The desire for employment and the benefits of work for the financial and emotional well-being of people with psychiatric disabilities are well known (
1–
6). Yet, 39%–68% of U.S. adults with psychiatric disabilities remain outside the labor force in any given year (
7), and more than 80% of adults receiving public mental health services are unemployed (
8). Moreover, people with psychiatric disabilities represent a significant proportion of beneficiaries of the Social Security Administration’s (SSA) Supplemental Security Income (SSI) and Social Security Disability Insurance (SSDI) (
9), and they rarely attain economic self-sufficiency once enrolled in these programs (
10).
Amid concerns about the role of this population in the rapid growth of the SSI and SSDI programs (
11) and the anticipated depletion of the SSDI trust fund (
12), there have been calls for more widespread implementation of evidence-based supported employment for public mental health clients (
13,
14). There is ample research, including systematic reviews of the evidence (
15–
18) and multistate demonstration programs (
19,
20), showing that evidence-based supported employment services substantially improve employment outcomes for people with psychiatric disabilities. However, analysis of the likely cost-benefit ratio of greater use of supported employment points to gaps in the knowledge base, including its long-term effectiveness (
21).
Supported employment studies typically follow subjects for relatively brief periods. A review of 11 published studies of evidence-based supported employment found that only four incorporated 24 months of follow-up, and the follow-up periods in the remaining seven studies ranged from 6 months to 18 months (
22). One exception is a 5-year study of 100 unemployed individuals with severe mental illnesses in Switzerland who were randomly assigned to supported employment or traditional vocational rehabilitation (
23). At the 5-year follow-up, 28% (13/46) of those in the supported employment group were in competitive work without active support, and another 15% (7/46) were competitively employed with support from an employment specialist.
Other smaller, nonrandomized studies have examined outcomes over 10–12 years of continuous supported employment services. In one such study, a 10-year follow-up of 36 individuals (58% of the original sample) found that 75% of ongoing supported employment participants had worked at all after the initial 18-month study period, including 68% in competitive jobs, although none were currently employed full time (
24). A similar follow-up study (
25), which included 38 participants in a nonrandomized trial of ongoing supported employment services (49% of the original sample), found that all had worked at some point during the 8–12 years after the study ended, including 24% (9/38) who were in competitive jobs.
In larger long-term studies using SSA administrative data on SSI and SSDI beneficiaries with a wide range of chronic disabilities, estimates are that 18%−28% of program participants work at all over the course of up to 10 years of follow-up and that 4%−10% of participants are suspended or terminated from receiving cash benefits at least once during that period due to work (
26). In an SSDI cohort observed from 1996 to 2006, 28% returned to work, 6.5% had their benefits suspended due to work in at least 1 month, and 3.7% had their benefits terminated due to work. The corresponding percentages were much higher for those who were younger than age 40 when they entered the SSDI program. Most first suspensions occurred within 5 years after program entry. There was considerable variation across states, and outcomes appeared to decline for more recent cohorts, possibly as a result of the 2008 economic downturn in the U.S. economy. In research on an SSI cohort followed over a similar interval, 18.6% worked, 8.4% had their SSI payments suspended because of work, and 9.8% had their payments suspended or terminated because of work (
27).
More information about the long-term effects of supported employment is needed, especially in the context of current discussions about expanding access to supported employment for SSI and SSDI beneficiaries with psychiatric disabilities (
13,
21). We address this knowledge gap by examining the long-term impact of evidence-based supported employment services on three vocational outcomes: labor force participation, earnings, and attainment of SSA’s SSI and SSDI nonbeneficiary status through suspension or termination of disability cash payments for work (NSTW). We hypothesized that individuals with psychiatric disabilities who received supported employment services for up to 2 years would be more likely than those who did not to be engaged in the labor force across an ensuing 13-year period; that these individuals would have their SSI and SSDI cash benefits suspended or terminated for at least 1 month due to work activity; and that these individuals would have higher earnings during the follow-up period.
