Federal legislation in 2000 and U.S. Food and Drug Administration approval in 2002 allowed psychiatrists and other physicians to obtain registrations from the U.S. Drug Enforcement Agency to prescribe buprenorphine, a schedule III partial opiate agonist, for opioid agonist maintenance treatment in office-based practice. This development may greatly expand access to maintenance treatment for untreated opioid-dependent individuals, estimated in 2001 to number more than 600,000 in the United States
(1), and provide opportunities for physicians to treat patients outside the specialized setting of narcotic treatment programs. Despite the efficacy of buprenorphine for treating opiate dependence and the lower risk of overdose and abuse liability with buprenorphine, compared to methadone
(2–
18), the high prevalence and adverse consequences of concurrent cocaine abuse in this population
(19) raise questions about the comparative efficacy of buprenorphine and methadone for patients with co-occurring cocaine and opioid dependence and about whether maintenance treatment can be improved by combining it with behavioral treatments, such as contingency management.
Cocaine abuse was found in 42% of those entering methadone treatment and in 22% at 1-year follow-up in a national multisite evaluation
(20). Cocaine abuse during opioid agonist maintenance treatment contributes to persistent illicit opioid use
(21); a high risk for HIV infection
(22–
25); higher levels of family, medical, vocational, and legal problems; and a continued focus on drug-related social interactions and criminal activity
(26–
29). We have no efficacious medication for primary cocaine dependence
(30), and methadone maintenance does not specifically reduce cocaine use
(29,
31).
Despite initial findings in animal and human studies that buprenorphine decreases cocaine use and possibly the reinforcing efficacy of cocaine more than does methadone
(32–
39), several randomized clinical trials found comparable or superior efficacy of methadone maintenance, compared to buprenorphine maintenance, for reducing cocaine and illicit opioid use
(40–
45). These findings led to the study hypothesis that methadone is superior to buprenorphine for co-occurring cocaine and opioid dependence. In animal models, however, cocaine self-administration is reduced most when buprenorphine is combined with access to an alternative, nondrug reinforcer, such as noncaloric sweetened water
(46,
47). This finding suggests the possibility, explored in this study, that medications that reduce the reinforcing efficacy of cocaine, such as possibly buprenorphine, would be preferentially enhanced by combining them with alternative rewards.
Contingency management alone or combined with counseling based on the community reinforcement approach can motivate cocaine abstinence in patients without concurrent opioid dependence
(48–
52). Contingency management has been found efficacious during opioid agonist maintenance treatment in some but not all studies of patients with concurrent cocaine and opioid dependence
(53–
60), who often show little internal motivation to reduce cocaine use
(61). The community reinforcement approach encourages involvement in rewarding, non-drug-related alternatives to illicit drug use; was used in combination with contingency management in the initial studies; and may contribute to persistence of abstinence after discontinuation of contingency management
(48,
49,
62).
Consequently, this study compared methadone and buprenorphine and evaluated whether contingency management improved maintenance treatment with methadone or buprenorphine. The two study hypotheses were that 1) methadone is superior to buprenorphine maintenance treatment for reducing illicit opioid and cocaine use and 2) contingency management compared to performance feedback reduces illicit opioid and cocaine use during opioid agonist maintenance treatment. The study also explored whether contingency management leads to greater reductions in cocaine use during buprenorphine rather than methadone maintenance treatment and whether reductions in illicit drug use persist after the value of the voucher rewards used in contingency management is reduced to a nominal level.
Method
Subjects
The subjects were 162 individuals seeking opioid agonist maintenance treatment in New Haven, Conn. All subjects were at least 18 years old, had at least a 1-year history of documented opioid dependence, and met the DSM-IV criteria for opioid dependence and cocaine abuse or dependence as assessed by the Structured Clinical Interview for DSM-IV
(63) conducted by a bachelor’s-level research assistant and confirmed by a psychiatrist. Individuals were excluded from participation if they met any of the following criteria: 1) current alcohol or sedative dependence; 2) significant medical condition (e.g., liver enzyme elevations greater than three times normal limit); 3) current psychotic or bipolar disorder, major depression, or suicide risk; 4) pregnancy; and 5) inability to read or understand English. Potential subjects who met the initial eligibility screening criteria and expressed interest in the study (N=169) between February, 1995, and July, 1998, were referred to the study through a centralized opiate intake treatment and research screening unit, and 163 of these 169 potential subjects enrolled in the study. Reasons for not enrolling included failure to complete intake (N=1), failure to attend the admission session (N=3), presence of a psychiatric condition (N=1), and expectation of incarceration (N=1). Randomization occurred at the time of enrollment. One of the 163 subjects received only one medication dose and provided no additional data; data for this subject were not included in the analyses. The results of analyses with this subject included do not differ from those with the subject excluded.
