The growing incidence of suicidal acts among prisoners
(1) and jail detainees
(2) has heightened awareness of the risk for suicide among persons characterized by criminal, aggressive, and substance abuse behaviors. The importance of these “externalizing” syndromes, as well as of “internalizing” forms of psychopathology such as depressive disorders, in predicting suicide is well established
(3–
5). Most research examining suicide risk among individuals who exhibit externalizing syndromes has been conducted with forensic or psychiatric patients
(6,
7). Although these subjects are often ideal for studies that examine extreme behaviors, their inclusion impedes disentangling the effects of incarceration or acute institutionalization from more stable underlying processes that place these persons at risk for suicide
(8). Even in community samples, the risk for suicide among persons exhibiting acting-out behaviors may simply reflect risk associated with the comorbidity of such behaviors with an internalizing axis I disorder, such as depression
(9,
10).
Mounting evidence supports the supposition that externalizing psychopathology represents a key risk factor for suicide. In this regard, Apter and colleagues
(7,
11) identified at least two subtypes of individuals with suicidal behaviors: depressed/withdrawn and irritable/aggressive. They found that among violent male patients and adolescents with conduct disorder, sadness did not correlate with suicidal behavior. On the other hand, the correlation between depression and suicidal acts was significant for nonviolent hospital patients and adolescents with internalizing syndromes
(7,