Method
The Employment Intervention Demonstration Program (EIDP) was a 5-year study of supported employment programs for people with severe mental illnesses, funded by the Center for Mental Health Services at the Substance Abuse and Mental Health Services Administration (
19,
28). Participants met the following study inclusion criteria: age 18 years or older; having a DSM-IV axis I diagnosis of mental illness; desiring employment; being unemployed (except at one site); and providing informed consent. Participants (N=1,648) were enrolled from 1996 to 1998 at eight sites in four U.S. geographic regions (Northeast, Mid-Atlantic, Southeast, Southwest) and were followed for 24 months, from 1998 through 2000. Participants provided written informed consent and were monetarily compensated (amounts varied from $10 to $20 per interview). Hereafter, we refer to this initial 2-year period of services and data collection as the EIDP study.
After enrollment, participants were randomly assigned to study condition. The control condition was defined as either usual services alone or usual services plus unenhanced vocational rehabilitation services. The experimental condition consisted of evidence-based supported employment services delivered by employment specialists on multidisciplinary teams that met frequently to coordinate employment and clinical services; the goal of these services was placement in competitive jobs that met patients’ career preferences, using a job search process beginning soon after program entry and providing vocational supports throughout the study.
Six of the eight EIDP sites also participated in a supplemental study conducted during the EIDP study. This supplemental study was designed to collect detailed information about the economic situations of adults with psychiatric disabilities. Of the 867 supplemental study participants, 505 (58%) provided consent to have their information matched to SSA administrative data. We verified 487 of these 505 individuals (96%) with SSA files using the Enumeration Verification System. Of these 487 individuals, 35 had no records in SSA’s Disability Analysis File, indicating that they had not participated in the SSI or SSDI programs from 2000 to 2012, and another three died prior to 2000, resulting in a sample size of 449. Disability Analysis File data were compiled for these 449 individuals for calendar years 2000 through 2012. Hereafter we refer to this 13-year data compilation and analysis as the EIDP long-term follow-up study.
The 449 long-term follow-up study participants did not differ statistically from the supplemental study's respondents in the larger EIDP cohort in terms of age, gender, race, diagnosis of depression or bipolar disorder, history of substance abuse or dependence, psychiatric hospitalization, study condition, or employment outcomes (i.e., worked at all or attained competitive employment) during the EIDP study. However, long-term follow-up study participants did differ from the remainder of EIDP participants in ways that were associated with poorer vocational outcomes, such as being less likely to work in the 5 years prior to study baseline (64% of long-term follow-up participants compared with 69% of other EIDP participants; χ2=4.25, p=0.039), being more likely to be diagnosed with schizophrenia spectrum disorders (54% compared with 46%; χ2=8.54, p=0.003), being more likely to have co-occurring medical conditions (44% compared with 35%; χ2=10.61, p=0.001), and being more likely to have been SSI and/or SSDI program beneficiaries during the EIDP study (86% compared with 80%; χ2=11.24, p=0.001). In addition, there was regional variation in the proportion of EIDP subjects who were also long-term follow-up participants: 50% of the Northeast region EIDP subjects also participated in the long-term follow-up; 49% of the Southeast region EIDP subjects participated in the long-term follow-up; 38% of the Southwest region EIDP subjects were long-term follow-up participants; and 17% of the Mid-Atlantic region EIDP subjects were long-term follow-up participants (χ2=88.66, p<0.001).
