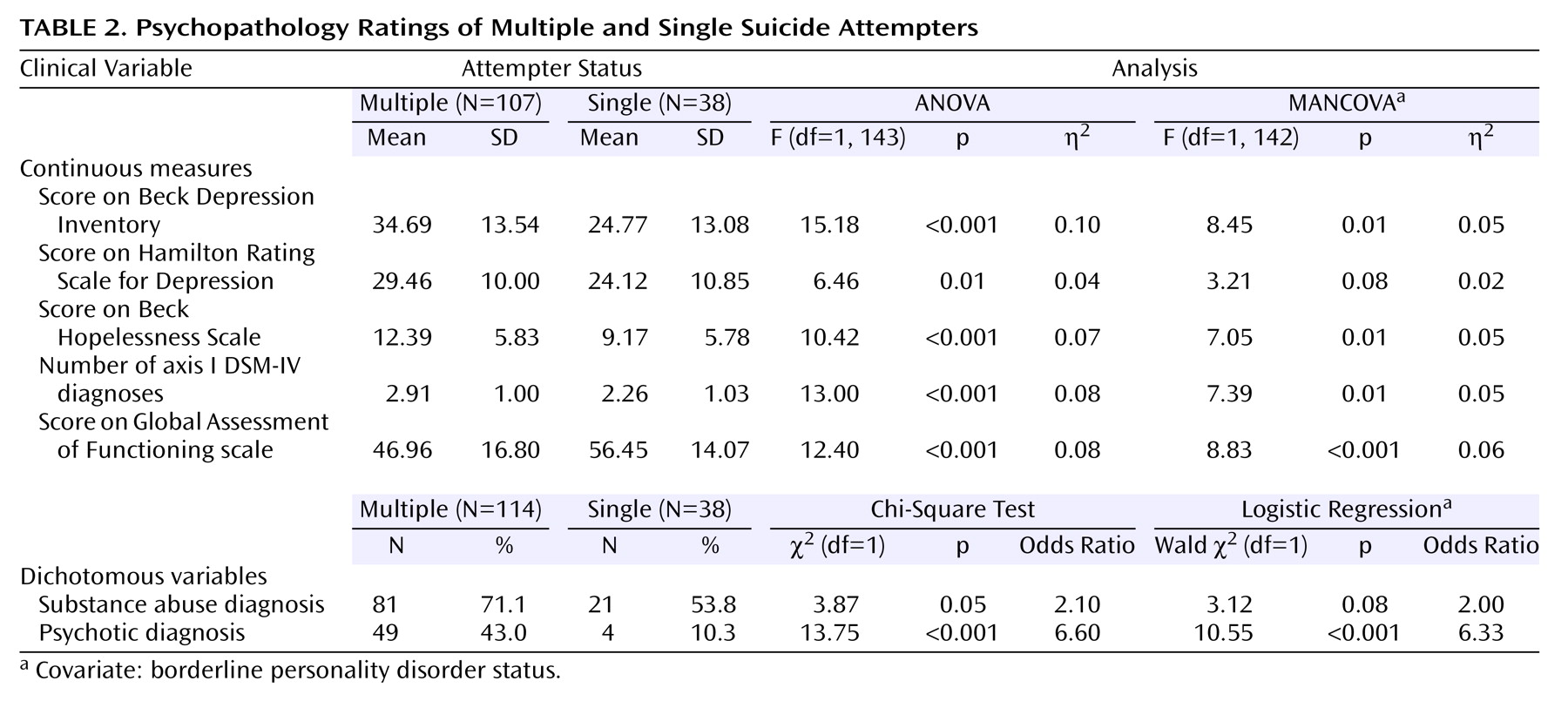
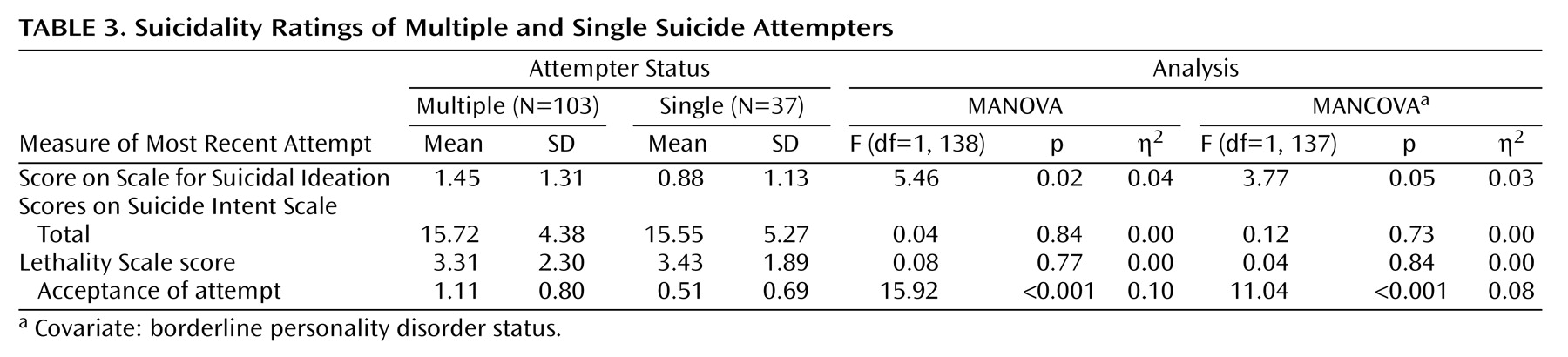
4), we predicted that crucial differences would emerge in the clinical profiles of single suicide attempters versus multiple suicide attempters. Our findings strongly support this prediction. As compared to single suicide attempters, multiple suicide attempters displayed higher levels of depression and hopelessness, met criteria for more DSM-IV axis I diagnoses, were at a particularly high risk for being diagnosed with substance abuse and psychotic disorders, were more likely to be diagnosed with borderline personality disorder, and were rated as having poorer global functioning in the year before their suicide attempt. Multiple suicide attempters also displayed greater suicidal ideation and had a more accepting attitude toward their suicide attempts, although the degree of suicidal intent and the lethality of the attempts were not found to be higher. Multiple suicide attempters were more likely to be unemployed and had poorer social problem-solving skills and more relational difficulties. Multiple suicide attempters also were more likely to report having experienced emotional abuse as children and having family members with histories of mental illness and suicide. Additionally, no significant differences emerged between multiple suicide attempters and single suicide attempters in terms of age, gender, education, and ethnicity, suggesting that the importance of multiple attempt status holds across various demographic subpopulations. Moreover, the findings largely held when we controlled for a diagnosis of borderline personality disorder; thus, multiple attempter status is not simply a marker for borderline personality disorder.
