Over the past several decades in the United States, gambling has become an increasingly popular, widely available, and socially acceptable activity. Legalized gambling ventures currently gross more than $50 billion annually
(1), and approximately two-thirds of the adult population have gambled in the past year
(2). Over the past several decades, the growth rate of gambling participation has been highest among the older adult age group: lifetime gambling rates in older adults increased from 35% in 1975 to 80% in 1998, and past-year gambling rates increased from 23% to 50% during the same time period
(3). Despite these changes, the health correlates of gambling participation in older adults have not been extensively investigated. While several studies have reported on the epidemiology of gambling in older adults
(4,
5), there is much that remains to be learned regarding the gambling behaviors of older adults.
Problem and pathological gambling have been demonstrated to be associated with negative measures such as high rates of job loss, receipt of welfare benefits, bankruptcy, arrest, incarceration, divorce, mental health problems, and poor general health
(3). However, a relatively small proportion of individuals exhibit problem or pathological gambling (up to approximately 5% of the general adult population)
(3,
6). The majority of adults in the United States gamble “recreationally,” at levels not considered problematic or pathological. Recreational gamblers, who by definition do not meet the diagnostic criteria for pathological gambling at a threshold (pathological gambling) or subthreshold (problem gambling) level, do not experience interference in areas of life functioning related to gambling similar to that of problem and pathological gamblers. Nonetheless, few studies have systematically examined the health correlates of recreational gambling, and, given the large proportion of recreational gamblers in the general adult population, an improved understanding of the health correlates of recreational gambling has significant public health implications
(5,
6). Recently, we showed that past-year recreational gambling is associated with both negative and positive measures of health and well-being: past-year recreational gamblers were found to have elevated rates of alcohol abuse/dependence, substance abuse/dependence, depression, and incarceration
(7). However, they also had higher rates of good to excellent subjectively rated general personal health. These findings suggest the need for additional research to examine not only the nature of the observed associations but also the relationship of recreational gambling to measures of health and well-being within specific demographic groups.
Older and retired adults represent an attractive demographic group for gambling ventures. Older adults constitute one of the largest-growing segments of the population
(8) and are frequently perceived as desiring social interaction and entertainment and as having large amounts of “free” time and disposable income and fewer responsibilities than nonelderly adults
(9). Residential and assisted-care facilities often offer gambling as in-house entertainment (e.g., bingo) and organize trips to casinos
(9,
10). One recent study of more than 6,000 adults over age 65 years indicated that gambling activities were the single biggest social activity attended by nursing home residents, with 23% attending in-house bingo games at least four times per month
(9).
Data suggest that recreational gambling can have both beneficial and detrimental effects
(11,
12). Among older adults, recreational gambling, like many enjoyable leisure activities, may provide opportunities for socialization, sensory and cognitive stimulation, and other benefits. However, data also suggest that older adults may be particularly vulnerable to gambling-related problems. First, there is some suggestion that slot machine games, which are popular among older gamblers
(11), may be more addictive than other types of gambling
(12). Second, early stages of dementia and other cognitive deficits may put older people at increased risk: excessive lottery and sweepstakes participation have been described in people with dementia
(13). Several state attorneys general have brought lawsuits on behalf of sweepstakes victims, many of whom are older adults
(14). Third, older adults may face greater problems related to excessive gambling because, although they are not necessarily poor, they often have restricted incomes and limited ability to work in order to replace savings or recover losses such as the substantial ones often incurred by problem or pathological gamblers
(15,
16). In response to the possibility of excessive risk, particularly given the rising rates of gambling among older adults, the National Council on Problem Gambling developed a task force specifically to focus on older adult gambling
(3). Taken together, these data highlight a need for an improved understanding of the relationship between recreational gambling and health measures in older adults
(17).
To date, there have been few studies that systematically explore the health correlates of older adult recreational gambling in a population sample
(4,
17). The current investigation utilizes data from the Gambling Impact and Behavior Study, a large national telephone survey of adults in the United States performed in 1998 by the National Opinion Research Center for the National Gambling Impact Study Commission Report
(1). Using these data, we examined 1) the health and well-being correlates of recreational gambling in older versus younger adults, 2) differences in the patterns of health and well-being correlates in older and younger gamblers versus nongamblers, and 3) the gambling patterns of older versus younger adult gamblers.