Measurements
The independent variable in our analysis was assignment to evidence-based supported employment or to the control condition. Three dependent variables from the Disability Analysis File served as outcomes. The first was labor force participation, which was defined as having any reported earnings from work. The second outcome was achievement of NSTW. The third outcome was amount of earnings from work. Covariates included demographic characteristics such as race/ethnicity (black, Hispanic), gender (male), age (in 10-year increments), education at time of study entry (less than high school education compared with high school education or more as a reference), and geographic region (Northeast, Mid-Atlantic, and Southeast, with Southwest as reference). In addition, clinical factors associated with outcomes in univariate analyses also were controlled for in the multivariable models. These factors included psychiatric diagnosis (schizophrenia spectrum disorder compared with other) and history of substance abuse or dependence as assessed by a clinician (any compared with none), both of which were negatively associated with study outcomes.
Statistical Analysis
We examined participant characteristics and summary outcomes, comparing differences by study condition using chi-square tests and analysis of variance. We analyzed longitudinal data using random-effects logistic and linear regression models, adjusting for the effects of time, for correlations of repeated measures, for unbalanced study attrition, and for participant demographic and clinical characteristics (
29). Participants were right-censored on program exit due to mortality, which occurred for almost a quarter (24.5%) of the sample.
Results
Long-term follow-up participants did not differ significantly by study condition in demographic and clinical characteristics, as shown in
Table 1. Participants were most frequently non-Hispanic white (52%), male (52%), and diagnosed with schizophrenia (54%); had a history of substance abuse or dependence (54%); had at least a high school education (73%); and had an average age of 38.4 years. Most reported receiving SSI benefits (70%) or SSDI benefits (56%) during their 2 years of EIDP participation. During the EIDP study, long-term follow-up subjects who had received supported employment had significantly better outcomes than participants in the control condition in terms of achieving competitive employment (56% compared with 36%; χ
2=17.57, p<0.001), and they were generally more likely to have worked at all (72% compared with 63%; χ
2=3.74, p=0.053). On average, supported employment participants worked more total hours and earned more total dollars than control subjects, although these latter differences were not statistically significant.
Table 2 presents descriptions of summary vocational outcomes by study condition aggregated across all 13 follow-up years (2000–2012). About a third (32.9%) of all participants worked at some point during the long-term follow-up period (i.e., reported countable income). Over 13 years, participants had an average of 10.5 months with any earnings. Total earnings averaged $6,453 per person among all subjects and $19,578 per person among those who worked. Among all participants, 13.1% achieved NSTW, with an average of 4.5 months in suspension or termination status during the 13-year follow-up period. Supported employment participants had superior but nonsignificant summary outcomes, although the higher total earnings of the supported employment group ($7,855) compared with the control group ($4,928) approached statistical significance (p=0.099). Over the 13-year follow-up period, 71% of participants were SSI beneficiaries, and 58% were SSDI beneficiaries. Finally, use of work incentive programs by all participants was low, with the Plan to Achieve Self-Support provision used in <1% of follow-up months and the Ticket to Work program used in <3% of follow-up months (data not shown).
We used multivariable random-effects logistic and linear regression models to compare outcome measures in the supported employment and control conditions over time, and we adjusted all models for time, age, race/ethnicity, gender, education, schizophrenia diagnosis, substance abuse history, and geographic region (
Table 3). In the multivariable model for any earnings over 13 years, the supported employment recipients were almost three times as likely as control subjects to be employed (odds ratio=2.89, p=0.022). In addition, both the supported employment group and the control group showed a small but significant decline in the likelihood of having any earnings over time (odds ratio per month was 0.99, p<0.001). Men were more likely than women to have earnings from work (odds ratio=2.71, p=0.040), and older people were less likely than younger people to have been employed (odds ratio=0.75, p<0.001 per 10-year increment in age). Those with schizophrenia spectrum disorders were more likely to have earnings (odds ratio=4.61, p=0.003), while people with a history of substance abuse were less likely to have reported earnings (odds ratio=0.38, p=0.042).