All eligible subjects provided written, informed, and voluntary consent before enrollment. The study protocol was approved by the Human Investigation Committee of the Yale University School of Medicine.
Treatments
Subjects were randomly assigned to one of four treatment groups (methadone with contingency management, methadone with performance feedback, buprenorphine with contingency management, or buprenorphine with performance feedback) by using a computerized urn randomization procedure to balance the groups with regard to gender and presence of antisocial personality disorder. Subjects and research personnel were informed about allocation to contingency management or performance feedback at the time of randomization.
Community Reinforcement Approach Counseling
Manual-guided counseling with the community reinforcement approach
(64) was provided to all subjects in individual sessions twice weekly during the first 12 weeks of the study and weekly during the last 12 weeks by a total of 11 therapists (nine doctoral-level psychologists, one psychiatrist, and one drug counselor with more than 5 years of experience). Therapists received intensive training in community reinforcement approach counseling and weekly individual supervision by a senior therapist with extensive training and experience in behavioral therapy. The community reinforcement approach utilizes behavioral counseling and cognitive and behavioral skills training to help patients develop long-range goals and encourage them to engage in non-drug-related, rewarding activities
(64,
65).
Opioid Agonist Maintenance Medications
Opioid agonist maintenance medications were dispensed to subjects daily under direct observation. A research pharmacist who had no direct contact with any of the subjects prepared all medications in advance. To maintain the double blind, all subjects received identical volumes of an oral liquid medication (methadone or placebo) and identical volumes of a sublingual liquid medication (buprenorphine or placebo). Methadone (35 mg p.o.) or sublingual buprenorphine (4 mg) was started on the first day of treatment; the medication dose was increased rapidly during the first 2 weeks of treatment to a predetermined set daily initial maintenance dose (65 mg/day of methadone or 12 mg/day of buprenorphine). The success of the blinding was evaluated by asking each patient during the maintenance phase which medication the patient thought he/she was taking. These assessments were initiated partway through the study and are available for 42 subjects. Most subjects thought they were receiving buprenorphine, regardless of whether they were receiving methadone (72% [18/25] of the methadone patients reported that they thought they were receiving buprenorphine and one reported not knowing) or buprenorphine (88% [15/17] of the buprenorphine subjects thought they were receiving buprenorphine). The initial maintenance dose of methadone was increased by 10 mg and the initial maintenance dose of buprenorphine was increased by 2 mg after 2 weeks if 50% or more of the urine toxicology tests in the preceding week were positive for opiates. A total of two dose increases was permitted (to a maximum daily methadone dose of 85 mg or buprenorphine dose of 16 mg). Medication doses were tapered after completion of 24 weeks of treatment for patients who were not planning to transfer to methadone maintenance treatment.
Contingency Management
Subjects assigned to contingency management earned monetary vouchers for each urine sample that tested negative for both illicit opioids and cocaine, beginning the first week of treatment. Research assistants collected urine from subjects thrice weekly, tested them immediately using on-site testing, and gave subjects a slip of paper indicating the results of each test (negative or positive for illicit opioids or cocaine) and the value of the voucher earned if the sample was drug-free. During the first 12 weeks of maintenance treatment, the value of the voucher increased from the initial $2.50 value in $1.25 increments for each successive drug-free urine sample. Subjects earned a $10 bonus voucher for providing three consecutive drug-free urine samples. The value of the voucher was reset to $2.50 after a drug-positive urine sample, was subsequently increased in $1.25 increments for successive, consecutive drug-free samples, and could return to the previous level after five consecutive drug-free samples. After the first 12 weeks of treatment, the escalating schedule of voucher reward was discontinued, and subjects earned a voucher with a nominal value of $1.00 for each drug-free urine sample. Money earned for drug-free urine samples could be exchanged at any time for goods or services consistent with treatment goals and generally purchased by a project staff member. The maximum value of the vouchers that a subject could earn in contingency management was $1,033.50.
Performance Feedback
To control for the interaction between research assistants and subjects and the provision of feedback about urine toxicology results in contingency management, subjects assigned to performance feedback received an informational slip of paper of no monetary value indicating the results of each urine test (negative or positive for opiates and for cocaine).