Method
Study Design
The data for this study are drawn from the Gambling Impact and Behavior Study
(3). The adult survey included two forms of data collection: a telephone survey that used random-digit dialing (N=2,417) and a face-to-face survey of patrons of gambling venues (N=530). Only the telephone survey data are utilized for this analysis owing to the noncomparability of samples and differences in survey questions.
Data for the telephone survey were obtained by using a list-assisted approach and one-plus sampling, as described elsewhere in greater detail
(3). Telephone numbers purchased from Survey Sampling, Inc., were stratified by Survey Sampling by state lottery status, and working residential numbers were identified in part through screening by Survey Sampling
(3). The survey thus targeted households and was likely not to sample from older adults living within assisted-living settings. The individual to be interviewed from the contacted household was determined by means of a variant of the Troldahl-Carter-Bryant method
(3).
The sample for the telephone survey was designed and statistically weighted to be representative of the U.S. population of adults age 18 years and older. Comparison of the final sample to the U.S. population indicated that black respondents were slightly underrepresented and that respondents in the Northeast were slightly overrepresented but that otherwise the sample was quite reflective of the U.S. household adult population
(3). There is no apparent way to examine potential differences in the gambling patterns of respondents and nonrespondents. Of the 3,160 interviews attempted, complete data were obtained for 2,417 interviews, for a study response rate of 76%.
After complete description of the study to potential participants, verbal consent was obtained to complete the interview. The study of publicly accessible data from the Gambling Impact and Behavior Study was presented to the Yale Human Investigations Committee and exempted from review under federal regulation 45 CFR Part 46.101(b).
Study Measures
Variables described in the analyses were derived from those described in the Gambling Impact and Behavior Study
(3), with responses to questions grouped as indicated in the tables. To obtain data on recreational gamblers, we excluded individuals with present or past problem or pathological gambling (N=51) using the criteria defined in the Gambling Impact and Behavior Study
(3). As in the Gambling Impact and Behavior Study, we categorized respondents who reported three to four and five or more DSM-IV-based diagnostic criteria for pathological gambling as assessed in the National Opinion Research Center diagnostic screen as being problem and pathological gamblers, respectively. We believe that excluding individuals above this threshold for problem gambling, which is significantly below the DSM-IV-TR criteria threshold for pathological gambling, generated a group of recreational gamblers consisting of individuals who would likely not consider themselves as having a problem with gambling and thus would not present for mental health care for help with a gambling problem.
Past-year alcohol use was defined as a report of having consumed alcohol at least 12 days in the previous 12 months. This threshold, which was used as a gateway question for assessment of past-year alcohol abuse/dependence, was based on data from the National Household Survey on Drug Abuse and was designed to capture the majority of alcohol-dependent respondents while minimizing respondent burden
(3). Past-year substance abuse/dependence was similarly assessed by using items from the National Household Survey on Drug Abuse. Respondents needed to meet a threshold criterion of use of a substance (not including nicotine or caffeine) for nonmedical purposes on at least five days in the previous year in order to be asked follow-up questions assessing the DSM-IV criteria for abuse/dependence (e.g., questions about tolerance, withdrawal, and adverse physical or social effects of use). Substance abuse/dependence in the current study was thus intended to assess abuse/dependence of alcohol; marijuana or hashish; cocaine or crack; stimulants such as methamphetamine, amphetamines, or speed for nonmedical reasons; or tranquilizers such as diazepam or alprazolam for nonmedical reasons.
Depressive symptoms were assessed in the entire sample by using two screening questions from the NIMH Diagnostic Interview Schedule
(18) that assessed a lifetime history of 2 weeks when the respondent either felt sad, empty, and depressed all the time or lost interest in most things previously found enjoyable. As with the measures of drug and alcohol use, such screening questions were designed to capture the majority of respondents with a history of major depression while minimizing respondent burden.
Whether the respondent sought mental health treatment in the past year was assessed by the question, “Since [DATE 12 MONTHS AGO], have you gone to a clinic, doctor or counselor, or outpatient treatment for problems with your emotions, nerves, or mental health?” Past-year subjective general health was assessed as described in the Gambling Impact and Behavior Study
(3) with the question, “How would you describe your general health over the past 12 months?” The Gambling Impact and Behavior Study did not contain additional, objective measures of general health. Lifetime incarceration was assessed by the question, “Have you ever been incarcerated in prison or jail for any reason?” Lifetime bankruptcy was assessed by the question, “Have you ever filed for bankruptcy?”
