Decades of research have established that the public holds negative beliefs about persons with mental illnesses, among them that such individuals are dangerous, unpredictable, unattractive, and unworthy and are unlikely to be productive members of their communities (
1–
6). Moreover, these negative perceptions have been remarkably constant despite advances in scientific understanding of mental illnesses and extensive efforts to improve public understanding (
7,
8).
It is unlikely that these negative attitudes and misperceptions emerge full blown in adulthood. Rather, they likely have their roots in childhood and develop gradually through childhood and adolescence. Psychiatrically labeled children, then, may face misunderstandings and negative attitudes by their peers. Ostracism, rejection, teasing, and damage to self-esteem, as well as reluctance to seek or accept mental health treatment, are among the possible consequences (
9–
12).
These consequences may be particularly relevant during adolescence and preadolescence, a period in which onset of a variety of psychiatric disorders peaks and children are acutely attuned to the judgments of their peers. Accordingly, it is important to understand more about the knowledge and attitudes of youths related to mental illnesses and peers who may manifest such illnesses. However, in the United States, attitudes toward mental illness among youths have not received as much research attention as attitudes among adults.
Wahl (
13) reviewed 13 studies completed between 1980 and 1995 in which investigators attempted to assess children's knowledge and attitudes toward mental illness. These studies involved different methodologies and age groups but, overall, seemed to indicate that even young children view mental illnesses as somehow less desirable than other kinds of health conditions. Since Wahl's review, additional studies have emerged. Most of these studies, however, involved students outside the United States (
14–
17), and it is unclear how applicable their results may be to youths in the United States.
The authors located only two previous studies of U.S. adolescents' attitudes toward mental illness. Corrigan and others (
18) found that adolescents described in vignettes as having alcohol abuse problems or mental illness were judged by their peers as more dangerous than those with general medical illnesses. Their peers also feared the vignette characters more and expressed a stronger wish to avoid them. Such results support the concern that stigmatizing attitudes occur among youths. The study, however, did not identify specific knowledge or misunderstandings that might underlie the attitudes expressed nor did it provide information about specific content of stigmatizing responses.
Watson and others (
19) assessed knowledge and attitudes of middle school students as part of an evaluation of a specific curriculum called “Science of Mental Illness.” They reported that students demonstrated some understanding of causes of mental illness but lacked knowledge about treatment and other specific aspects of mental illness.
The studies described above, however, are too small in number to establish understanding of the mental health knowledge and attitudes of U.S. adolescents and to provide more than limited information about the youngsters' specific ideas. Thus, there remains a need for additional research concerning the attitudes and beliefs of youths about mental illness. One aspect of this need is a lack of instruments specifically designed to measure youths' attitudes (
20). Despite the importance of adolescence in the development of attitudes toward mental illness, measures of this group have been slow to emerge. This study, completed as part of a larger study of the effectiveness of a mental health education program (
21), is intended to help fill the gap in knowledge about beliefs among middle school students about mental illness as well as to meet the need for instruments designed for the assessment of mental health knowledge and attitudes of this group.
Methods
Seventh- and eighth-grade students in science or health and physical education classes at four middle schools in different parts of the United States were surveyed between November 2008 and April 2009 about their knowledge of and attitudes toward mental illness. The schools, located in South Carolina, New York, Florida, and New Mexico, had agreed to participate in the larger evaluation study.
The survey consisted of three measures constructed to assess the knowledge and attitudes of students toward mental illnesses and were developed with special attention given to their utility for middle school students. The measures were developed by using items from previous studies of adults' attitudes and feedback from an advisory board of teachers and researchers; a pilot study was used to test and refine items. The knowledge measure consisted of 17 factual statements about mental illness rated on a 5-point Likert scale, from strongly disagree to strongly agree. The attitude measure consisted of 17 opinion statements rated on the same 5-point Likert scale. The items for knowledge and attitudes were randomly interspersed in a single questionnaire for ease of completion. In addition, reverse items were included in each scale such that correct knowledge or positive attitudes would be reflected by disagreement with the statement.