Assessments
At baseline, subjects were assessed with the Addiction Severity Index, Structured Clinical Interview for DSM-IV (sections for substance use, psychotic disorders, mood disorders, and antisocial personality disorder), Center for Epidemiological Studies Depression Scale
(63,
66–68), and urine toxicology testing. Urine samples were obtained three times weekly during treatment under direct observation. On-site toxicology testing used the EMIT system (Syva Company, Cupertino, Calif.), with cutoffs for positive findings set at 300 ng/ml for morphine and for cocaine metabolite. All assessments were administered by trained and experienced research assistants, who were supervised by a research coordinator with many years of experience in drug abuse treatment clinical trials.
Statistical Analyses
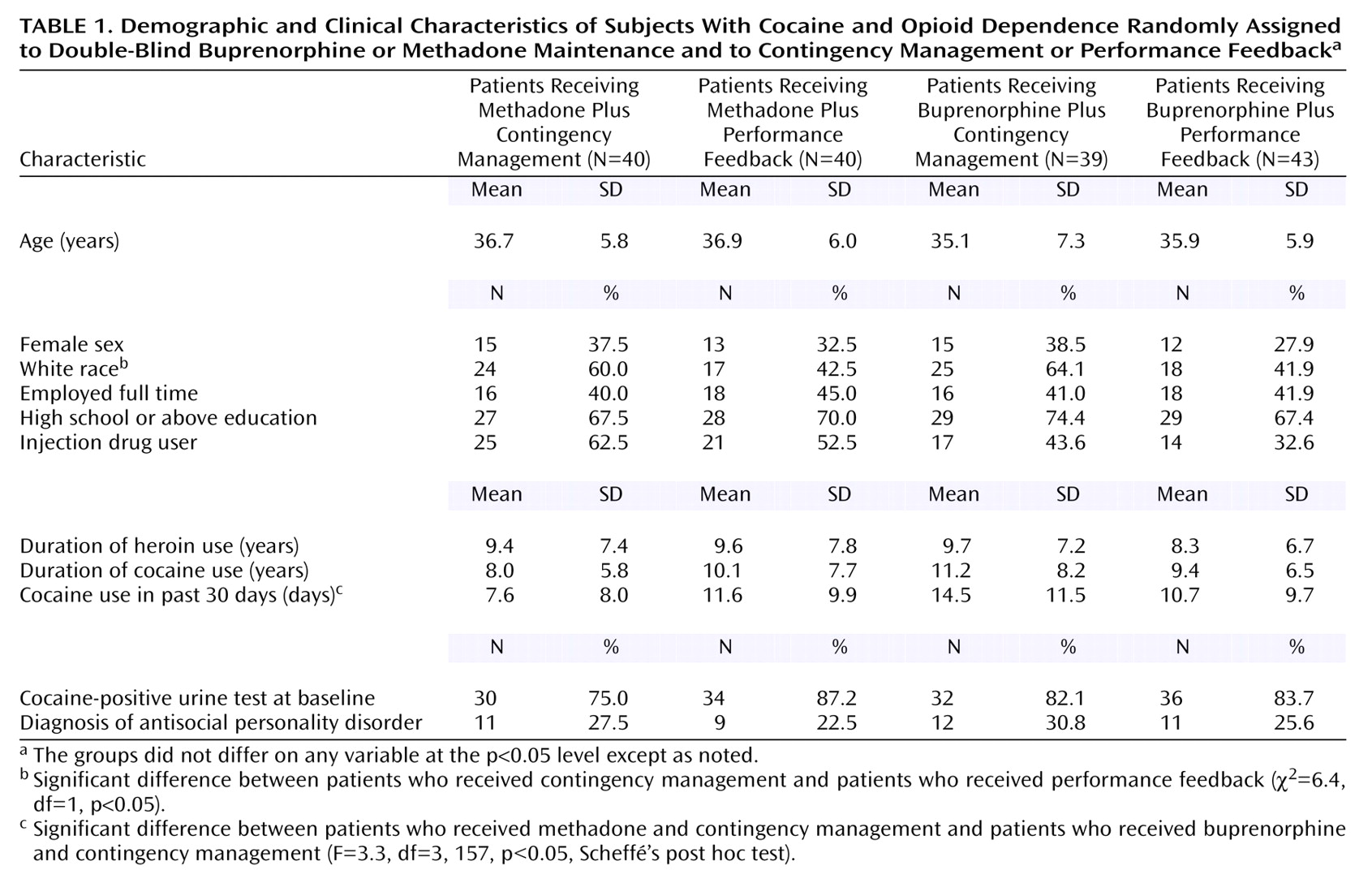
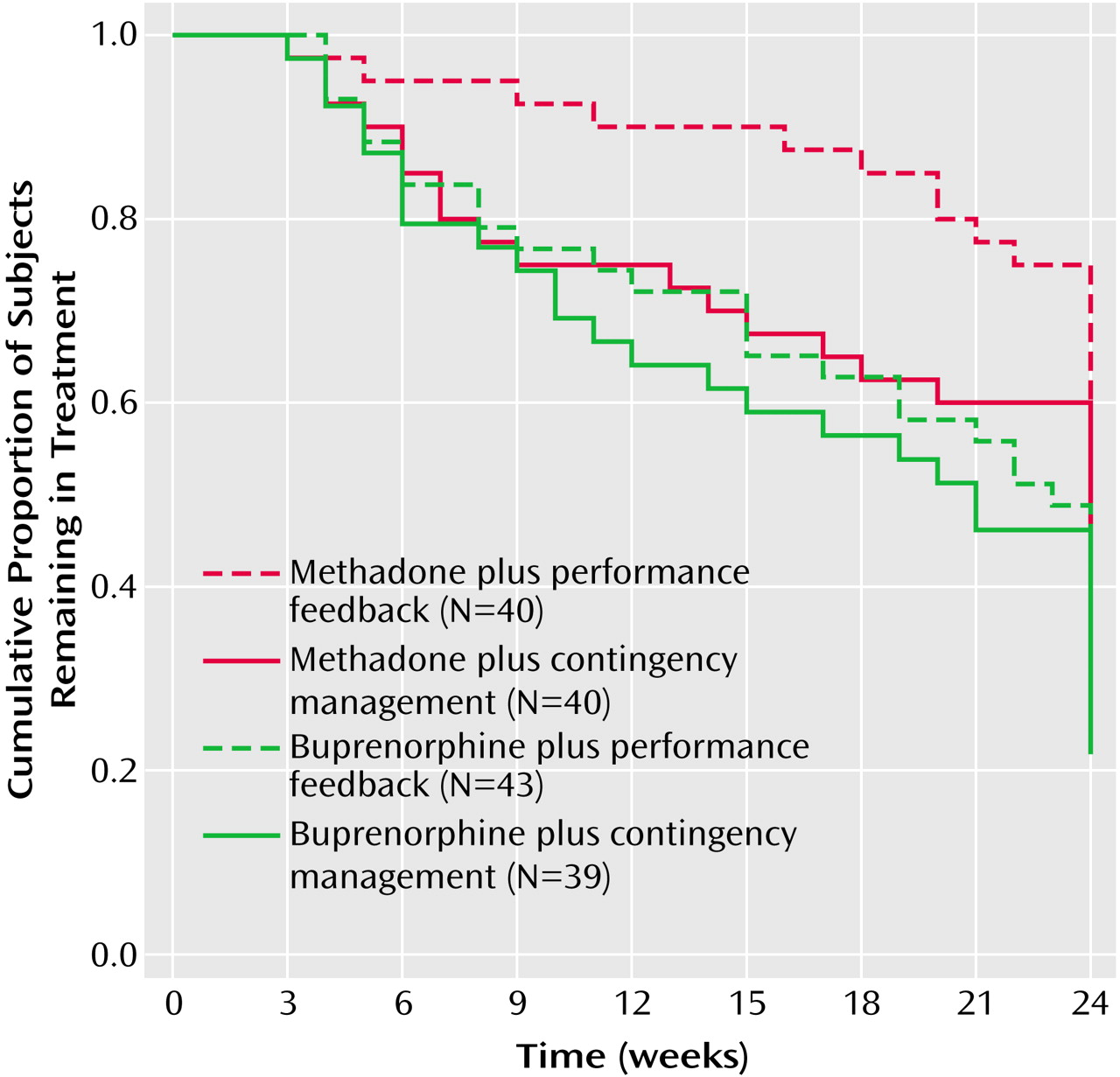
Analysis of variance procedures (for continuous variables) and chi-square tests (for categorical variables) were used to compare the baseline characteristics of patients in the four treatment groups. The differences in retention among the four groups were evaluated by using the Kaplan-Meier survival analysis procedure and the log rank test