Most measures of gambling patterns (reasons for gambling, age of gambling initiation, and quantity/frequency measures) were taken directly from the responses to Gambling Impact and Behavior Study items
(3). For example, respondents were asked to identify the reasons why they gambled from a formulated list. They were also asked the earliest age they ever gambled (before/after age 18 years) and whether they usually gambled with someone they knew well (yes/no). Responses to the questions on maximum frequency of gambling, largest wins, and largest losses were collapsed into the following categories: for maximum frequency—daily, one to three times per week, one or two times per month, a few days per year, and only once a year; for largest wins and largest losses—<$100, $100–$500, and >$500.
We created new categories to group types of gambling and to group favorite forms of gambling, as in our prior work
(7), as follows. Strategic gambling was defined as any acknowledgment of participation in track/off-track, card room, private game, table game, sports, video poker, card game, roulette, dice, games of skill, pari-mutuel, auction, board game, and frog racing gambling. Nonstrategic gambling was defined as any acknowledgment of participation in lottery, bingo, keno, pull-tab, slot machine, video lottery, unlicensed numbers game, 50–50, raffle/drawing, or big wheel gambling. Machine gambling included any acknowledgment of participation in Internet, machine, slot machine, video lottery, video poker, electronic game, or video machine gambling. Past-year noncasino gamblers were defined by any acknowledgment of past-year participation in racetrack, jai alai fronton, off-track betting parlor, lottery, bingo hall, charitable, card room, private game, store, bar, restaurant, truck stop, or computer gambling. Past-year casino gamblers were defined by acknowledgment of past-year participation in any game played at a casino.
Favorite types of strategic gambling included any positive responses to book-type betting, cards, dice, games of skill, off-track betting, betting on the outcome of sports, pari-mutuel sports, roulette, sports pool, or table games. Favorite types of nonstrategic gambling included any positive responses to bingo, instant lottery, live keno, lottery, pull-tabs, or slots. Favorite types of machine gambling included any positive responses to Internet or slot or video machine gambling.
Data Analysis
Data from individuals for whom gambling information was missing (N=4) and those with probable problem or pathological gambling, as defined in the Gambling Impact and Behavior Study
(3) and determined by a lifetime or past-year National Opinion Research Center diagnostic screen score of 3 or more (N=51), were removed for the present analyses. Of the 51 subjects removed because of prior or current problem or pathological gambling, two were age 65 years or older and 49 were within the 18–64-year age group. These individuals corresponded to 0.50% and 2.43% of the older and younger adult age groups, respectively. Weighting factors calculated for the full sample by the Gambling Impact and Behavior Study were adjusted for the size of the sample examined in the present study (N=2,362).
The final sample was divided into older adults (age ≥65 years) and younger adults (ages 18–64 years) as well as respondents acknowledging or denying past-year gambling. Analyses proceeded in several steps. First, sociodemographic characteristics (gender, education, marital status, employment status, and income) were compared across gamblers and nongamblers in the two age groups by using chi-square tests. Second, odds ratios relating outcome measures of health and well-being to gambling status, both unadjusted and adjusted for potentially confounding sociodemographic factors, were estimated by using a logistic regression procedure and a Wald chi-square test for significance. Odds ratios associated with alcohol use and abuse/dependence, substance abuse/dependence, and depression were adjusted for sociodemographic factors. Measures of mental health treatment sought in the previous year, subjective general health, incarceration, and bankruptcy were additionally adjusted for lifetime substance abuse/dependence and depression. Third, interaction terms between age group and gambling were tested to identify factors that differentially distinguished past-year gamblers from nongamblers between age groups. Finally, older and younger gamblers were compared on their gambling patterns.
Results
Among older adults, 50.3% (N=195) reported gambling in the previous year, compared to 65.5% (N=1,291) of younger adults. Of the older adult group, 0.50% (N=2) were classified as ever having experienced problem or pathological gambling, compared with 2.43% (N=49) of the younger adults (χ2=5.96, df=1, p<0.02). This between-group difference persisted when weighted data for the sample were examined (0.30% versus 2.40%) (χ2=7.16, df=1, p<0.008). As described in the Method section, individuals with prior or current problem or pathological gambling were excluded from subsequent analyses in order to examine correlates of recreational gambling.
