Site Demographic Characteristics and Prior Community Education Experience
By design, there was significant variation across sites in geography, demographic characteristics of the population served, agency affiliation, and prior outreach. Defined catchment areas ranged from 4,839 square miles in Oregon to 82 square miles in New York, encompassing a total population of 2,985,384 across all sites, about 1% of the U.S. population according to 2010 census data (see online supplement). Four sites had prior experience with community education, mostly regarding optimal treatment of first-episode psychosis.
PIER, based at Maine Medical Center, Portland, began providing outreach to the community in 2000 and continued outreach during EDIPPP, focusing on youths at high risk of psychosis. Its catchment area had a relatively homogeneous population of 323,105, with recent immigrants adding some cultural diversity. PIER’s connections in the community, established through ongoing and organized outreach to schools, medical practices, and community agencies, were an asset when EDIPPP was implemented in the Portland area.
EAST was a division of Mid-Valley Behavioral Care Network in Oregon, a five-county intergovernmental managed mental health organization in northwestern Oregon; the catchment area population was 631,853. For seven years prior to EDIPPP, EAST conducted extensive community outreach within this system for a first-episode program. With EDIPPP, EAST expanded its outreach to schools and medical practices, updating referrers on clinical high-risk criteria.
M3P, operated by Washtenaw Community Health Organization in Michigan, provides integrated health care for people with mental illness, developmental disabilities, and substance use disorders. With a population of 344,791, Washtenaw County covers nearly 800 square miles. When EDIPPP was implemented, M3P was newer to community outreach but found that its outreach and community education was welcomed in schools and medical facilities. At the time of EDIPPP implementation, M3P had no prior experience with high-risk youths.
Since 1998, RAP has been an early intervention and prevention research program at Zucker Hillside Hospital. RAP’s catchment area included areas in Nassau and Queens Counties, with an ethnically diverse population of 557,725. When EDIPPP was implemented, its hospital system had provided most of the referrals needed to sustain its research program; systematic and targeted outreach was initiated in 2007.
EDAPT, a division of the University of California, Davis (UCD), had the city of Sacramento as its catchment area, with a highly diverse population of 466,488, and 27% with Latino ethnicity. When EDIPPP was implemented, EDAPT’s prior community outreach for research purposes was helpful, but it included only inpatient and outpatient mental health facilities. With the start of EDIPPP, UCD conducted more systematic outreach to schools, primary care physicians, and community agencies. Previous affiliation with the city’s school district contributed to outreach to schools.
EARLY is located in Albuquerque’s largest metropolitan area. The catchment area’s population of 661,422 is ethnically diverse, with 48% identifying as Latino. EARLY is based at the Department of Psychiatry’s Center for Rural and Community Behavioral Health at the University of New Mexico. When EDIPPP was implemented, its previous community partnerships enabled it to rapidly launch outreach efforts.
Outreach Successes and Challenges
Each site offered qualitative feedback about its unique experience with the outreach protocol. EAST’s steering council was able to access a wide network of professionals and opportunities for partnering at events where other programs in the area were offering community education. PIER’s steering council was crucial in helping to map community audience groups and in connecting with “gatekeepers” for intended audiences, especially among recent immigrants. EDAPT’s steering council provided invaluable guidance on how best to approach some of the cultural communities, such as the Hmong. The EARLY program did not ask its steering council to play a more active role in setting up outreach presentations, although program outreach was successful through some of the university’s community affiliations.
In New York, the population density is so high that only a few specific and noncontiguous zip codes were included in the catchment area of RAP. As a result of this design, compared with other locations, the New York site had a high volume of telephone referrals from out of its catchment area (
24). The EARLY program in New Mexico found that although presenting to districtwide groups was efficient, it was also problematic because the zip codes of some attendees were not in the eligible catchment area. Because of the size of its treatment team, EARLY’s enrollment was staggered by area zip codes to eventually include the entire county. Sites that included the entire county (New Mexico, Michigan, and Oregon) had fewer concerns about the catchment restrictions.
EDAPT’s initial contact with administrators in the Sacramento City Unified School District led to districtwide outreach activities, which had the greatest impact on EDAPT’s referral base. As a result of M3P’s outreach in schools, some of the schools and colleges developed their own mental health awareness campaigns. PIER’s greatest area of success was in developing a system of regular training sessions in all Portland-area high schools and colleges. PIER’s outreach broadened within the school system after a tenth-grade health class curriculum and a college resident advisor training were developed. EARLY’s initial outreach priority was schools. Within the first few months, the program had presented to all of the nurses, social workers, school counselors, and psychologists in the Albuquerque public schools. Because EARLY is a division of the University of New Mexico, it met with student counseling personnel, campus police, and residence hall directors. RAP faced unique challenges in school outreach because the New York City Board of Education has restrictive rules about the involvement of outside agencies and research projects. Thus conducting outreach events at area schools was difficult, but RAP made use of professional networks through mailings and calls that led to successful school outreach events. However, RAP’s inability to do wider school outreach was reflected in a lower rate of school referrals.
M3P, like EAST, was embedded in the community mental health system, providing a natural referral source. EARLY had fewer referrals from mental health professionals, because the program focused more of its energy on schools.
