Hepatitis C virus (HCV) is one of the leading causes of preventable death worldwide and the most common blood borne infection in the United States.
10 An estimated 2.7 to 3.9 million Americans are living with HCV.
11 Most patients are asymptomatic, and up to 75% with chronic HCV remain unaware of their status until liver problems develop.
11–13 Current treatments for chronic HCV include direct-acting antivirals, which have shown to achieve sustained virologic response (SVR) in 90% or more of patients.
14,15 Eradication of HCV peripherally is unambiguously associated with clinical improvement. However, there is growing evidence that a substantial proportion of patients have impairments that appear to be unrelated to viremia. Most concerning is the presence of HCV in the central nervous system of some patients.
Though HCV primarily infects the liver, factors that are necessary for viral uptake and cell entry are not solely expressed in liver-derived cells. HCV has been detected in multiple organs including lymph nodes, bone marrow, pancreas, thyroid gland, adrenal gland, and spleen.
16 Between 40%−75% of patients with HCV experience extrahepatic effects (e.g., mixed cryoglobulinemia, arthralgia/myalgia, autoantibody production).
12,17–19 HCV is also associated with a higher prevalence of cardiovascular and cerebrovascular disease, inflammatory related problems, type II diabetes, renal insufficiency, and peripheral neuropathy.
17–20The belief that mild HCV is typically asymptomatic has been challenged in recent years. Patients with HCV report poorer health related quality of life (HRQoL) in multiple domains of functioning.
3,19–25 Common functional problems include chronic fatigue, depression, and insomnia. As noted in a recent review, the substantial associations among these conditions (
Figure 1) complicate identification and management.
25 Although evidence varies, inattention, poor working memory, poor learning, and slowed psychomotor speed are the most commonly noted cognitive problems. When cognitive deficits are present, they tend to be mild.
26,27 Notably, studies generally do not account for confounding factors present in this population (e.g., depressive symptoms, chronic fatigue) that can significantly influence cognitive performance, making it unclear whether HCV has any direct effects on cognition. A systematic review of studies found that HCV eradication led to improved functioning (e.g., HRQoL, cognition).
28 However, patients who attained SVR (SVRs) were still impaired compared with healthy individuals. More recent studies have confirmed modestly improved functioning in SVRs posttreatment compared with individual baselines and to treatment nonresponders.
29–35 Patients with more severe liver disease may have greater functional gains.
34 Overall, these results indicate that peripheral viral clearance decreases impairments but does not result in return to baseline levels of functioning in all HCV patients. The pathophysiological basis for these impairments is an area of debate.
Having a diagnosis of HCV is proposed to be a psychosocial factor that negatively affects self-perceived HRQoL.
24,27 A set of studies in voluntary blood donors obtained HRQoL from donors with positive initial tests at the time of confirmatory testing and after notification of the results.
36,37 Prior to confirmatory testing, donors with initial positive tests reported lower scores on multiple HRQoL domains than matched (age, sex, race) blood donors with negative tests.
36 When the group was divided based on the latter confirmatory test results, donors that were true positives had reported generally lower scores than donors who were false positives on multiple domains, but only physical role and emotional role components were statistically different.
37 The groups differed significantly on the additional components of vitality and social functioning following notification of confirmatory test results, due primarily to improved scores in the false positive group, perhaps indicating relief from stress associated with initially testing positive. At clinical follow-up of the true positive group, improvements were observed in multiple domains. As noted by the authors, these results support the beneficial effects of receiving appropriate counseling and other clinical care.
36,37Studies assessing hepatic encephalopathy (HE) have reported presence of minimal HE in a substantial proportion of HCV patients.
15,38–41 Minimal HE is defined by impaired performance on cognitive tests in the absence of clinical manifestations of liver disease. A recent study utilizing hierarchical clustering analysis identified multiple patterns of deficits.
41 The authors speculated that this symptomatic heterogeneity suggests involvement of different brain systems and potentially different underlying mechanisms across patients.