Demographic Characteristics
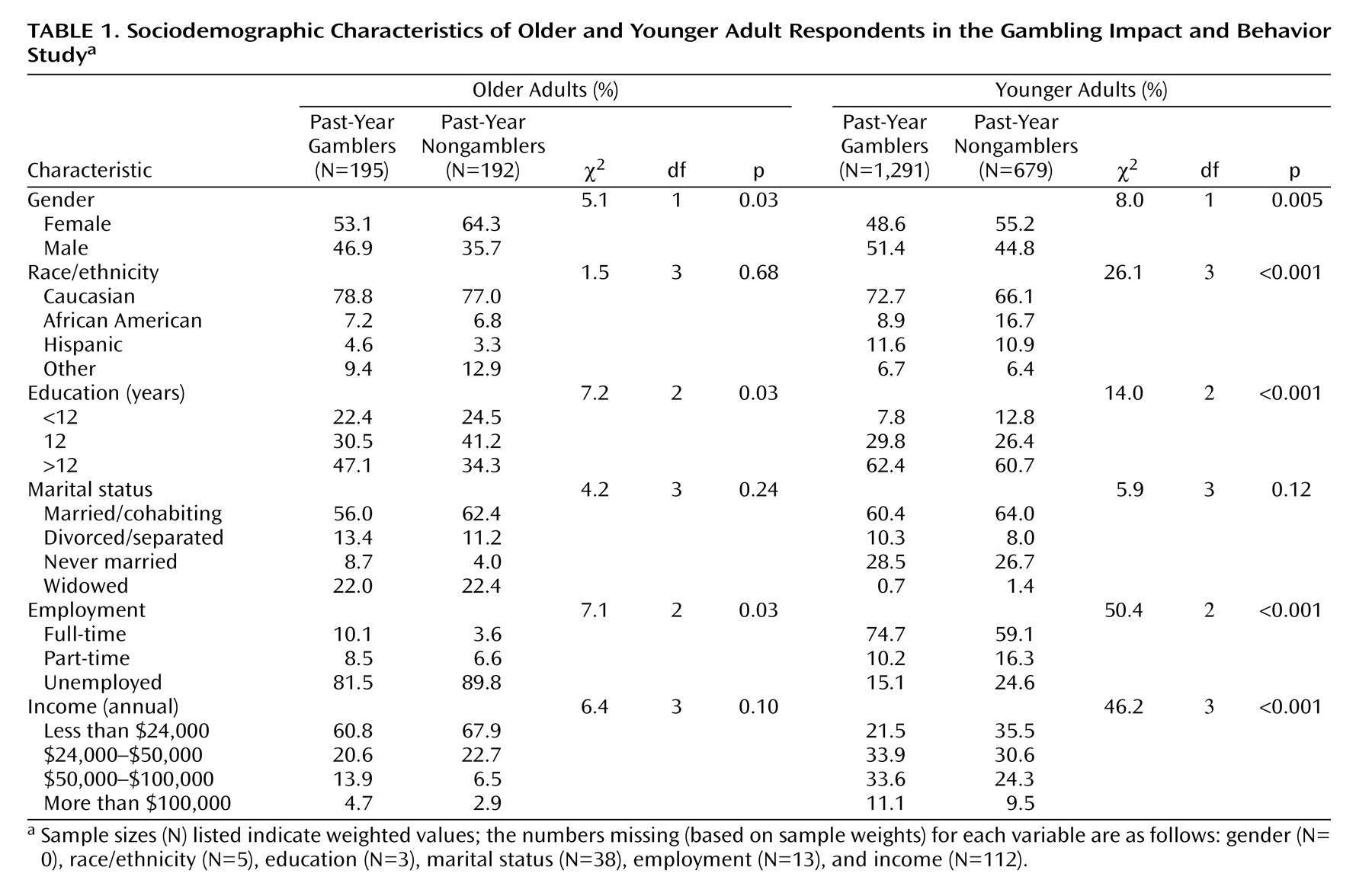
Compared with older nongamblers, older recreational gamblers were more likely to be male, to have more than 12 years of education, and to be employed full-time (
Table 1). Younger adult recreational gamblers differed from younger adult nongamblers on the variables of gender, race/ethnicity, education, employment, and income (
Table 1). With the exception of marital status, all sociodemographic variables were included in subsequent multivariate analyses.