In the longitudinal analysis of achievement of NSTW, people in the supported employment group were notably more likely than control subjects to be in NSTW (odds ratio=12.99, p<0.001). Again, both groups showed a decline in likelihood of NSTW over time (odds ratio per month was 0.99, p<0.001). Older age and substance abuse history were again associated with lower likelihood of NSTW (odds ratio=0.39, p=0.010; and odds ratio=0.06, p<0.001, respectively), as was residence in the Northeastern region (odds ratio=0.10, p=0.029). Finally, people with a schizophrenia spectrum diagnosis were significantly less likely to be in NSTW than those with other diagnoses (odds ratio=0.14, p=0.005).
In the third set of analyses, those who had received supported employment had significantly higher earnings per month than control participants over time (a difference of +$23.82, p=0.047). In addition, there was an overall decline in earnings per month for both groups over time (a difference of −$0.25, p<0.001). Age (in 10-year increments) was the only covariate significantly associated with earnings, with lower earnings associated with increased age (a difference of −$16.32, p=0.013).
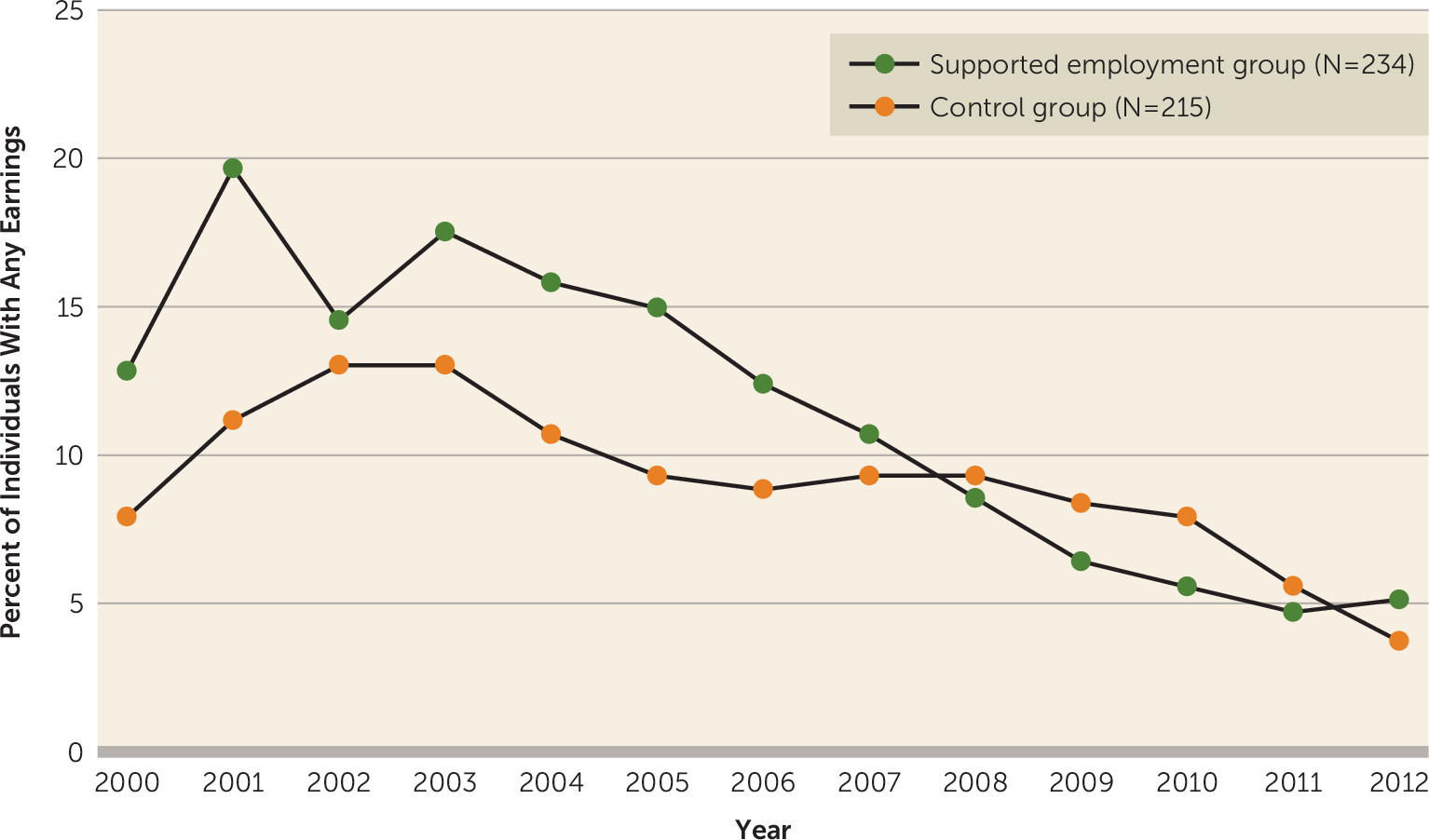
Observed longitudinal outcomes are illustrated in the figures. In
Figure 1, the higher proportion of supported employment participants with earned income compared with control participants is clear until about two-thirds of the way through the follow-up period, in 2008. The overall decline in work over time in both groups is seen, and the percentage of working participants declined to less than 5% by 2012.