(69–
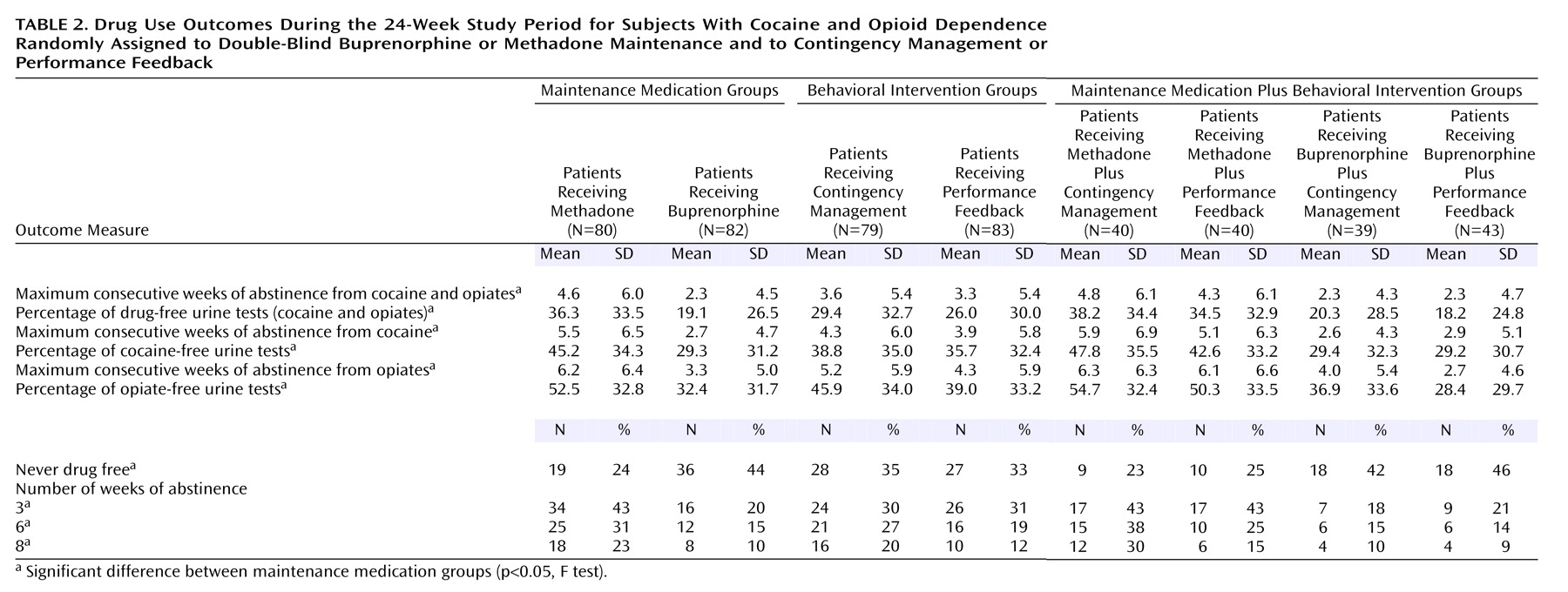
71). The primary outcome measures, assessed by thrice weekly urine testing, were the maximum number of consecutive weeks of abstinence from illicit opioids and cocaine and the proportion of drug-free urine tests. The statistical significance of differences in the maximum consecutive number of weeks of abstinence was evaluated with a two-by-two analysis of variance procedure to test the main effects of the two factors (medication and contingency management) as well as their interaction. The maximum number of consecutive weeks of abstinence provides the best summary measure of varying, arbitrary periods of abstinence (e.g., never abstinent, 1, 3, 6, or 8 weeks of abstinence). For comparison with other studies, we also calculated the proportion of subjects in each group who never had a drug-free urine test or who achieved varying periods of abstinence, and we evaluated the significance of the differences between methadone and buprenorphine