Health and Well-Being
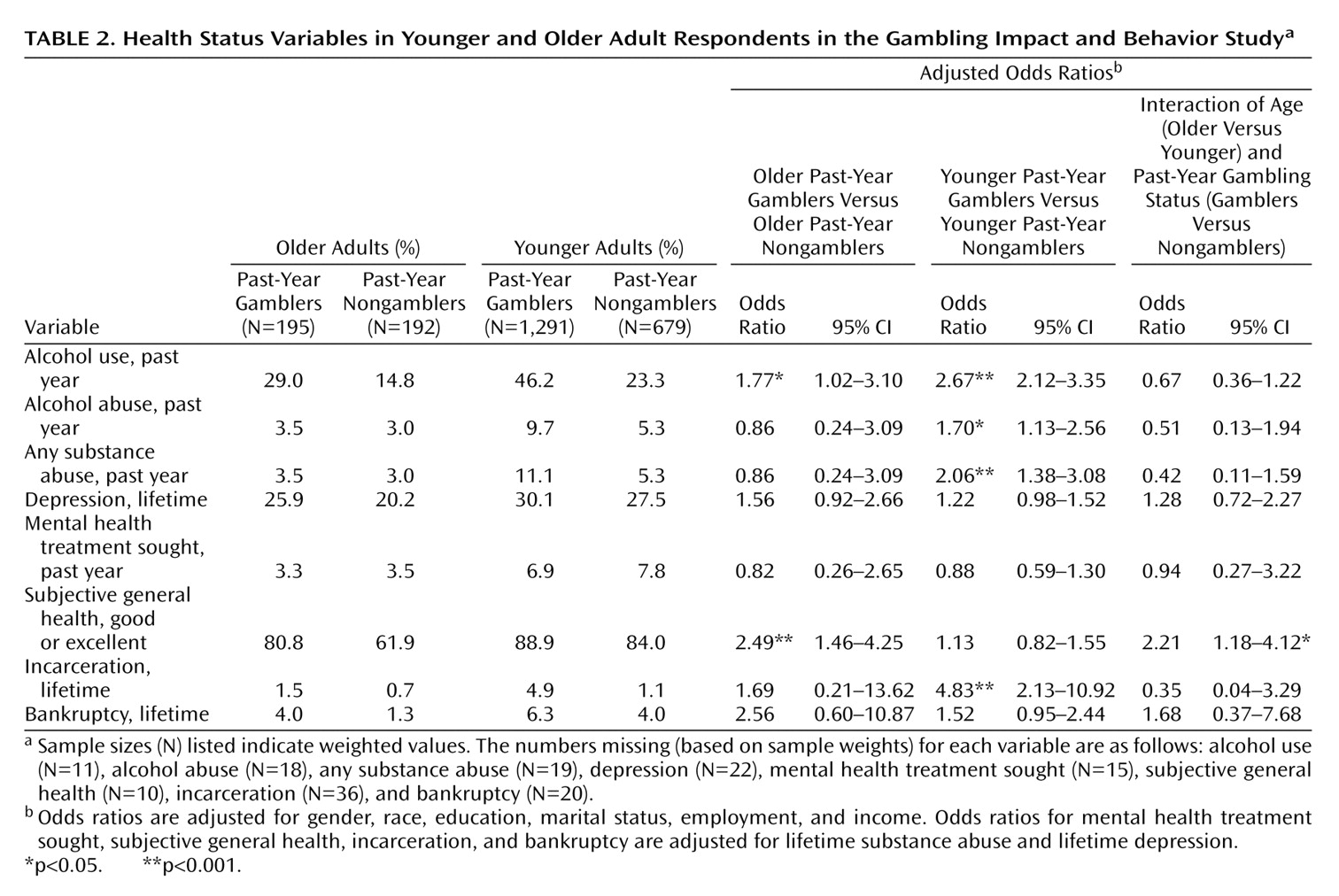
Several significant differences were observed in measures of health and well-being between older adult recreational gamblers and nongamblers (
Table 2). After sociodemographic factors were adjusted, older gamblers were significantly more likely to have used alcohol in the previous year (χ
2=4.07, df=1, p<0.05), were marginally more likely to have a lifetime history of depression (χ
2=2.71, df=1, p=0.10), and were 2.49 times more likely (95% confidence interval=1.46–4.25) to report good or excellent subjective general health (χ
2=11.17, df=1, p=0.0008). In the younger adult age group, the variables of alcohol use (χ
2=71.13, df=1, p=0.0001), alcohol abuse/dependence (χ
2=6.4, df=1, p<0.02), substance abuse/dependence (χ
2=12.61, df=1, p=0.0004), and incarceration (χ
2=14.28, df=1, p=0.0002) distinguished the past-year recreational gamblers and nongamblers, while the variables of bankruptcy and depression showed marginal significance (
Table 2). In all cases, higher rates were observed in the gambling group (
Table 2).