12). Although major depression is an important precipitant, suicide risk among individuals with externalizing disorders may instead be related to impulsive and anger-related behaviors. Despite this evidence, a few issues prevent firm conclusions about the roles of internalizing and externalizing psychopathology in suicidal behavior. First, in the studies just discussed, the study groups were composed of psychiatric patients, and we wanted to examine whether these relationships could be found in the general population. Second, prior research has not statistically controlled for depressive symptoms, or comorbidity between internalizing and externalizing disorders, in analyzing the relationship between externalizing disorders and suicidal behavior. Finally, few authors have examined gender differences in the effect of internalizing and externalizing disorders and their co-occurrence on suicidal behaviors in a large group of men and women from the community.
The high rate of comorbidity among mental disorders is relevant to the understanding of risk for suicide in different diagnostic groups. Epidemiological data support the high rate of comorbidity among depressive and anxiety disorders
(13,
14), as well as the co-occurrence of externalizing symptoms (including antisocial and criminal behaviors, excessive alcohol use, and aggressive acting out) within individuals
(15–
18). Krueger
(19) suggested that these patterns of comorbidity represent meaningful covariance. Specifically, he validated a two-factor model of common mental disorders (i.e., not including schizophrenia and bipolar disorder): an internalizing factor representing mood and anxiety disorders and an externalizing factor that included antisocial personality disorder and alcohol and other substance dependence. This dimensional model suggests that each factor (or cluster of related disorders) represents a common underlying process of psychopathology
(20,
21).
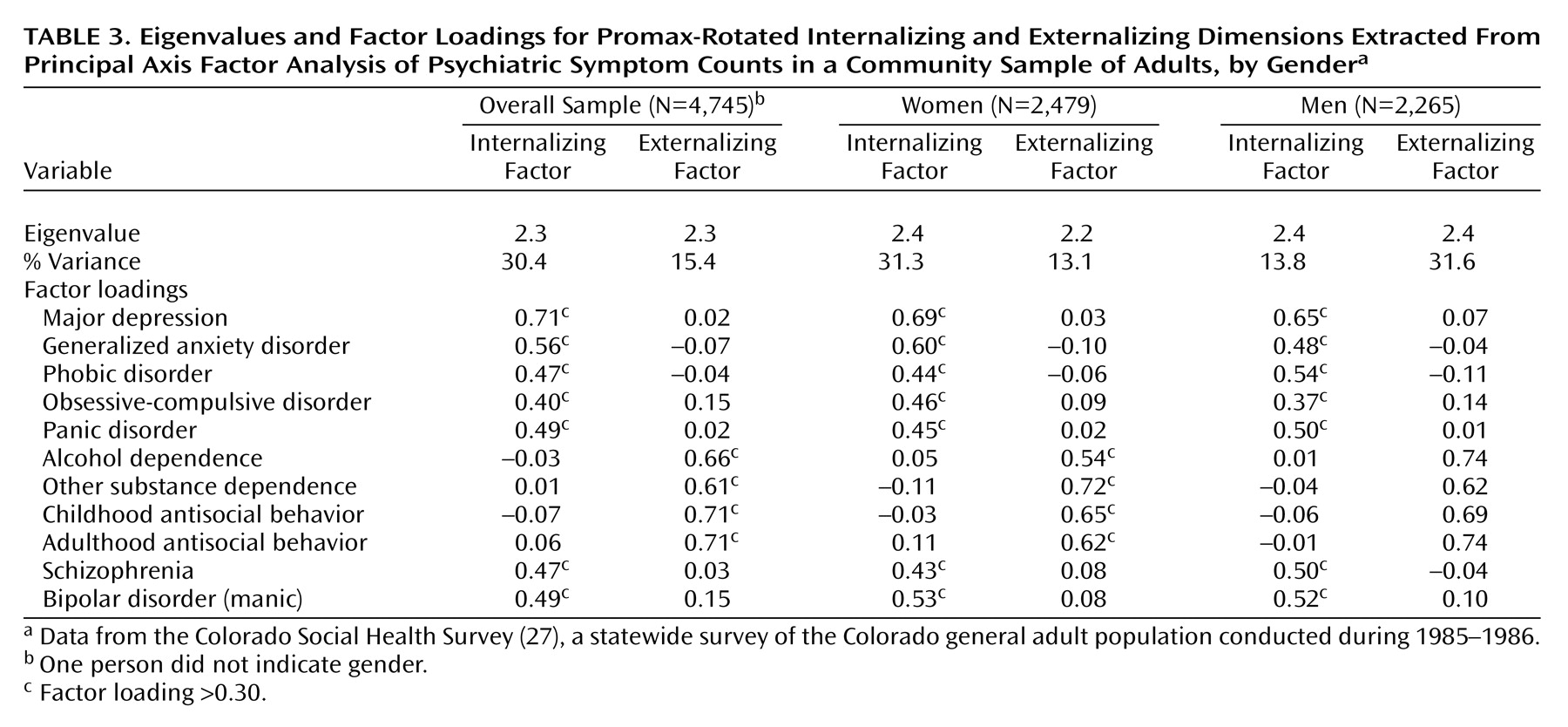
Although some controversy exists in the interpretation of Krueger’s analyses
