The article by Poulsen et al. (
1) published in this issue of the
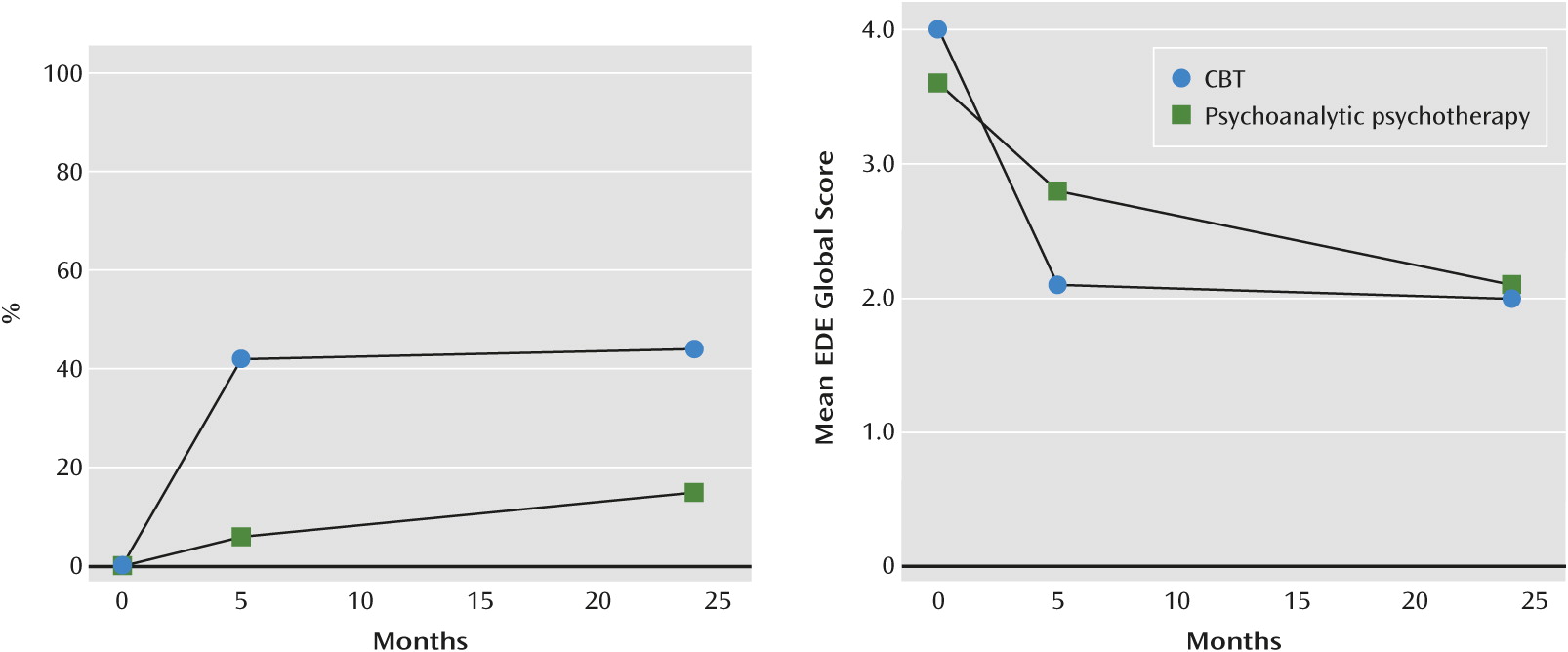
Journal is remarkable in many respects. In this study from Copenhagen, 20 weeks of a new “enhanced” form of cognitive-behavioral therapy (CBT) was found to be markedly superior to 2 years of psychoanalytic psychotherapy. If every figure tells a story, the story told by the left panel of the second figure in the published article (the number of participants who no longer binged or purged) is the most dramatic that we have seen in the literature, and the right panel in that same figure (global eating disorder psychopathology) is also impressive (
Figure 1). These findings stand in stark contrast to the widespread claim that there are no differences in outcomes between the various psychological treatments and that they all work through common (“nonspecific”) processes (
2). Beyond the comparative treatment outcomes, it is also important to highlight the potency of enhanced CBT and the impressive maintenance of change over the 19-month follow-up.
What makes these findings even more striking is that the study was initiated by the two lead authors (who developed the psychoanalytic treatment used in the trial) and it was conducted at a clinic that specializes in psychoanalytic therapy. In the past, differences in outcomes across studies have been attributed to allegiance effects (
3). In this study, the allegiance effects worked against the more efficacious enhanced CBT.