An interaction model investigating factors that distinguished past-year recreational gamblers from nongamblers across age groups was significant for the variable of subjective general health (
Table 2). Specifically, higher rates of good to excellent subjective general health were associated with recreational gambling to a greater degree in the older adult age group (χ
2=6.19, df=1, p<0.02).
Gambling Motivations, Patterns, and Preferences
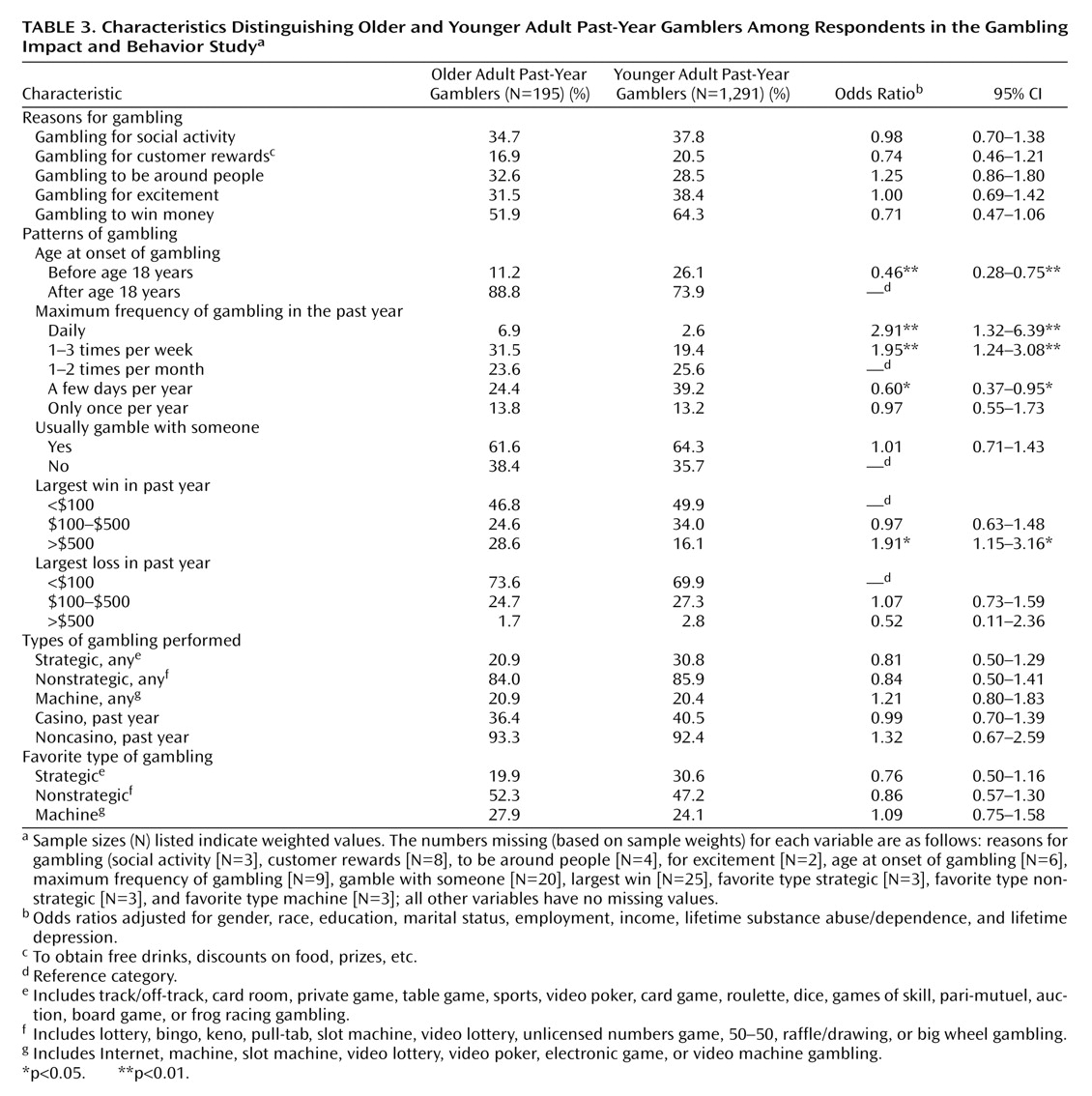
Older past-year recreational gamblers were marginally less likely than younger gamblers to report gambling to win money. However, they were significantly less likely to report first gambling before age 18 years (χ
2=9.78, df=1, p<0.002) and gambling in the past year at a frequency of only a few days per year (χ
2=4.73, df=1, p<0.03) (
Table 3). They were more likely to report gambling in the past year one to several times per week (χ
2=8.23, df=1, p<0.005) or at a daily frequency (χ
2=7.06, df=1, p<0.008) and having experienced a win of >$500 (χ
2=6.26, df=1, p<0.02). Interaction effects between age and gender revealed no significant findings (data not shown).
Discussion
To our knowledge, this study is one the first to systematically investigate health and well-being correlates of recreational gambling in older adults and the gambling attitudes and behaviors of older, compared with younger adult recreational gamblers. We found that, in comparison to the findings for younger adults, there are fewer negative measures of health and well-being associated with recreational gambling in older adults. Specifically, the findings of increased rates of alcohol abuse/dependence, substance abuse/dependence, and incarceration that are found among younger recreational gamblers were not observed in the older recreational gamblers. In addition, we found that subjective ratings of general health were more strongly associated with recreational gambling in older, compared with younger adults, such that older gamblers report being in better health than their nongambling peers.
Health and Well-Being
The finding of fewer negative health effects associated with recreational gambling in older adults is in part a reflection of the epidemiology of factors such as substance abuse and incarceration among older adults in general. Despite the overall lower prevalence of such factors among adults over age 65 years, differences between gamblers and nongamblers might be expected to mirror patterns seen in younger age groups. However, the current results do not support this hypothesis. Several reasons could explain the findings. For example, a selective mortality effect might in part explain the lack of an association between substance use disorders and recreational gambling in the older adult group. That is, people with a history of substance use disorders may have died before reaching age 65 years and thus would not be available for inclusion in the older adult sample.