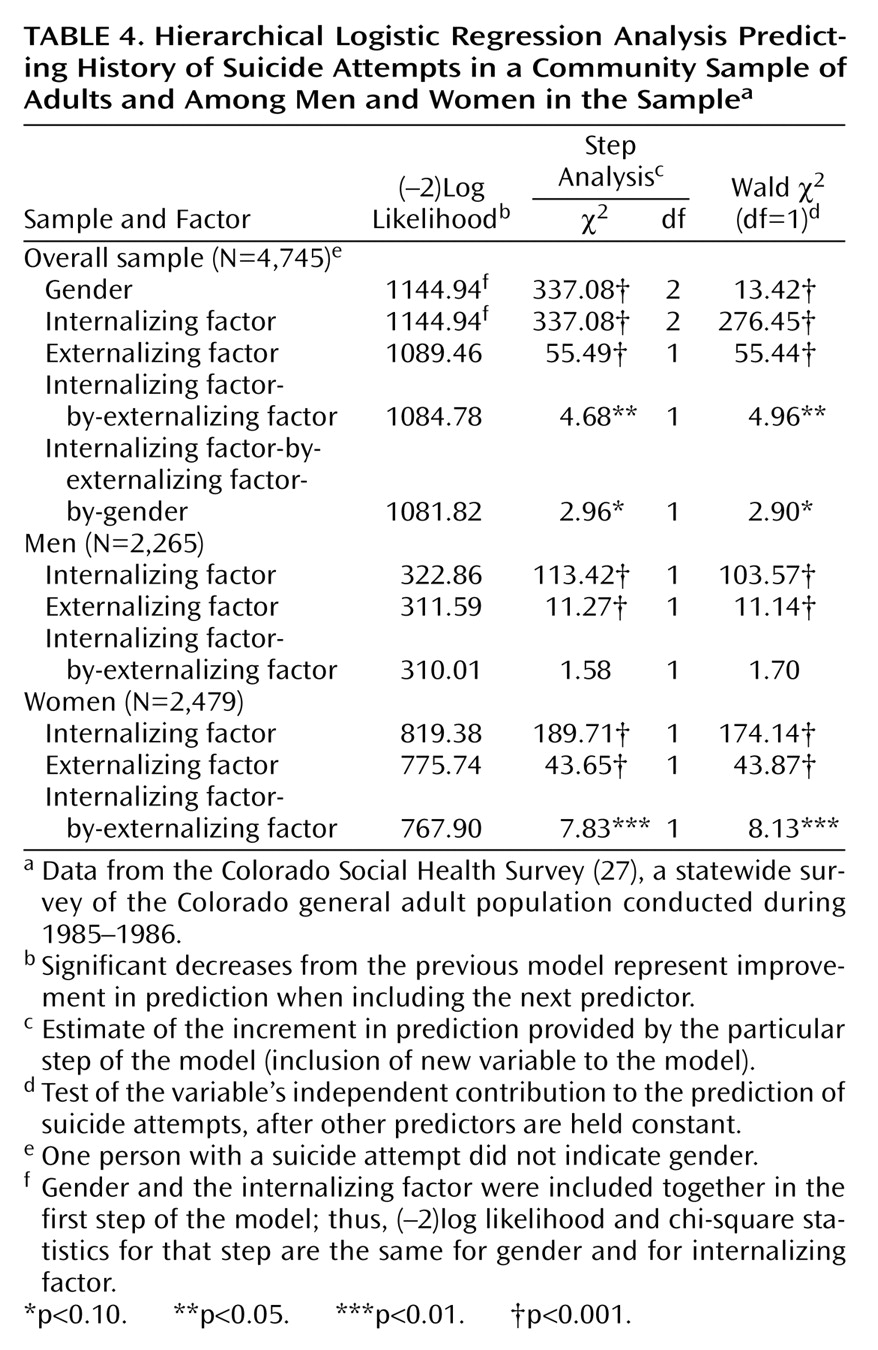
(22), his conceptualization provides a parsimonious approach to examining the influence of a collection of correlated syndromes on outcomes. Following this framework, we attempted to validate this two-factor structure of mental disorders in an epidemiological sample and extended Krueger’s work by including both schizophrenia and bipolar disorder in these analyses to determine if these inclusions would change the factor structure. Then, factor scores were used in regression analyses to determine whether externalizing psychopathology predicts risk for suicide attempts above the variance accounted for by the presence of internalizing symptoms and comorbid internalizing
and externalizing symptoms.
In addition, we were interested in whether these effects would be similar for both genders. Typically, women are more likely to experience depressive and internalizing symptoms and engage in suicide attempts
(23–
25), but externalizing behaviors are more strongly associated with men
(26). Thus, we explored whether the effect of externalizing disorders on suicide was equally robust for both genders.
Discussion
An innovative aspect of this study was the application of dimensional models of psychopathology
(19,
38) to the examination of relations between internalizing or externalizing symptoms and suicidal behavior. Although a large literature has confirmed relationships between suicidal behaviors and externalizing syndromes
(5,
39–41), a number of these studies have been conducted with incarcerated or psychiatric subjects. Our results support the validity of the link between externalizing syndromes and suicidal behavior in a large community sample, confirming that this relationship is robust across psychopathological and “normal” populations.