The third major instrument was a social distance scale in which respondents indicated their degree of willingness to interact with a person with a mental illness in specific social situations. Items were modified from standard social distance measures (
20) to better fit the lives of middle school students. For example, instead of being asked about willingness to work with someone with a mental illness at one's job, students were asked about willingness to work together on a class project. The eight items were rated on a 5-point Likert scale, from definitely unwilling to definitely willing.
To determine test-retest reliability of our measures, 87 students from the sample completed the instruments on two occasions approximately one week apart. Test-retest correlations for overall scores for knowledge, attitude, and social distance were .49, .74, and .89, respectively. Analyses of internal consistency, completed during the pilot study, for knowledge, attitudes, and social distance yielded Cronbach's alphas of .63, .83, and .91, respectively.
The research was reviewed and approved by the Human Subjects Research Committee of the University of Hartford. A written description of the research was presented to both parents and students before the students' participation, and both parental consent and student assent were obtained for all participants.
Results
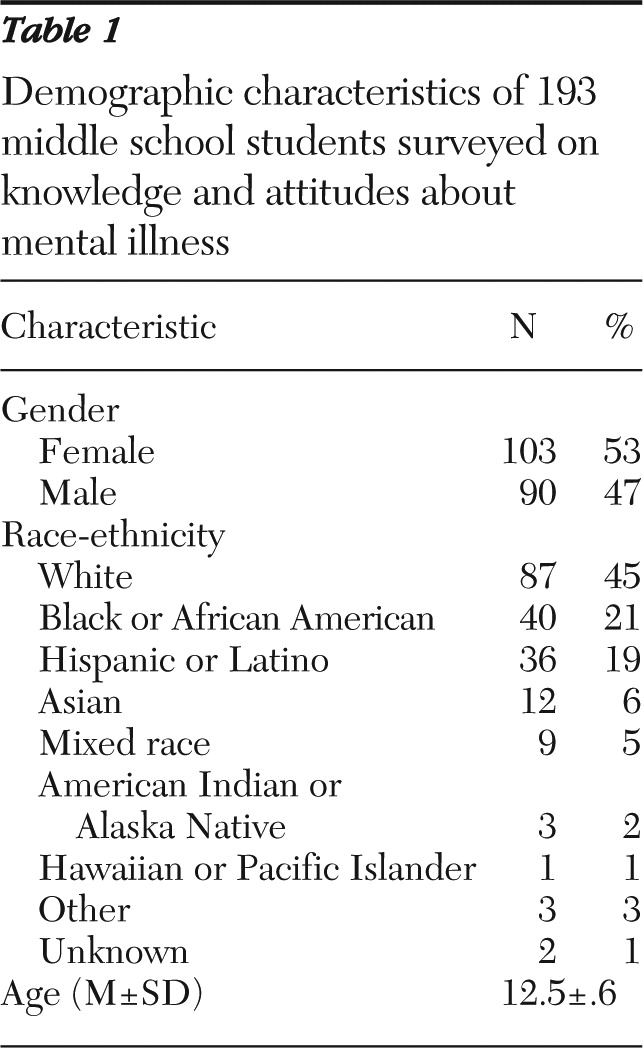
Surveys were completed by 193 students. As shown in
Table 1, the sample included approximately equal numbers of boys and girls and was characterized by substantial racial and ethnic diversity. Analyses comparing study results across schools, genders, and racial or ethnic backgrounds revealed no consistent differences.
For simplification of results, we combined categories of response. The percentage of respondents reported as expressing agreement includes both “agree” and “strongly agree” responses, and the percentage reported as expressing disagreement includes both “disagree” and “strongly disagree” responses. For social distance, willingness includes the responses “definitely willing” and “probably willing,” and unwillingness includes the responses “definitely unwilling” and “probably unwilling.”