The finding of a differential association across age groups of better subjective health in association with gambling seems largely driven by the low frequency of acknowledgment of good to excellent subjective health in the older adult past-year nongamblers: while the proportion of respondents reporting excellent health was consistently 80%–90% among all gamblers and younger nongamblers, the proportion of older nongamblers reporting excellent health was only 62%. Again, the relative health reports of younger gamblers and nongamblers might be hypothesized to be mirrored in older adults. The data, however, do not support this hypothesis.
The underlying reasons for these findings could be multiple. For example, the results could reflect differential positive attributes of recreational gambling for the older adult age group. Recreational gambling in older adults may allow for increased socialization, community activity, and travel
(11,
17), which may in turn be reflected in more positive ratings of health
(19,
20). Such an effect may not be evident in younger adults, perhaps because other social or occupational activities take priority. It is also possible that a greater proportion of older, compared with younger, adults are too sick to gamble and are categorized in the nongambling group, making the older gamblers appear healthier. These sicker older adults might have more limited access to transportation or lack the energy or motivation necessary for specific types of gambling. Finally, there could exist a reporting bias in the substance and health status questions. For example, older adults may be less likely to report histories of mental health treatment, either because of social stigma
(21) or loss of memory. It is unlikely, however, that such a bias would be differential based on recreational gambling. These findings highlight the need for additional research into the relationship between recreational gambling and health in older adults, specifically to clarify the nature of the relationship and the specific areas of improved health status that are suggested by the current findings.
A cautionary note is indicated in interpreting the findings. The current study focused on recreational gambling and excluded individuals with problem or pathological gambling from the analyses. As problem and pathological gambling have been associated with adverse health measures
(1,
3), conclusive statements regarding the effects of gambling in older adults should be interpreted cautiously.