41 This is consistent with an earlier proposal of neurocognitive disorder due to HCV that is distinct from minimal HE.
15 Multiple pathophysiological mechanisms have been proposed for these impairments in brain functioning.
15,38–40,42 Some are related to liver dysfunction (e.g., hyperammonemia-induced brain edema, release of proinflammatory substances into the circulation). Others are secondary to the wide range of co-occurring conditions (e.g., renal dysfunction, hyponatremia, diabetes, sepsis, cardiovascular disease). Mechanisms secondary to HCV infection of the brain have also been proposed.
Functional neuroimaging provides multiple approaches to noninvasive assessment that may provide insight into pathophysiology. The methods that have been most commonly utilized in relevant studies are proton (
1H) magnetic resonance spectroscopy (MRS), diffusion tensor imaging (DTI), and positron emission tomography (PET). Proton MRS provides noninvasive measures of several metabolites (after suppression of the signal from water) that are sensitive to changes in neuronal and glial state and/or density.
2,3 The most commonly assessed metabolites include N-acetylaspartate (NAA; considered a marker for neurons/axons because it is located primarily in mature neurons), choline-containing compounds (Cho; considered a marker for cell turnover and membrane metabolism), creatine and phosphocreatine (Cr; considered a marker of cellular energy metabolism), and myoinositol (mI; considered a marker of glial cells because it serves as an intraglial osmolyte). In general, metabolites are normalized (reported as a ratio) to Cr. Cr is used as an internal standard because its level is thought to be stable; however, there is evidence that Cr level may be altered by some disease conditions, including neuroinflammation.
2 Diffusion tensor imaging (DTI) is a type of magnetic resonance imaging that provides metrics for the speed and direction of water diffusion within the voxel. Mean diffusivity (MD) is an averaged measure of speed of diffusion in the three main directions. Fractional anisotropy (FA) is a measure of the degree to which diffusion is faster in one direction than others, and is highest in voxels containing highly parallel densely packed axons. Reductions in FA and elevations in MD are thought to indicate impaired white matter integrity. Microglial state is also assessed using the positron emission tomography (PET) ligand PK11195, which binds to the mitochondrial membrane translocator protein (TPSO) present in endothelial, astroglial, and microglial cells. It is generally considered a marker for microglial activation.
Several changes in neuroimaging metrics are considered to characterize individuals with minimal HE compared with healthy controls.
3,4,42–46 Changes on proton MRS (expressed either as concentrations or referenced to Cr) include decreases in mI and Cho, and normal levels of NAA (