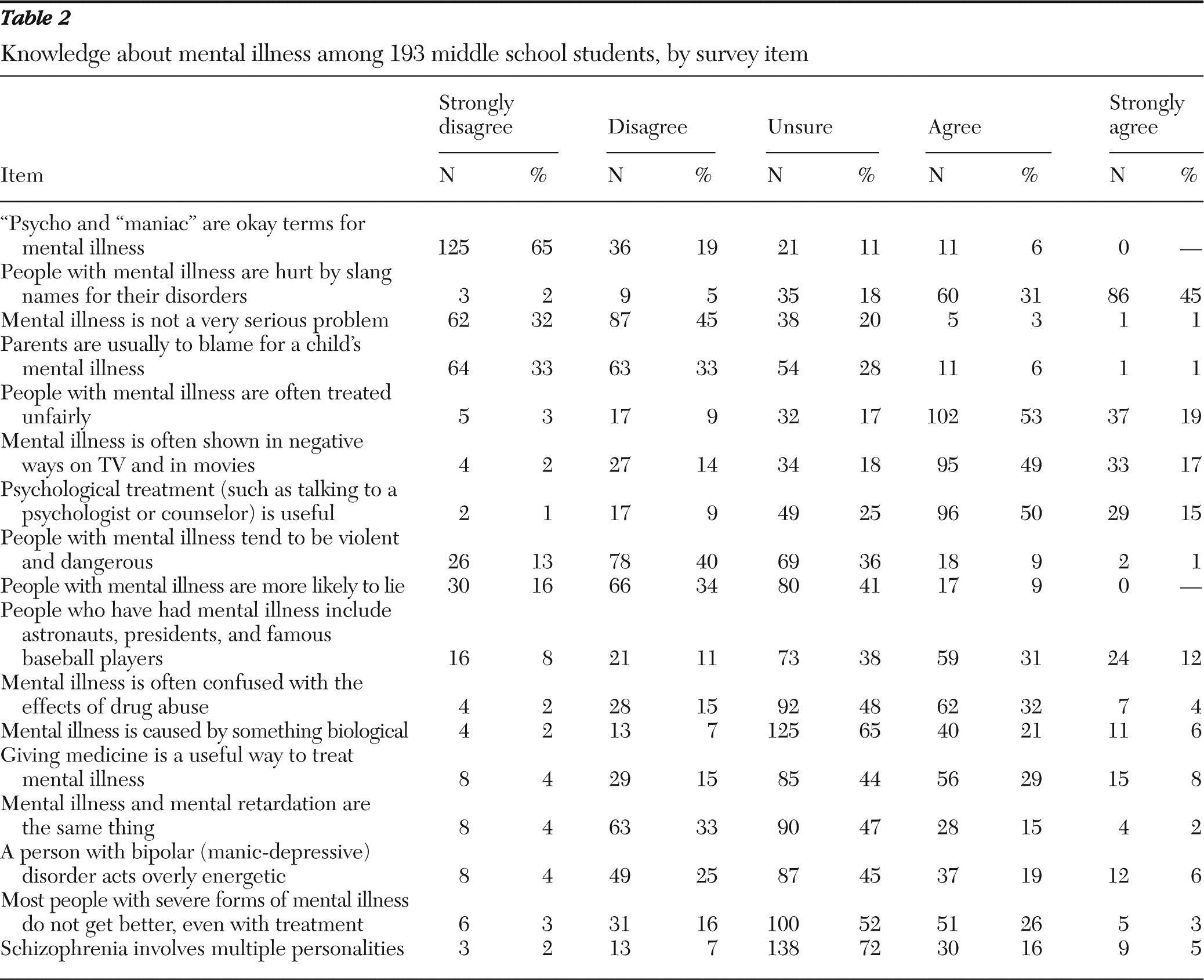
As shown in
Table 2, most students recognized that mental illnesses are often viewed and depicted unfavorably. For example, 72% agreed that people with a mental illness are often treated unfairly, and 66% agreed that mental illness is often shown in negative ways by the media. A majority of students also rejected some of the common inaccurate stereotypes about mental illness. Less than 10% of the students indicated that parents are usually to blame for mental illness, and only 10% agreed that those with mental illness tend to be violent and dangerous.