maintenance treatment and between contingency management and performance feedback by calculating odds ratios and 95% confidence intervals (CIs). The statistical significance of differences in the proportion of drug-free urine toxicology tests was evaluated by using the mixed-models procedure to test for the main effects of the two factors, time effects during treatment, and possible interactions among the two factors and time
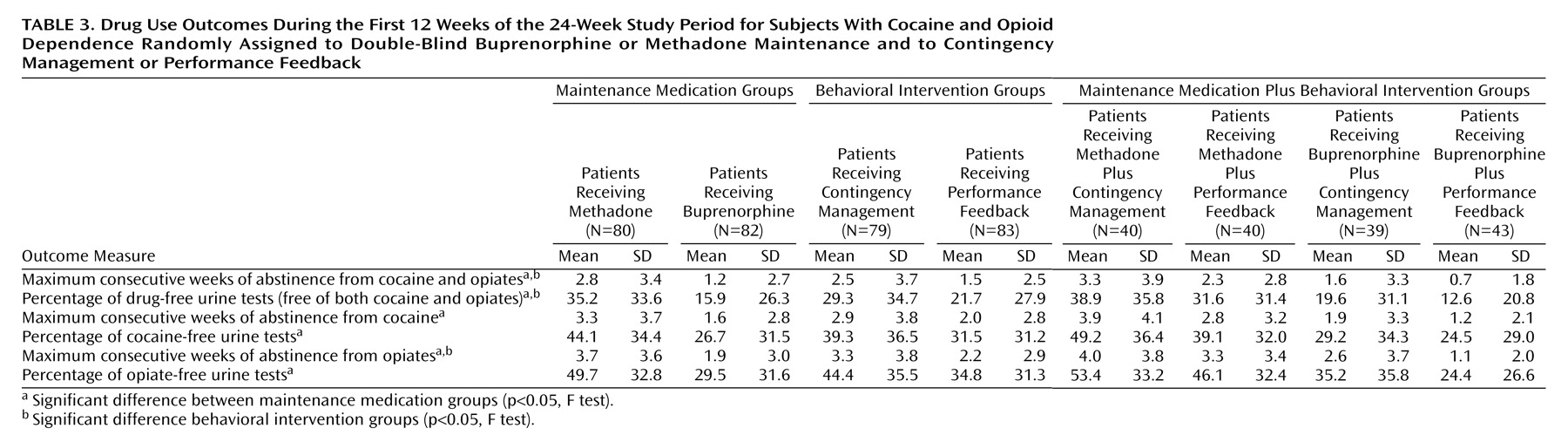
(72). To develop a continuous measure of the proportion of drug-free tests, urine test results were aggregated into eight successive 3-week periods and entered as a repeated outcome measure. Results were also analyzed separately for the proportion of opiate-negative urine tests and of cocaine-negative tests and for the maximum consecutive number of weeks subjects were abstinent from cocaine only and from illicit opioids only. Results are based on 8,201 urine samples (70% of the 11,664 total possible urine samples that could have been collected had all subjects remained in treatment for the entire study). During the time subjects remained in the protocol, 399 of the 8,600 scheduled urine tests (4.6%) were missed. Analyses were conducted for the entire 24-week study period and, to evaluate the effects of contingency management during the time of escalating voucher value, for weeks 1–12.
Because there were significant baseline differences among the treatment groups in race and in the reported number of days of cocaine use in the 30 days before enrollment, we repeated the analyses with adjustment for the effects of these baseline differences. The results of these analyses were similar to those found without adjustment for either variable. Consequently, the results of the analysis of covariance are not reported. Power calculations conducted before the study indicated that the planned sample size of 168 would provide sufficient statistical power (d=0.80) to detect small to moderate treatment effects on the primary outcome measures with an alpha level of 0.05
(73). All analyses were conducted by using SAS version 8.1
(74) and SPSS version 11
(75) statistical packages, with an alpha level of 0.05 and two-tailed tests of significance.