Cover and Figure 2). For DTI, the most characteristic change is increased MD in most or all areas assessed, and normal FA. Two recent studies have assessed the value of specific metrics for differentiating patients with and without minimal HE.
4,44 A study that compared MRS measures reported that the group with minimal HE had higher levels of glutamate (no difference in glutamine) than the group without; whereas mI did not differ significantly between groups.
44 A study that included both MRS and DTI reported that greater changes in all metrics were present in the minimal HE group, but that higher MD discriminated presence of minimal HE better than any of the MRS metrics.
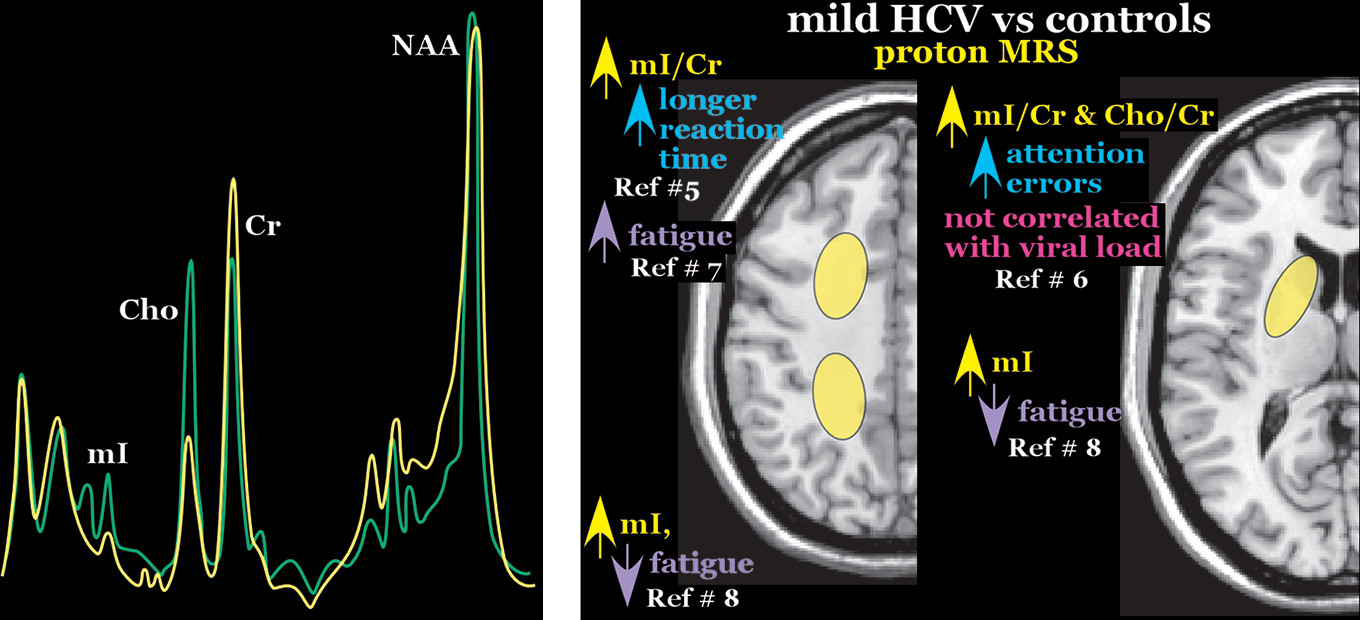
4The changes on neuroimaging metrics reported in studies comparing patients with mild HCV (positive for the virus but no cirrhosis) to healthy individuals differ greatly from those considered to characterize minimal HE. Although studies vary considerably in the area(s) of brain most affected, mild HCV is characterized on proton MRS by higher mI (or mI/Cr), higher Cho (or Cho/Cr), and often lower NAA (or NAA/Cr).
5–8,47–49 Two groups have reported that elevated mI/Cr in the frontal white matter and/or basal ganglia correlated with greater fatigue and/or poorer cognitive performance in some domains (working memory reaction time, processing speed, language fluency), suggesting that microglial activation is detrimental (
Figure 2).
5–7 In contrast, another group reported significant elevations in parietal white matter mI only for the subset of HCV patients without pathological levels of fatigue. There were no differences when grouped by depression or attention performance.
8 This study reported a negative correlation between fatigue and mI concentration, supporting a beneficial effect for microglial activation (
Figure 2).
8 Another study reported elevations in frontal white matter Cho/Cr and NAA/Cr in mild HCV that correlated with greater severity of depression and higher fatigue.
26 Two studies compared MRS metrics prior-to and following treatment.
29,30 One reported increased Cho/Cr in the basal ganglia in SVRs, but not improved cognitive performance.
29 The other study reported decreased mI/Cr and Cho/Cr in the basal ganglia in SVRs accompanied by improvement on some domains of functioning.
30 Both studies that utilized DTI reported that MD was increased in only a few of the areas assessed.
7,47 One study reported decreased FA in all white matter areas measured.
47 The other found no differences in FA of white matter areas, but increased FA in striatum, thalamus, and insula.
7 Higher striatal FA correlated with poorer cognitive performance.
7 Following treatment, only the SVRs with improved cognitive performance showed evidence of improved white matter integrity (increased FA and/or decreased MD).