At the same time, the results indicated lack of knowledge about the symptoms of specific psychiatric disorders. Only one in four students (25%) knew that overly energetic behavior is a symptom of bipolar disorder. Similarly, only 9% of the students were sure that schizophrenia does not involve multiple personalities, compared with 21% of students who believed that schizophrenia does involve multiple personality disorder. Almost three-quarters (72%) of the students were uncertain about whether multiple personalities are part of schizophrenia. In addition, almost half (47%) the students were uncertain about whether mental illness and mental retardation are the same.
Another gap in knowledge involved biological causes and treatment. Most students (65%) were uncertain whether mental illness is caused by something biological, and less than half (37%) believed that medicine is useful in treating mental illness. In addition, nearly one-third (29%) of the students agreed that most people with severe forms of mental illness do not get better, even with treatment, and a majority (52%) were uncertain whether that was true.
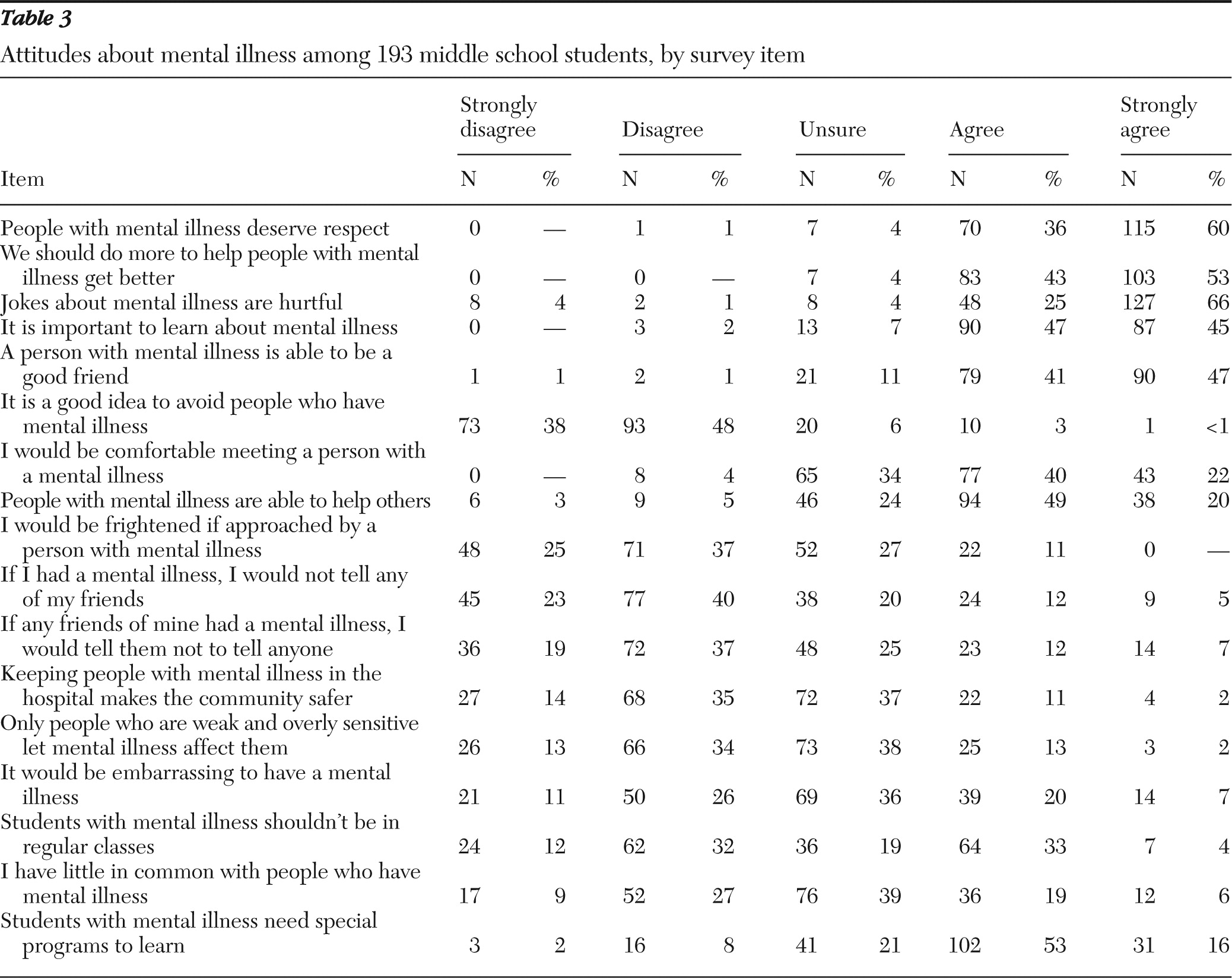
Responses to attitude items are summarized in
Table 3. The results revealed high agreement on many items indicating positive attitudes toward mental illness. Over 90% of students agreed that people with mental illness deserve respect, that more should be done to help people with a mental illness get better, and that jokes about mental illness are hurtful. The students also expressed strong acceptance of people with mental illness. A majority (62%) indicated that they would be comfortable meeting a person with a mental illness, and 62% denied that they would be frightened if approached by someone with a mental illness. Most (86%) also rejected the notion that it is a good idea to avoid people who have mental illness.