It is important to note that when they were compared to the general population, single suicide attempters display greater psychopathology and dysfunctionality than nonattempting ideators
(3). However, the magnitude and robustness of the differences between the multiple suicide attempters and the single suicide attempters are striking and support the premises that those with histories of multiple attempts should be considered as a unique subgroup of suicide attempters and that this behavior represents a behavioral marker for particularly impaired functionality across a broad number of domains.
Study findings suggest further avenues for investigation and have implications for both theory and treatment. A particularly important conclusion that can be drawn from this and prior studies is that repeated instances of nonlethal suicidal behavior should not be dismissed as nonserious or of no consequence. Rather, this behavior is indicative of particularly severe psychopathology and of high risk for future suicidal behavior. In terms of theory, researchers should begin to focus on understanding the causal nature of the relationship between psychopathology and multiple attempt status, i.e., whether high levels of psychopathology tend to cause people to make repeated suicide attempts, whether the reverse is true, or whether the relationship is, in fact, transactional.
The finding that multiple suicide attempters are more than four times as likely as single suicide attempters to have a psychotic diagnosis, while not inconsistent with previous findings
(30), is striking and bears further discussion. In this group, nearly all psychotic diagnoses are mood-related (i.e., major depressive, bipolar, and schizoaffective disorders). Thus, it might be hypothesized that the powerful link between psychotic diagnosis and attempt status is simply because those receiving the psychotic diagnoses are much more depressed. However, a post hoc analysis of the data revealed that the association remains strong, even after control for the level of depression. One possibility is that psychotic symptoms (e.g., hallucinations) produce misery and suffering that increase the likelihood of a suicide attempt.
Beck’s theory of modes
(31) offers a theoretical framework for conceptualizing repeated suicidal behavior in cognitive terms. Modes are defined as interconnected networks of cognitive, affective, motivational, physiological, and behavioral schemas that are activated simultaneously by relevant environmental events and result in goal-directed behaviors. When the suicidal mode is activated, individuals experience suicide-related cognitions, negative affect, and the motivation to engage in suicidal behavior
(32). When an individual repeatedly engages in suicidal behavior, the suicidal mode becomes highly accessible in memory and requires minimal triggering stimuli to be activated
(33).
In terms of treatment, the different clinical profiles of multiple suicide attempters and single suicide attempters suggest potentially different treatment regimens. Effective interventions for multiple suicide attempters should focus on decreasing hopelessness, depression, suicidal ideation, and acceptance of attempt behavior and increasing social problem solving, general relational skills, and appropriate use of other social and medical services. Moreover, clinicians can facilitate multiple suicide attempters’ understandings of triggering internal and external events as well as the key cognitions occurring at the time of the attempts, thus potentially deactivating the suicidal mode and averting self-destructive behavior. Interventions of these types already exist
(10,
34,
35), and preliminary results of clinical trials have demonstrated success in decreasing subsequent suicide attempts
(35–
37). As important differences between multiple suicide attempters and single suicide attempters continue to be delineated in future research, especially in terms of developmental origins, interventions can be further tailored to the unique clinical profile of multiple suicide attempters as well as toward prevention of future suicidal behavior.
A number of study limitations should be considered in evaluating the findings discussed. First, the group was constrained in terms of suicide status (all were recent attempters) and by virtue of self-selection (only those who agreed to participate in a larger treatment outcome study), perhaps limiting generalizability. Additionally, as noted by other authors
(3), categorizations of multiple versus single attempters represent a single point in time, and some unknown portion of the single attempter group will become multiple attempters. Future research goals might include determining the stability of the single attempter group and identifying factors that predict which individuals become multiple attempters. A related issue concerns the question of whether attempter status is better conceived of as a continuous versus a categorical variable. While simply dividing individuals into single and multiple attempters has been demonstrated to be a powerful assessment tool, it is quite possible that dividing the population of attempters into more finely grained groups would be useful (e.g., single, double, and triple or more). Overall, an understanding of the multiple attempt group would be greatly enhanced by future research that makes use of longitudinal data enabling the exploration of causal relationships between attempt status and psychopathology, interpersonal functioning, and suicidal thoughts and behavior. Our research team is currently following this group of suicide attempters in an attempt to shed light on these questions.
In conclusion, the current study demonstrates that individuals with histories of multiple suicide attempts have a particularly severe clinical profile characterized by an extremely high degree of psychopathology, suicidality, and interpersonal dysfunction. As such, multiple attempters are likely to be at high risk for future suicidal behavior and are in great need of clinical intervention. On this basis, we argue that an essential element of suicidal assessment should be a history of multiple suicide attempts versus a single attempt. This simple, easy to assess variable can then be used to help guide risk assessment, case conceptualization, treatment planning, and intervention design and refinement.