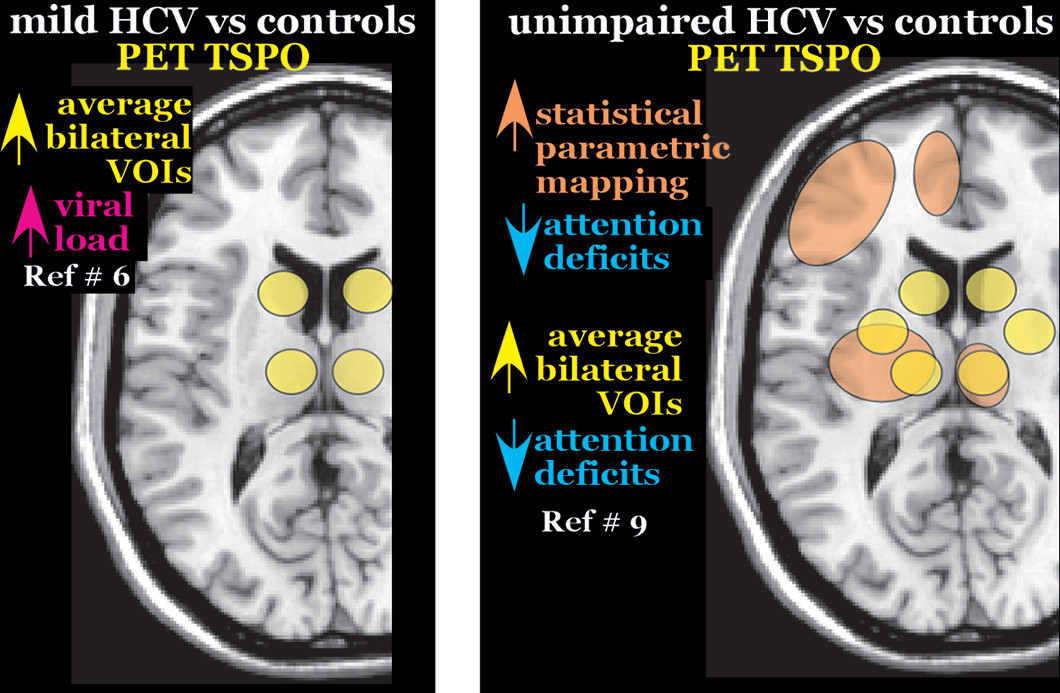
35 Studies from two research groups have compared PET TSPO binding in patients with mild HCV to healthy controls.
6,9 One study reported significantly higher binding potential in all subcortical areas assessed (caudate, thalamus, pallidum) but in no cortical areas (frontal, parietal, temporal, occipital) (
Figure 3).
6 Higher binding potential in thalamus (trend for caudate) correlated with higher viral load. In turn, higher viral load correlated with greater fatigue. No PET metric correlated with cognitive performance or with MRS metrics.
6 The other study reported no differences between patients with mild HCV and healthy controls.
9 Higher binding potential was reported in frontal cortex only for the subgroup of patients no longer positive for the virus. The substantial differences across studies in changes of functional imaging metrics and direction of associations (i.e., positive, negative) with functional status in groups with mild HCV suggest that the underlying neurobiological states may vary considerably in this patient group.
Studies in cohorts of HCV patients without cirrhosis or relevant complicating conditions (e.g., other viral infections, history of substance use) have reported similarly high rates of impairment (e.g., HRQoL, sleep, depression, fatigue, cognition) in subgroupings based on viral testing (negative or positive)—even decades after initial infection.
1,9,27,50 One study found 42% of the HCV group that had cleared the virus had impaired HRQoL, compared with 47% of the group that still tested positive.
27 Logistic regression identified depression and fatigue as important factors influencing impaired HRQoL. Another research group has done a series of studies examining different aspects of functioning.
1,9,50 In one study, they found that 95% of their HCV group reported disturbed sleep, despite 40% having cleared the virus.
50 Measures of HRQoL, depression, and fatigue were significantly correlated with measures of sleep, suggesting depression as a possible mediator of impaired sleep quality. Their most recent study reported that a much greater proportion of HCV patients had pathological levels of neuropsychiatric symptoms (e.g., fatigue, anxiety, depression) than were impaired on cognitive testing regardless of viral status.
1 Additionally, HRQoL was negatively associated with fatigue, depression, and attention (
Figure 1). Notably, attention was also independently associated with fatigue. The cognitive measure with the highest rate of impaired performance was not correlated with any neuropsychiatric symptom domain or with attention, but was positively correlated with time since infection. These results support the importance of pathophysiological mechanisms other than viremia, and suggest independence between cognitive and functional impairments.
1 Findings from their small study comparing PET TSPO between HCV patients and healthy individuals is consistent with this hypothesis.