Positive attitudes were apparent also in relation to personal responses to mental illness. Most students (56%) rejected the idea of advising friends to avoid admitting to having a mental illness. Most (63%) also disagreed with the idea of not telling friends about their own mental illness. In addition, only a minority (25%) of students saw themselves as having little in common with a person with mental illness, and only 27% agreed that they were likely to feel embarrassed about having a mental illness.
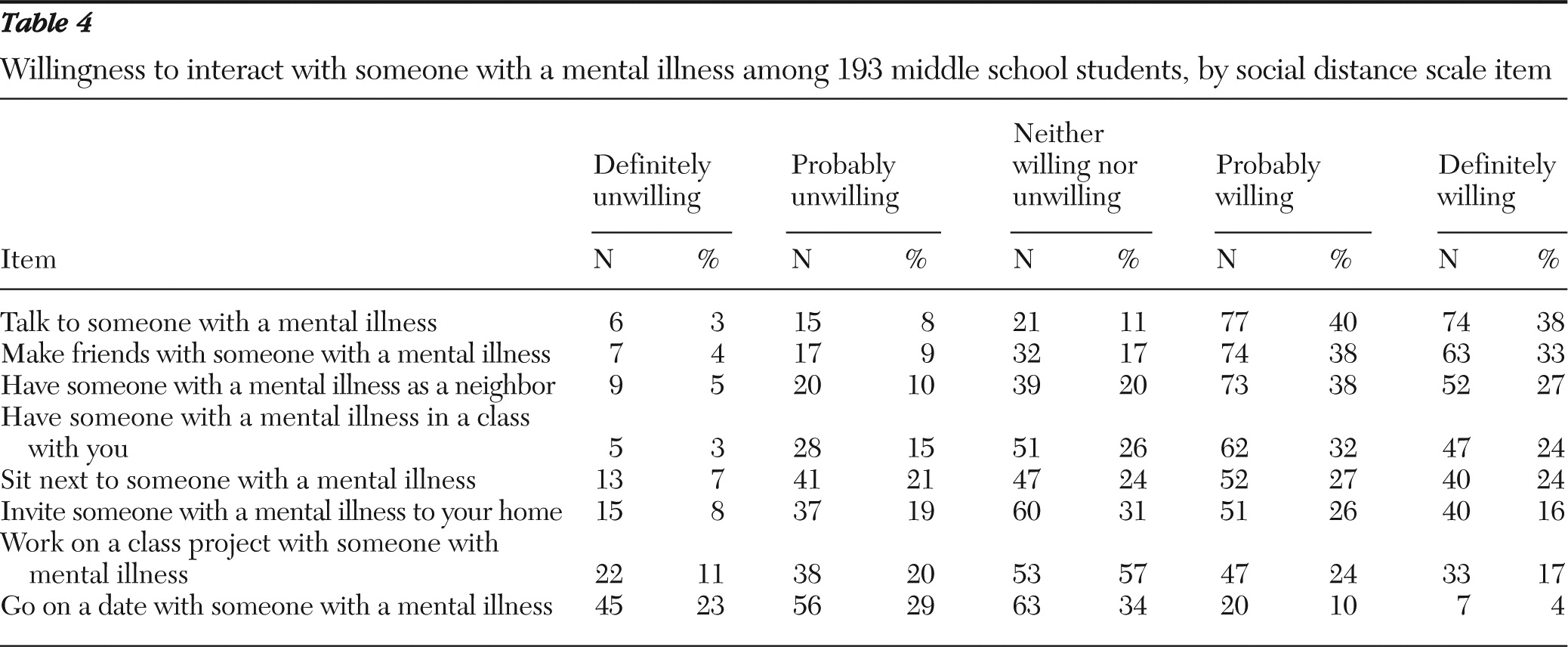
Table 4 summarizes responses to social distance items. Results indicated that most students (78%) expressed a willingness to talk to people with a mental illness, and 71% expressed a willingness to make friends with them. A majority of students also indicated a willingness to have someone with a mental illness as a neighbor (65%) or as a classmate (56%), and half (51%) indicated a willingness to sit next to someone with a mental illness. On the other hand, less than half the students indicated a willingness to invite someone with a mental illness to their home (42%) or to work on a class project with someone with a mental illness (41%). A majority of students (52%) were unwilling to go on a date with someone with a mental illness; only 14% expressed willingness to date someone with a mental illness.
Discussion
The results suggest that middle school students' knowledge of mental illness is inconsistent. They seemed well-informed about some things, such as the unfavorable treatment and depiction of people with mental illnesses. Their knowledge seemed lacking in other areas, and the greatest gaps in knowledge involved the symptoms of specific mental disorders. The common misconception that schizophrenia involves multiple personalities was apparent among student participants, given that only 9% disagreed with that idea.
Similarly, a majority of students did not know that overly energetic behavior is a characteristic of bipolar disorder or that mental illness and mental retardation are not the same. Such results suggest a strong need for better education of students about specific disorders to enable them to recognize, understand, and respond to their own mental illnesses or those of others.
The students' responses to knowledge items also included some unexpected results. One surprising result involved the biological aspects of mental illness and its treatments. Given the increasing trend of conceptualizing mental illness as having biological roots and the pervasiveness of pharmaceutical advertising for an increasing variety of psychiatric conditions, we expected that the students would view mental illness primarily as a biological condition and identify drugs as a main treatment. Certainly, research shows strong endorsement among adults of biological causation and medical treatments of mental illness and indications that such views have become even stronger over the past decade or so (