Discussion
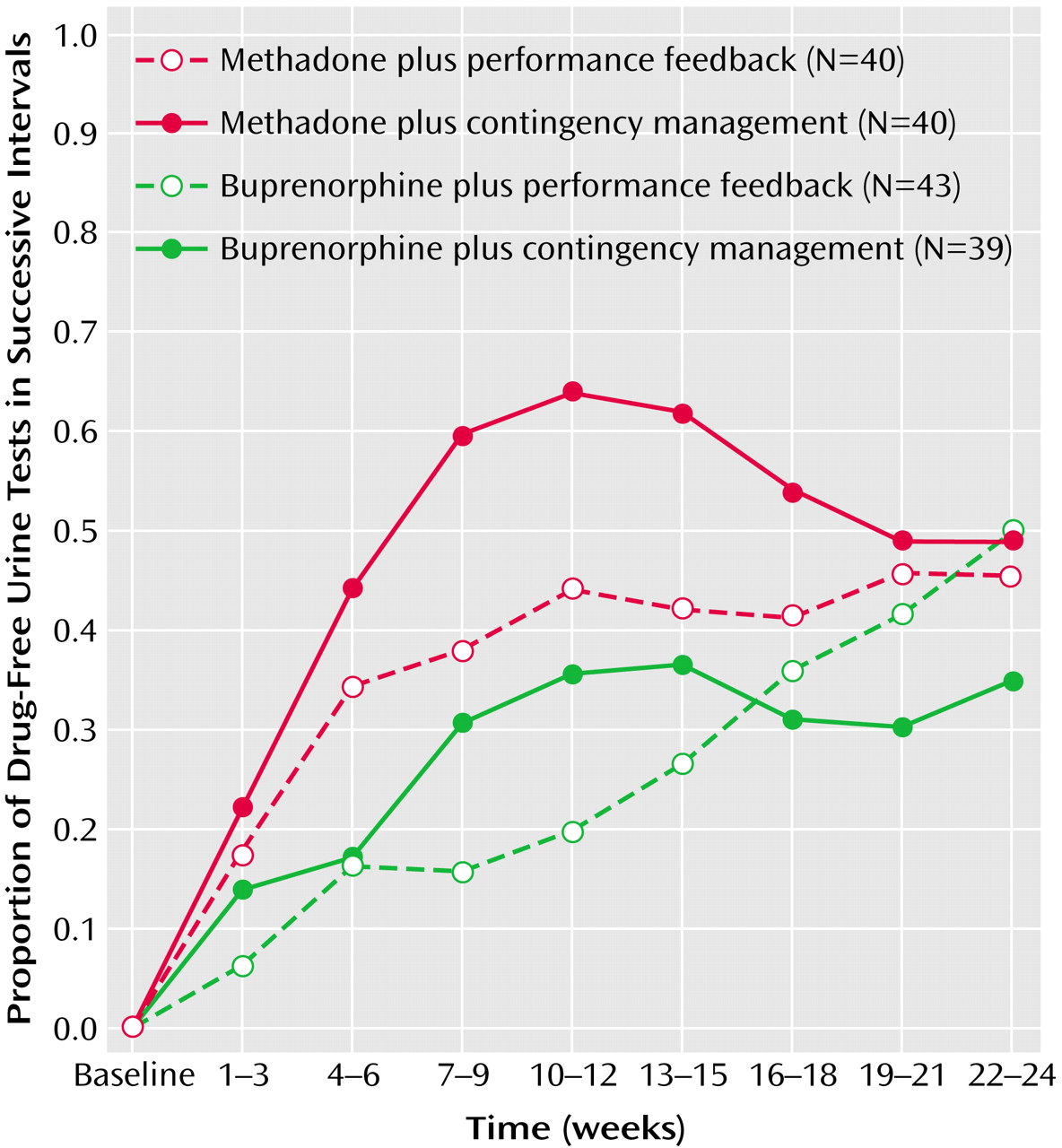
The results of this study support the greater efficacy of methadone maintenance, compared to buprenorphine maintenance, and of combining contingency management with methadone or buprenorphine for concurrent cocaine and opioid dependence. Illicit drug use decreased over time both for subjects who received methadone and for those who received buprenorphine, but the subjects who received methadone remained in treatment longer, achieved longer periods of sustained abstinence from illicit opioids and cocaine, provided a greater proportion of cocaine- and opiate-free urine samples, and experienced a faster reduction in illicit opioid and cocaine use. During the period of escalating rewards for consecutive drug-free urine tests, contingency management was associated with longer periods of abstinence and greater and faster increases in the proportion of drug-free urine tests. No significant interaction was found between maintenance medication and contingency management, suggesting that contingency management improves outcome comparably when combined with methadone or buprenorphine.
The study results favoring methadone are consistent with recent double-blind clinical trials
(40–
44) but not with earlier studies that suggested particular benefits of buprenorphine for concurrent cocaine and opioid dependence
(35–
39). The doses used in this study for both methadone (range=65–85 mg/day, average maximum dose=80 mg) and buprenorphine (range=12–16 mg/day, average maximum dose=15 mg) are comparable to doses typically used in clinical programs and clinical trials during the period when the study was conducted. The protocol allowed dose adjustments of both medications, so that the differences in efficacy are unlikely to be the result of inadequate dosing with buprenorphine. Dose-dependent reductions in illicit opioid use have been found in systematic studies of methadone doses up to 100 mg/day and of buprenorphine doses up to 16 mg of sublingual liquid daily (5, 41, 76–80); even higher doses of both medications are used in clinical practice and may produce additional benefits in patients with continued illicit opioid use at lower doses. Bioavailability of the sublingual tablet formulations of buprenorphine (buprenorphine only or buprenorphine combined with naloxone in a 4:1 ratio) is approximately 80% of the liquid formulation used in this study
(81,
82), and somewhat higher doses may be needed with the tablets.