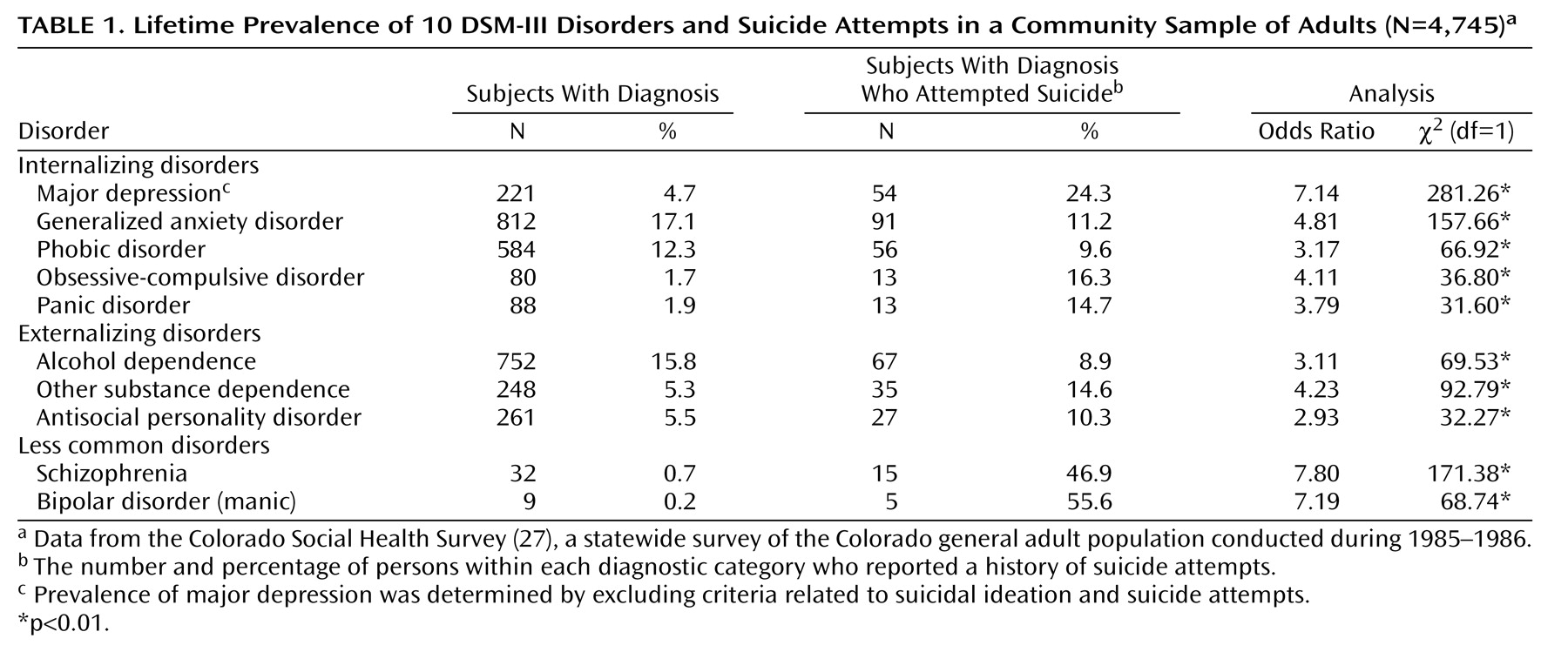
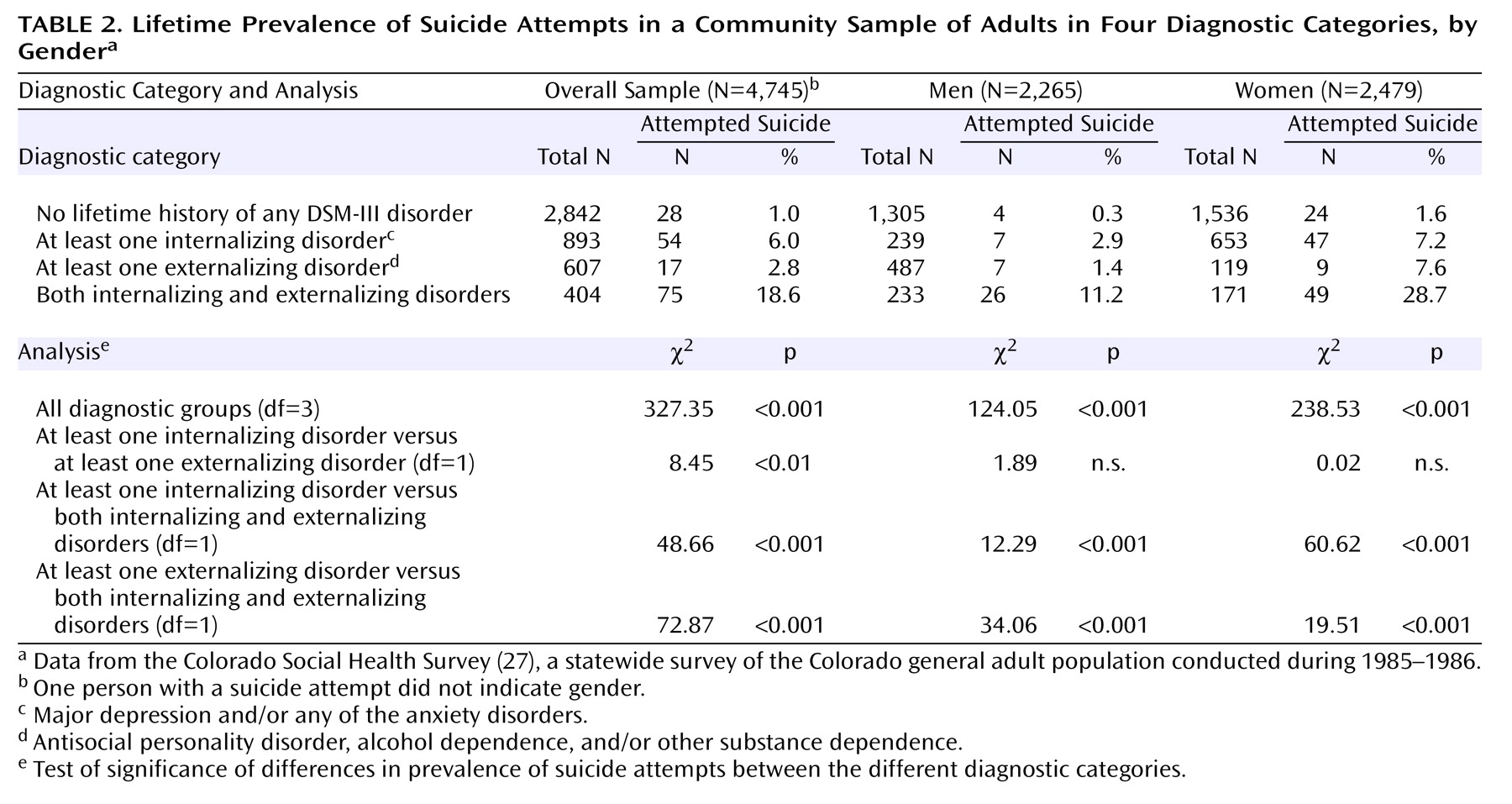
In addition, our data provide support for the thesis that the relationship between a history of suicidal behavior and a history of impulsive, deviant (externalizing) behaviors is independent of internalizing symptoms and independent of comorbidity between internalizing and externalizing symptoms. Indeed, the results of the chi-square analyses of diagnostic categories showed that persons who had internalizing disorders did not differ in rate of suicide attempts from those with externalizing disorders. A more important finding was that the results of the regression analyses of symptom count data suggested that the common variance associated with these disorders (i.e., the externalizing factor dimension) is predictive of a history of suicide attempts. As suggested by Krueger and colleagues
(19,
21), a common vulnerability factor may underlie the co-occurrence of externalizing behaviors; our data indicate that suicide risk among persons with externalizing syndromes may also be related to this common diathesis
(5). The underlying mechanism in this relationship (e.g., impulsivity) would theoretically be different from the mechanism that links suicide to depressive and other internalizing disorders (e.g., hopelessness)
(7,
11,
12).
Results from the current study point to other areas for future study. Research on normal personality links to psychopathology can help in identifying the common risk factor for externalizing and suicidal behaviors. For example, in a study by Verona et al.