8). However, most students (65%) expressed uncertainty about whether mental illness had a biological cause and less than half (37%) agreed that medicine is useful in the treatment of mental illness.
Those who believe that it is important to understand the biological underpinnings of psychiatric disorder may be disappointed by the students' substantial uncertainty or lack of knowledge about the biological causes of mental illness and the usefulness of medication as treatment. On the other hand, those who believe that the promotion of biological explanations of mental illness and the increasing reliance on pharmaceutical intervention have had adverse effects may be pleased that students have not fully accepted the biological view of mental illness.
Another surprising result involved fears of violence. A major component of adult views of mental illness is the inaccurate belief that those with psychiatric disorders tend to be violent and dangerous. Our expectation was that this belief would be shared by students as well. However, only about one in ten middle school youths agreed that people with a mental illness tend to be violent and dangerous, and a far greater percentage (53%) disagreed. The responses to specific items in the survey of attitudes, moreover, were consistent with those beliefs. Most students said they would not be frightened if approached by someone with a mental illness, disagreed that people with a mental illness should be avoided, and indicated that they would be comfortable meeting someone with a mental illness. Such results suggest the possibility that the youths of today have not picked up the same fears of mental illness that persist among adult populations.
Finally, with respect to knowledge of mental illness, it appears that the youths were pessimistic about the potential for recovery of people with severe mental illnesses. More than half the students were uncertain whether such individuals would get better, even with treatment, and almost one in three thought such individuals would not benefit from treatment. The more optimistic expectations of the recovery movement have apparently not been incorporated into the understanding of youths, raising the concern that the unwarranted pessimism about the treatment and recovery of persons with severe mental illness of earlier generations continues to be felt.