The benefits of contingency management in this study, evident during the period of escalating reward, were not as pronounced or persistent as has been found in some other studies
(53–
57,
60) but were greater than those reported in other studies of patients receiving buprenorphine maintenance treatment
(58) and of patients receiving methadone maintenance treatment
(59). Several factors might account for the differences across studies. Some studies provided rewards contingent on abstinence from cocaine only
(53–
57), while the current study and some other studies provided rewards contingent on abstinence from both cocaine and illicit opioids
(58–
60). Abstinence from both cocaine and illicit opioids is an important goal, but setting too high a threshold initially for earning a reward may reduce the effectiveness of contingency management. Rewarding abstinence from cocaine only was associated with reduced illicit opioid use in one
(53) but not all
(57) studies. Other differences in study methods involve the counseling procedures and the control for contingency management. Providing manual-guided or specified counseling to all participants, as was done in the current and some (58, 59) but not all (53–57, 60) studies, reduces the likelihood that differences in the counseling provided to patients in one group could lead to observed differences in outcome. To control for the effects of performance feedback and the attention of study personnel in interactions between study personnel and subjects at the time of voucher delivery, this study and two prior studies
(59,
60) provided urine test results to all participants. Other studies did not provide performance feedback
(57) or provided monetary vouchers independent of urine test results
(53,
58) to control for the effects of the additional resources provided with contingency management.
Reflecting the severity of drug dependence in this population, a high proportion of subjects in this and other studies
(53,
58,
59) never provided a single drug-free urine test and thus never had an opportunity to sample the voucher reward. Allowing patients to sample reinforcers, lowering the threshold for earning a reward (e.g., rewarding reductions in use rather than complete abstinence), or providing very high magnitude monetary vouchers may improve the effectiveness of contingency management
(56,
83). Promising alternatives to voucher-based contingency management that may be less costly and more feasible in community treatment settings include the use of an innovative lottery reward system or abstinence-contingent employment or housing
(52,
60,
84–88). Strategies to enhance maintenance of abstinence after discontinuation of aggressive contingency management are also needed. Sustaining a longer duration of initial abstinence (e.g., with more prolonged contingency management) or gradual fading of rewards may help with abstinence persistence
(51,
89).
One limitation of the present study was that contingency management was initiated at the outset of treatment, while subjects were being inducted into the maintenance medication regimens, a period when it might be most difficult for subjects to abstain from opiates and thus have an opportunity to sample the reward. The study design did not allow for a period of stabilization while taking methadone or buprenorphine, because subjects had to be randomly assigned to treatment group (medication and contingency management or performance feedback) at study entry. Differences in retention might also affect analyses of the proportion of drug-free urine tests, but the pattern of results did not change when other approaches for handling missing data (coding missing data as positive or negative or carrying the last value forward) were used. The findings favoring methadone are likely conservative, because drug use generally worsens after dropout from agonist maintenance treatment. The leveling off in effects of contingency management after 12 weeks was also coincident with a reduction in the frequency of community reinforcement approach counseling (from twice to once weekly). Counseling frequency was reduced after 12 weeks for all subjects, however, and subjects assigned to performance feedback showed continued reductions in illicit drug use during the final 12 weeks. Finally, individuals with current alcohol or sedative dependence or significant medical or other psychiatric disorders were excluded from the study, thus limiting the generalizability of the findings.
In conclusion, illicit opioid and cocaine use is reduced by methadone and buprenorphine maintenance treatment. The greater efficacy of methadone for concurrent opioid and cocaine dependence suggests that patients with continued illicit opioid or cocaine use during buprenorphine maintenance treatment might experience improved treatment response with methadone. Contingency management improved outcomes during both buprenorphine and methadone maintenance, supporting the efficacy of combining opioid agonist maintenance with this behavioral treatment. The leveling off of contingency management effects after the value of the voucher was set to a nominal amount as well as the cost and difficulty of implementing monetary voucher rewards
(60,
88) points to the importance of continuing to improve contingency management techniques, evaluating innovative alternatives to voucher rewards, and developing behavioral treatments and counseling approaches that mobilize naturally occurring intrinsic and extrinsic rewards to reinforce abstinence.