Private-practice professionals were more difficult to reach without a specific group to which presentations could be made. One successful approach was to offer large-scale training sessions and to provide continuing education credits. Overall, mental health professionals generated the highest number of referrals across sites and were more likely to make appropriate referrals (
24).
Although gaining access to primary care providers was a critical part of the strategy, it was a challenge for all sites because of skepticism about the prevalence of psychotic illnesses and limited time available to focus on mental health issues. Hospital affiliations (RAP and PIER) did not facilitate access to primary care providers. PIER found that the most successful approaches included a “lunch and learn” to accommodate physicians’ schedules, grand rounds presentations, and outreach to participants’ medical providers. EDAPT clinicians were able to reach family medicine providers and some primary care providers through existing clinical affiliations.
One of the challenges for the sites with large Latino populations was the research restriction that the client and one parent be proficient English speakers. Nevertheless, enrollment of Latino families at most sites was representative of the catchment area: California had 31%, compared with 27% in the catchment area; New Mexico had 45%, compared with 48%; New York had 22%, compared with 20%; and Oregon had 10%, compared with 18% (
Table 1).
Prior to EDIPPP, UCD Medical Center had made efforts to reach underserved cultural communities in Sacramento and had a number of programs that greatly facilitated outreach to immigrant communities. However, the name recognition of UCD may have hindered outreach to some community providers who were not part of the UCD Health System because of an “ivory tower” perception.
New Mexico has a large Latino and Native American population. Some cultures have a different interpretation of the cluster of symptoms that Western medicine considers “psychosis.” For example, during a presentation to behavioral health staff at a Native American charter school, the presenters were interrupted as they listed the signs of psychosis by a staff member who said, “You just described a medicine person in my culture.” The nature of psychosis and how it might be interpreted required cultural sensitivity and a focus on functioning. We presented warning signs in terms of their impact on work and school, such as “difficulty speaking or understanding others” or “trouble with reading comprehension and writing.” The Michigan staff found that at health fairs with diverse audiences, they were asked to talk more broadly about overall mental health and wellness.
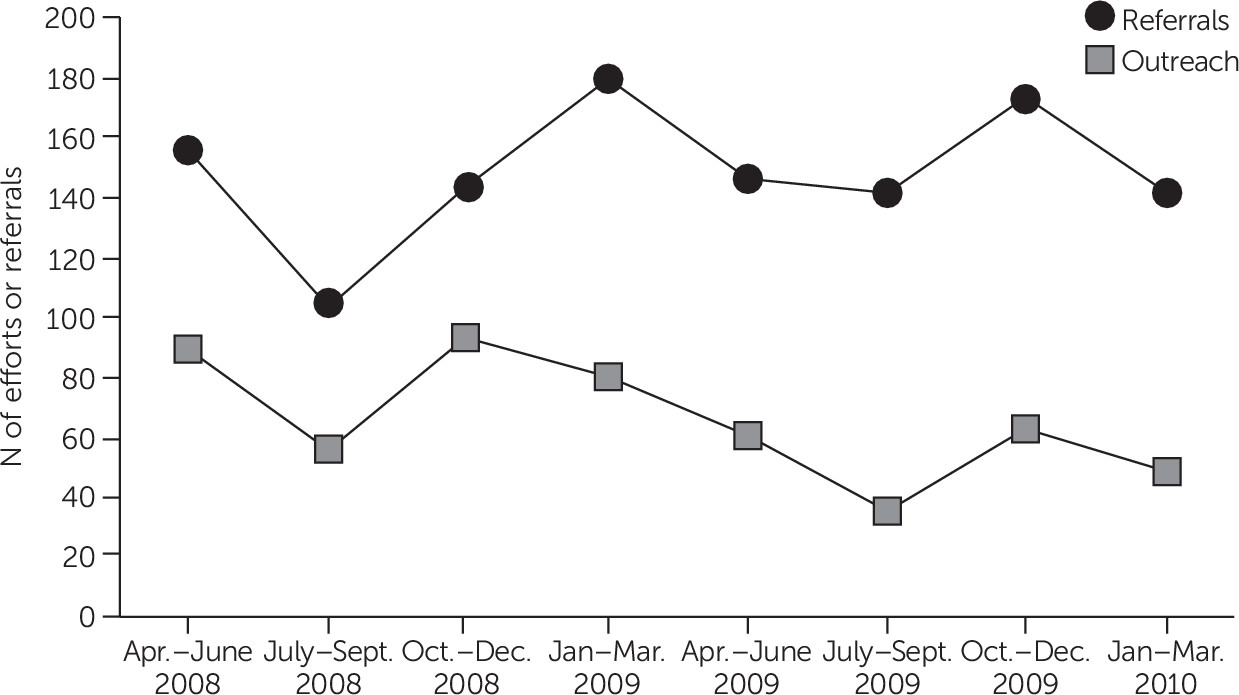
Consistency of outreach effort resulted in more referrals. Providers needed periodic contact from the EDIPPP team to both train new staff and refine skills in identification of early symptoms. Maintaining consistent community education was a challenge at all sites, but setting monthly target goals helped. For instance, EARLY stayed in touch with referrers through a quarterly newsletter, periodic e-mails containing program updates, and media coverage.