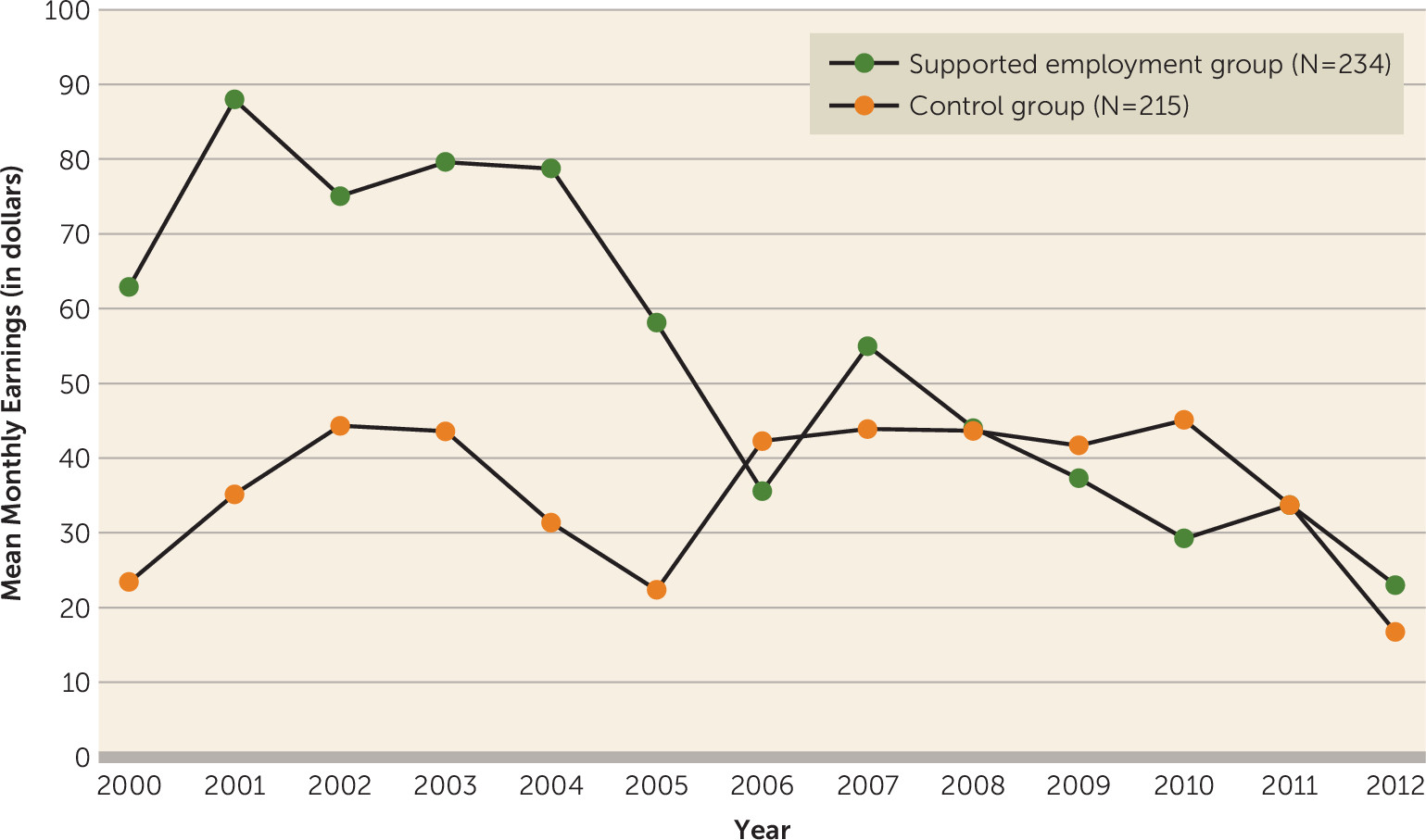
Figure 2 shows a higher proportion of supported employment participants compared with control subjects in NSTW until about 2008, with an overall decline evident for both groups over time. In
Figure 3, a similar pattern is seen for earnings among all participants. In 2000, mean monthly earnings were $62.91 among supported employment participants and were $23.41 among control participants, declining by 2012 to $23.02 and $16.76, respectively.
Discussion
Our study findings indicate a significant vocational advantage accruing to recipients of evidence-based supported employment in the decade following service delivery. This was true for having any earnings from employment, for the amount of earnings, and, most notably, for achievement of nonpayment status following suspension or termination of SSI or SSDI cash benefits due to work. In terms of sample size, length of follow-up period, and use of SSA disability file data, this study of long-term effects of supported employment is unique.
It is interesting to note that the outcomes of supported employment recipients in the EIDP long-term follow-up study were superior to those reported among working-age individuals with disabilities who began receiving SSI disability payments from 1996 through 2006 (
27). Higher proportions of our study participants had any earnings and had payments suspended or terminated due to work than national cohorts of beneficiaries. For example, 35.5% of EIDP long-term follow-up participants worked, compared with 18.6% of the 2001 national SSI award cohort. Similarly, 15.0% of participants in the EIDP long-term follow-up achieved NSTW, while only 9.8% of the national SSI award cohort did so. Supported employment outcomes in the EIDP long-term follow-up group are also superior to those of SSDI beneficiaries reported (
26) for the 1996 award cohort (which is closer to the time of SSDI entry for the EIDP participants). Of the 1996 SSDI cohort, only 28% achieved employment, 6.5% reached nonpayment status through suspension due to work, and 3.7% reached nonpayment status through termination due to work.
We observed noteworthy decreases in outcomes over time that may have been due to declining labor force participation as the cohort aged, exacerbated by the economic downturn of 2008. This finding also may be an artifact of incomplete data in the Disability Analysis File for later years (2010–2012) because of lags in the processing of work reviews. The processing of both NSTW and earnings data takes longer for SSDI beneficiaries than for SSI beneficiaries and may account for the observed declines in both groups. Yet another minor contributor to declining outcomes is that a small percentage of participants who successfully left the SSI and SSDI disability programs were not represented in the later years of follow-up and, as a result, our sample represents long-term beneficiaries unlikely to exit the rolls. It is noteworthy that the amount of earnings was relatively small and not at all close to the substantial gainful activity threshold ($1,010 a month for nonblind beneficiaries in 2012), which makes our finding regarding proportions achieving nonpayment status all the more compelling.