9 TSPO binding potential was higher in the HCV subgroup with intact attention than in healthy controls in subcortical (putamen, caudate, thalamus) volumes of interest (VOIs) (
Figure 3). In contrast, TSPO binding was higher in the HCV subgroup without fatigue than in healthy individuals in the temporal cortex.
9 As noted by the authors, these results support microglial activation as a beneficial process.
The pathophysiological mechanisms of cognitive and functional problems as well as sleep disturbance in HCV patients, in the absence of viremia, remain poorly understood. Proposed mechanisms include direct infection of the brain, chronic neuroinflammatory response, indirect stimulation of neurotoxic cytokine pathways, as well as the development of cerebral vasculitis.
18,19,21,22,51 Most concerning, although sample sizes are relatively small, is the mounting evidence that HCV infection can spread into the brain.
3,20,22–24 The presence of HCV RNA in cerebrospinal fluid (CSF) of HCV-infected patients was the first indication. The possibility that HCV directly infects brain cells is supported by the presence of HCV negative strand RNA (a replicative intermediate) or other molecules linked to HCV replication in samples of postmortem brain tissue.
52,53 Both studies reported glia as the major cell type infected, but differ on whether microglia or astroglia are more involved. HCV was relatively less abundant in brain than liver specimens.
22 It has been suggested that the low levels of viral replication might not induce a sufficient immune response, therefore possibly supporting a chronic, persistent infection.
24 In addition, these findings could also indicate passage of infected peripheral blood mononuclear cells (PBMCs) into the brain. The detection of different HCV strains (quasispecies) in brain and serum provide support for genetic compartmentalization and the hypothesis that there is independent viral evolution in the two sites of replication.
3,20,22,23Most recently, the possibility of independent viral evolution was investigated using a deep sequencing approach in a small cohort of HCV patients without liver disease.
3,54 In two-thirds of the group (4/6), HCV was detected in CSF. In half (2/4), different viral quasispecies were identified in CSF and plasma, further supporting the presence of independent viral evolution in some patients. Multiple authors have noted that the growing evidence of HCV neuroinfection in some patients brings the long-term efficacy of current therapies into question.
The precise method of HCV entry into the brain is speculative. Brain microvascular endothelial cells, a major component of the blood brain barrier (BBB), have been shown to express all receptors required for HCV internalization whereas other brain-derived cell lines (e.g., microglia, glioblastoma) did not.
17,55,56 In vitro studies indicate that HCV infects brain microvascular endothelial cells that release the virus at low levels and also undergo apoptosis.
55 If these processes occur in vivo, they would provide mechanisms (e.g., reservoir of infectious virus, altered BBB permeability) by which HCV could directly affect the brain.
20,22,55 It has also been proposed that HCV may enter through a Trojan horse mechanism, similar to what is hypothesized for human immunodeficiency virus, as infected PBMCs can cross the BBB and serve as precursors of microglial cells.
20,22,55 Increased viral load in the periphery might facilitate infiltration of the brain by this mechanism.
54Treatments for HCV are now very effective, with SVR increasingly likely with newer direct-acting antiviral agents.
14 However, it is unclear if SVR equates to complete eradication of the virus. In addition, it is likely that antiviral therapies for HCV have limited ability to cross the BBB.
14,54 Reactivation of HCV has been found to occur, especially in immunocompromised patients.
57,58 It is possible that HCV-infected brain microvascular endothelial cells and/or glial cells may provide a reservoir for the virus to persist during antiviral treatment.
22,55 Late relapses (up to 5 years after achieving SVR) following antiviral treatment might be explained by the slower replication rate of HCV in the brain.
59 Studies assessing longer-term SVR with new therapies will be needed.
In conclusion, neuroimaging studies of subjects with HCV has contributed to the understanding of this complex viral infection. Early evidence indicates that in some patients HCV can pass through the BBB, that several cell types may serve as a viral reservoir, and that the virus can evolve independently necessitating further research to answer key questions. These include: What proportion of HCV-infected patients will have brain involvement; how extensive is this involvement; do the antivirals clear the brain of the virus; and are there lasting neuropsychiatric impairments following clearance of the virus?