Gambling Motivation
The finding of a marginally lower likelihood for older adults to gamble to win money is consistent with patterns of gambling motivation in older adult pathological gamblers in treatment settings. Grant et al.
(15) found that 6.3% of pathological gamblers over age 60 years, compared with 26.1% of those age 40–50 years and 36.4% of those age 20–30 years, reported thoughts of winning as motivating factors to engage in gambling. In the same study, the authors found that 50.0% of pathological gamblers over age 60 years, compared with 19.6% of those age 40–50 years and 9.1% of those age 20–30 years, reported boredom or free time as motivating factors to engage in gambling. Although the findings in the study by Grant et al. were not statistically significant because of the small number of subjects, the data suggest that similar motivations to gamble exist for older adult recreational and pathological gamblers, perhaps reflecting different life circumstances common to older adults (e.g., increased unstructured time, decreased drive to earn money).
Gambling Patterns
Older, compared to younger adult past-year recreational gamblers were more likely to start gambling later in life, consistent with the gambling patterns of older adult pathological gamblers in treatment settings
(15,
16). For example, in a comparative study of patients in treatment for pathological gambling, Grant and colleagues
(15) found that patients over age 60 years began gambling, on average, at age 46 years, while younger patients began gambling, on average, between 18 and 27 years. The later age at onset may reflect a lack of availability of gambling opportunities during earlier ages for respondents currently over age 65 years. It is also possible that respondents who gambled only in their younger years might not be included in this analysis because they stopped gambling or were removed from the sample due to a lifetime diagnosis of problem or pathological gambling. Such a “maturation effect,” as has been observed with other behaviors with addictive potential
(22), requires longitudinal exploration, as there currently exist no data on patterns of gambling over a lifetime with an identified cohort.
The finding that older recreational gamblers are more likely to report gambling every day or at least once a week is of concern but also requires additional investigation. For example, it is unclear whether high-frequency gambling, and specific types of high-frequency gambling (casino, bingo, lottery, etc.), affect health and well-being measures in older adults. The current sample of older adult gamblers, which included fewer than 200 older adult gamblers, had limited power for examining these relationships. Larger investigations of older adult gambling patterns are needed to address these and related questions.
Conclusions and Future Directions
This study is among the first to use a probability population sample to investigate the characteristics of past-year older adult gamblers. The results are applicable to a large and growing segment of the population, adults age 65 years and older, more than half of whom report gambling in the past year. The most significant finding from the present study is that recreational gambling in older adults does not appear to be associated with adverse health measures, as observed in younger gamblers, and may even possibly provide some beneficial effect. Although the underlying reasons remain hypothetical, proposed reasons included the increased activity, socialization, and cognitive stimulation that are related to engaging in gambling. Such a mechanism would be consistent with the literature on healthy aging, which indicates that more socially and cognitively active elders are, in general, healthier
(19,
20). Even given the possibility of a positive effect of engaging in recreational gambling, however, careful monitoring of gambling behaviors in older adults appears indicated, given the poorly understood relationship between recreational and problematic forms of gambling, particularly within older adult groups.
Limitations of the data include the use of self-report measures for health status, which may be biased by loss of memory or social stigma, and the cross-sectional nature of the data, which make temporal sequences difficult to elucidate. The use of specific objective measures of health in future studies would be helpful in clarifying the relationship between gambling and health. In addition, small sample sizes, particularly among older age groups, make more detailed analyses of subgroups difficult. Furthermore, given that a number of older adults live in assisted- living communities, the lack of representative sampling within these settings limits generalizability. However, the inclusion of a large general adult sample obtained through random-digit dialing methods and the use of analyses employing weighting factors to make the sample nationally representative are considerable strengths and facilitate generalization of the results.
Future research is needed in several areas. First, longitudinal studies of the course of gambling behavior over the lifetime will be important in understanding the chronological course of gambling in younger and older adults over time, examining in greater detail the positive and negative health associations with specific levels of gambling, and identifying groups at high risk for the development of gambling problems. In addition, longitudinal studies are the best way to test the hypothesized mechanisms suggested by the cross-sectional data used in the present study. Second, it will be important to understand the biological mechanisms related to different patterns of gambling behaviors across age groups. Findings from longitudinal and biological studies will be of significant value in developing health guidelines for gambling in all age groups.