As noted, students' attitudes overall were quite positive, given that a majority of students expressed accepting, respectful, and sympathetic views toward people with psychiatric disorders. These results are a hopeful sign that the next generation may be developing more favorable attitudes toward mental illness than those of older generations. However, the sizable minorities that indicated negative attitudes toward persons with a mental illness are nevertheless potentially problematic. About one in six (15%) students agreed that only individuals who are weak and overly sensitive let themselves be affected by mental illness. One in four (25%) saw themselves as having little in common with a person with mental illness and about the same percentage (27%) indicated that they would find it embarrassing to have a mental illness. In addition, many students expressed uncertainty about these items. These numbers suggest an environment that includes a substantial undercurrent of negative views about mental illness despite the presence of many positive attitudes.
Social distance results revealed a similar pattern of positive attitudes by a majority of respondents and less accepting views by large minorities. For example, almost one-third (31%) of the students indicated unwillingness to work on a class project with a classmate with a mental illness, and only 41% expressed a clear willingness to do so. The results also mirrored a frequent finding by studies that measure social distance—the more intimate the relationship, the less willing is an individual to interact with someone with a mental illness. Although 78% of students were willing to talk to someone with a mental illness, only 51% were willing to sit next to such a person, and a mere 14% would consider dating that person. Such results suggest that a student with mental illness still will experience substantial rejection and exclusion by his or her peers.
This research, of course, is not without limitations. First and foremost is the potential for socially desirable responding. Student participants may have expressed attitudes that were more positive than their actual views to appear more accepting or to please the researchers. It is also possible that the sample, despite its relative diversity, was not fully representative of the national population of middle school students. For example, the schools that agreed to participate in our research may have had a greater interest in or more accepting ideas about mental illness than schools that did not participate. Similarly, the families and students who agreed to participate in this study about mental illness may have had more favorable attitudes than those who declined. Finally, both the test-retest reliability and internal consistency of the survey of knowledge were somewhat low, raising the question of the scale's overall validity. However, it is not altogether surprising that the students' responses to factual statements were less consistent across administrations. The lower test-retest reliability may represent a meaningful finding that reflects more about the students' uncertainty about the material than about the validity of the instrument. Similarly, the lower internal consistency result may reflect inconsistent gaps in knowledge rather than inadequacy of the measure.
Conclusions
This study provides one of the few systematic empirical assessments of youths' knowledge and attitudes about mental illness, and its results expand considerably what is known about the views of youths. It also introduces a carefully constructed set of measures adapted to the level of its juvenile respondents. Results suggest three main conclusions. First, there are clear gaps in adolescents' knowledge about mental illness, particularly with respect to the symptoms of specific disorders. Middle school students do not appear to have a good understanding of the signs of specific disorders, including disorders that are common among their peers. They may, then, be slow to recognize illnesses experienced by themselves or by their peers, leading to delays in help seeking. It is also possible that students will be confused by or misunderstand psychiatric labels that may be used to describe themselves or others.
Second, attitudes expressed toward and social acceptance of peers with a mental illness among these students were generally positive, but, nevertheless, a substantial proportion of young people held negative views about and were reluctant to interact with peers with a mental illness. At an age when peer approval and inclusion are especially important and when many serious mental health problems emerge, a student experiencing such problems will not be well served by encounters with classmates with negative and rejecting views. In addition, students with negative attitudes may themselves experience mental health problems and experience an exacerbation of disability through self-stigma. Clearly, better education of youths about mental illness and its varied forms and inculcation of more positive and accepting attitudes are needed.
Acknowledgments and disclosures
This research was supported by grants R01MH076093 and R01MH075837 from the National Institute of Mental Health (NIMH). The National Alliance on Mental Illness (NAMI) Queens/Nassau receives funds from a wide variety of sources, including donations by pharmaceutical companies to the NAMIWalks campaign. Funds raised through the walk are used for general operating expenses and for support and education for those living with mental illness and their families as well as for the Breaking the Silence school education program. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIMH or of the National Institutes of Health.
The authors report no competing interests.