The investigators took particular care to ensure the two treatments were delivered to a high standard. Competence is often confounded with allegiance, although strictly speaking they are not the same (
4). To the extent that they could be disentangled in this study, there was little to suggest an advantage for enhanced CBT. The two sets of therapists received initial training from the experts who developed the two treatments, and the therapists were then closely supervised (albeit off-site via videoconferencing for enhanced CBT). The psychoanalytic psychotherapy therapists were experienced in their approach (17 years on average), whereas the enhanced CBT therapists were distinctly newer to the field (2 years on average). Adherence ratings conducted by independent raters were strong and specific for each approach.
The psychoanalytic treatment enjoyed virtually every advantage over enhanced CBT in this study: a considerably larger dose (more than 70 sessions over 2 years versus 20 sessions over 20 weeks); being delivered at its home site and supervised by the professionals who developed it; and the use of more experienced therapists. Yet enhanced CBT achieved a dramatically better outcome. Moreover, it did so with no indication that it led to symptom substitution, a concern that is rarely mentioned nowadays but that used to be charged against a too rapid (and allegedly superficial) approach to symptom reduction.
Methodological Features
Several features of the study design are worthy of comment. First, the lead investigators are to be commended for pulling in an outside expert to oversee the implementation of enhanced CBT. Trials are often biased against the less preferred intervention simply because it is hard to find comparable expertise and allegiance in the same geographic setting. The authors followed a principle from the cognitive psychology literature in which competing biases are balanced, termed “adversarial collaboration” (
5).
Second, the investigators are also to be commended for maximizing external validity within the confines of a randomized controlled trial. The first impulse of many investigators (and review committees) would have been to equalize the amount of time and contact provided by each treatment even though the two approaches inherently differ in this regard. We applaud their decision to implement each treatment as it is conducted in clinical practice. Doing so did not threaten the internal validity of the study (the ability to draw a causal inference), since the assessment time points were the same for each intervention, while it maximized external validity (generalizability). The only risk the authors ran was to construct validity; had dynamic therapy proven to be no less, or even more, efficacious then enhanced CBT, then it might have been a consequence of the greater amount of contact it afforded (confounding nonspecifics with specifics), but that was clearly not what was found. We are not a little surprised that the project was funded with this much disparity in the amount of therapist contact, but we would have been prepared to argue in support of what the investigators proposed. The design should always fit the question and not the other way around. We salute the authors in crafting their design.
Third, the project breaks new ground with respect to the dissemination of psychological treatments. The enhanced CBT therapists in Denmark were trained and supervised by experts in Oxford using videoconferencing technology. This is an excellent example of the use of technology for training. It greatly expands the scope and scalability of specific, specialized treatments (
6).
Finally, we applaud the candor of the lead investigators for being so forthright in their presentation of the findings. This cannot have been what they hoped to find and indeed was not what they hypothesized (the introduction predicts a lack of differences between the two conditions).
Methodological Caveats
The strengths of the design notwithstanding, we would take issue with some more minor methodological points. No differences were found between the two therapies at long-term follow-up in specific eating disorder or general psychopathology. The authors state, “Both treatments had substantial effects on global eating disorder psychopathology and general psychopathology.” In the absence of a suitable control condition (or differences between conditions) it is not possible to attribute specific causal effects to either treatment on the long-term outcomes of these measures. Closely related is the investigators’ choice to do a nonequivalence trial in an underpowered sample. In this instance, the study was doomed from the start if the respective interventions had not differed in outcome. One need look no further than the recent STAR*D study in the United States to see the risks inherent in not including a control condition. Four thousand patients and 25 million dollars later all we can say is that none of the dozen treatments provided to refractory patients differed from one another, and not whether any of them worked (
7). The authors were saved from interpretive “limbo” by the marked superiority of enhanced CBT over psychoanalytic psychotherapy with respect to binge and purge behaviors.
Why Enhanced CBT Works
The effectiveness of enhanced CBT can be attributed to five main features. First, it directly addresses the mechanisms that research has shown to maintain bulimia nervosa and related eating disorders; namely the overvaluation of body shape and weight, extreme dietary restraint, and sensitivity to adverse events and moods. Second, within the general framework of a structured protocol it is individualized so that it matches the patient's problems. Third, it engages even the most ambivalent patients by providing a comprehensible and credible account of why their eating problem is self-perpetuating and what needs to be changed to overcome it. Fourth, its use of real-time self-monitoring provides a functional analysis of the processes that are currently maintaining the patient's eating problem, and thereby guides the choice of well-established cognitive-behavioral treatment strategies. Lastly, it minimizes the risk of relapse by helping patients develop the ability to identify and correct setbacks as they occur (relapse prevention).
Conclusions
Our sense is that this will prove to be a landmark study as it provides one of the clearest examples of the superiority of one well-implemented psychological treatment over another. This study also provides powerful additional evidence in support of the efficacy of CBT as the evidence-based treatment of choice for bulimia nervosa (
8).