In general, older program beneficiaries had poorer long-term work outcomes. This finding adds to the evidence from previous research showing that the proportions of individuals who had earnings and who were in suspension or termination status were much higher for those who were younger than age 40 when they entered the SSDI program (
26). In addition, those with histories of substance abuse had poorer long-term work outcomes, a finding that may reflect research that has shown lower interest in working and poorer work outcomes among people with dual diagnoses of mental illness and substance abuse, although results have been inconsistent (
30,
31).
We found that program beneficiaries with schizophrenia spectrum disorders were more likely than those with other diagnoses to work; however, they were less likely to be in NSTW. This may reflect generally lower sustainable employability because of social, vocational, or functional limitations (
32) even among those who successfully apply for and attain SSI or SSDI beneficiary status (
33). Previous research has shown that, among people with schizophrenia, clinical symptoms are barriers to any employment, but receipt of disability benefits is specifically associated with less likelihood of competitive employment (
34). In our long-term follow-up group, participants with schizophrenia may have been able to work but unable or unwilling to have higher earnings or risk beneficiary status.
We did not find regional differences in likelihood of any earnings or in amount of earnings over time, but the Northeast region was associated with lower likelihood of being in NSTW. Studies of larger cohorts of SSA disability program beneficiaries have found considerable state variation in NSTW, possibly attributable to regional differences in use of SSA work incentives and in access to public health insurance and vocational services (
26,
27).
A number of caveats bear mentioning with regard to our study findings. First, we did not examine a nationally representative sample of adults with psychiatric disabilities, and thus our results are not generalizable (although we did have participants from different regions of the United States). Second, the study population consisted of paid volunteer subjects who were interested in working, a group that may not be representative of the broader population of individuals with psychiatric disabilities. Third, our findings may have been affected by incomplete earnings data for beneficiaries who had left the rolls, as well as because of lags in the processing of work reviews during the later years (2010–2012). Fourth, it is possible that unmeasured underlying demographic characteristics of the study sample contributed to the effect of region that we found, although our data do not allow us to explore this possibility. Fifth, it is possible that participants in either study condition received supported employment or other vocational rehabilitation services after the EIDP study, although research shows that this is rare (
20). Sixth, not all sites in the original EIDP study participated in the long-term follow-up study, which may have introduced regional and local biases to our analysis. Finally, although all EIDP interventions met supported employment criteria (
19), not all sites implemented the current best-practice individual placement and support model (
21), which may have diluted intervention effects.
It also is important to note limitations in study scope. We were not able to address nonvocational outcomes associated with supported employment, such as mental health, social inclusion, and quality of life (
35), or to address the cost-effectiveness or social cost-benefit ratio of the supported employment intervention (
21).
In summary, we provide the strongest research support thus far for the long-term effects of evidence-based supported employment services on employment, earnings, and attainment of NSTW among SSI and SSDI beneficiaries with psychiatric disabilities. Although participants did not generally achieve economic self-sufficiency, the significant positive supported employment intervention effect adds to the ever-expanding evidence base regarding ways to help career-oriented workers escape from a cycle of poverty and dependence on Social Security disability benefits. These strategies include increased funding, interagency collaboration, and early intervention efforts to bring supported employment services to larger numbers of disabled workers in order to reduce their dependence on public disability payments by enabling them to hold jobs that pay a living wage. A recent analysis suggests that expanding access to supported employment would be unlikely to result in drastic budgetary savings to SSA; nonetheless, this model is more cost-effective than other vocational rehabilitation programs and results in beneficial social and personal outcomes, which are positive arguments for increasing funding and expanding access (
21). A systematic, policy-driven approach to expanding supported employment would benefit from greater interagency understanding (
9). Finally, while best-practice supported employment models such as individual placement and support are well established, expanded use and access should be informed by research-based innovations in delivery, including early intervention and cognitive enhancement treatment (
36,
37). Hopefully, future research will give us additional guidance regarding who is most likely to achieve long-term benefits from supported employment, as well as whether and how to deliver this model to individuals early in or even prior to the disability determination process.