(42), analyses revealed that extremes in personality traits reflective of negative emotionality and (low) constraint accounted for the relationship between antisocial behavior history and suicide attempt history among male offenders. Moreover, Krueger and colleagues
(20,
21) have confirmed that the externalizing spectrum of disorders is related to the genetically linked personality trait of low constraint. Although trait negative emotionality may represent vulnerability to both internalizing and externalizing psychopathology (and thus explain their comorbidity), low constraint seems to be related to engagement in externalizing versus internalizing behaviors
(20). Application of this hypothesis to the relationship between suicidal behavior and externalizing symptoms should be examined directly in future work.
Another important contribution of this study is the analysis of relationships between psychopathology and suicidal behavior in men and women separately. As in earlier studies, women were more likely to engage in suicidal behaviors than men, probably because they had a higher prevalence of depression, which was a strong predictor of suicide attempts. However, externalizing psychopathology uniquely predicted suicidal behaviors in both genders, even though women showed fewer externalizing symptoms. On the other hand, women, more than men, showed strong relationships between comorbid externalizing and internalizing psychopathology and suicide attempt history. These results are only preliminary and require replication; however, they suggest that suicidal behaviors in women with externalizing symptoms may relate to the combination of emotional instability (such as depression or anxiety) and behavioral disconstraint (represented by acting-out behaviors)
(43). This latter description is reminiscent of borderline personality traits, which are strongly linked to self-harm in women. Unfortunately, the Colorado Social Health Survey did not obtain information on borderline personality disorder, which is a limitation of this study. Thus, we could not investigate this hypothesis directly, although such an endeavor would be an important contribution in future work.
Some have suggested that substance dependence and antisocial personality disorder in men may be the equivalents of depression or anxiety in women and, thus, that externalizing syndromes may represent unrecognized depression in men (see reference
44). However, in our study, men were more likely than women to endorse both internalizing and externalizing symptoms; thus, the differential results for men and women are too preliminary to interpret fully. Nonetheless, these results suggest that gender differences in the link between psychopathology and suicide should be explored further in other samples in which rates of suicide attempt are higher, especially among male participants (see reference
45).
Certain limitations of the current study should be considered in interpreting the findings. The diagnosticians were lay interviewers; thus, our results need to be replicated in studies utilizing experienced clinical interviewers. Also, diagnosis and symptom assessment relied on DSM-III criteria, and future research should confirm these results using the most recent version of DSM. We also relied on participants’ retrospective reports, which is a limitation of using lifetime diagnosis and symptom counts. However, this strategy allowed us to obtain data from a large number of persons who endorsed psychopathological symptoms, increasing the reliability of our statistics. In addition, when analyses were performed by using more current (within the last year) information on diagnostic and suicidal behavior variables, we found similar results. Nonetheless, future research can examine, in a prospective or longitudinal fashion, whether initial symptoms of externalizing disorders predict later suicidal behaviors. An additional weakness of the current study is the binary index (yes/no) of suicidal behavior that was utilized. However, there was clear evidence for the validity of the index, in that it was correlated in predicted ways with diagnostic variables (particularly the high concordance of suicidal behavior with depression). Nonetheless, this limitation should be remedied in future research to help uncover differences in the nature of suicidal acts performed by antisocial individuals, compared with clinically depressed individuals
(16).
Another weakness of this study is that we could not fully examine the important relationship between suicide and symptoms of schizophrenia and bipolar disorder, because of the low base rates of these syndromes in the studied population. In extending Krueger’s work, we did find that these two symptom clusters tended to load on the internalizing factor of psychopathology. However, our factor analytic results need to be replicated in future research, which should examine further the relationship of schizophrenia and bipolar disorder symptoms with externalizing disorders and suicidal behaviors.
Our results also have clinical implications. In general, this work informs the development of interventions to prevent individuals from engaging in behaviors that are destructive to the self and to others. Our results suggest that clinicians and treatment providers would benefit from paying closer attention to the assessment of suicidal impulses in persons exhibiting externalizing behaviors, even if they do not (but especially when they do) present with comorbid depression.