The prevalence of mental illness is higher among persons who have committed criminal offenses than in the general population (
1,
2). Offenders with mental illness reoffend at higher rates and more quickly after incarceration than offenders without mental illness (
1,
3–
6). Mental health courts (MHCs) were developed to stem this trend, aiming to reduce the number and limit incarceration time of mentally ill offenders in the criminal justice system (
7–
9).
Although no standardized model exists, many MHCs share several characteristics (
8,
10–
13). MHCs are criminal courts with a specialized court docket for mentally ill offenders, who typically voluntarily consent to enrollment. MHCs require participants to have a mental illness that likely contributed to one or more crimes, and some restrict enrollment to misdemeanor or nonviolent offenses (
11,
14). MHCs rely on a collaborative team of individuals, such as judges and social workers, to facilitate relationships between offenders and community support and to provide additional supervision.
Several studies have reported a trend for MHC participation to have an impact on recidivism outcomes. A recent meta-analysis reported a significant, moderate mean effect size for decreased rates of recidivism among participants in MHCs (
15). MHC participants tend to reoffend less frequently (
16–
23), commit less severe crimes at rearrest (
20), and take longer to reoffend (
20,
23,
24). Although MHC researchers generally report positive findings, the methodology they employ varies greatly, and the quality of the study has an impact on the significance of the results. Meta-analytic data indicate that results for quasi-experimental studies were moderate and significant, whereas the pooled effect for studies comparing the effect of the program on a single group of individuals was nonsignificant (
15). Even with quasi-experimental design, studies of MHCs typically utilize nonequivalent matched control groups (for example, Herinckx and colleagues [
18]). Although random assignment would be ideal—examples include studies by Cosden and colleagues (
16,
25)—many stakeholders resist withholding services from control participants. Only two studies have employed statistical methods designed to control for the problems inherent in nonrandom assignment (
21,
26).
In addition to these concerns, previous studies failed to adequately address potential differences in effectiveness of MHC among classes of offenders. Many MHCs exclude or limit felony and violent offenders (
10). Felony defendants, however, tend to have better recidivism outcomes than misdemeanants in the general population (
27), among mentally ill offenders (
5,
6), and in drug courts (
28). Felony-only (
29) and combined misdemeanor-felony MHCs (
16,
20,
22,
25,
26) have reported favorable recidivism outcomes, and two studies have reported no significant relationship between offense type and either odds of recidivism or number of jail days after exiting an MHC (
22,
24). No similar empirical examination has compared recidivism outcomes of violent and nonviolent offenders, although studies of drug courts offered preliminary support for inclusion of violent offenders in diversion programs (
30). Generally speaking, the conclusions that can be drawn from research on recidivism among MHC participants have been limited by a lack of analyses by subgroup of offense type, given that the “dose” of MHC may differ on the basis of the type of index crime. (For example, the number of status hearings could differ as a function of severity of index offense [
31]).
This study of an MHC in the southeastern United States attempted to expand upon previous findings in three main ways: by employing propensity score matching to control for nonrandom assignment, utilizing a control group of mentally ill offenders in traditional criminal court in the same jurisdiction, and exploring potential differences between felony and misdemeanor participants and violent and nonviolent participants. Outcomes were examined with both between-groups and within-subjects designs. We predicted that at 12-month follow-up, MHC defendants would have significantly lower rates of recidivism; if arrested again, would be charged with a less severe crime; and would have increased time to rearrest. We also predicted similar findings for subgroups of felony, misdemeanor, violent, and nonviolent offenders. In addition, we predicted MHC defendants would exhibit significantly lower rates of recidivism, subsequent arrests for less severe crimes, and increased time to rearrest during the 12 months after enrollment than during the 12 months before enrollment. Finally, we predicted recidivism outcomes for MHC defendants charged with a felony would be superior to those of MHC defendants charged with a misdemeanor, and violent MHC defendants would have superior recidivism outcomes than nonviolent MHC defendants.
Methods
Participants
Inclusion criteria for both the MHC group and the traditional-court control group were presence of a new charge in the years 2008–2010, index offense or reoffense other than a technical violation, and complete data for all demographic, diagnostic, and clinical variables used to generate propensity scores. Of the 824 MHC participants, 450 met inclusion criteria for this study. Included and excluded MHC participants significantly differed by gender (males, N=329, 73%, and N=243, 65%, respectively; χ
2=7.75, df=1, p<.05). Of the 522 mentally ill offenders assigned to traditional criminal court, 227 were included in this study. Included and excluded traditional-court offenders significantly differed by diagnosis of a bipolar disorder (N=9, 4%, and N=47, 16%, respectively; χ
2=21.47, df=1, p<.001). [A detailed description of the study setting and group assignment procedures is available online as a
data supplement to this article.]
Florida State University’s Institutional Review Board approved the study, and the court also consented to data collection. This study was part of a larger data collection evaluating the MHC. Because data were retrieved from public records, informed consent was not required.
Measures
Access to the Jail Information System (JIS) and the Management Information System (MIS) was granted by the MHC's Board of County Commissioners. The JIS contains data for MHC and traditional court collected by the MIS. This database contains demographic, criminal, and diagnostic information for every defendant in the county of the MHC. These databases contain only information about arrests made in Florida. All data used in the analyses were retrieved from JIS and MIS or created by using data from those systems.
Index offense variables.
The index offense for the MHC group was the arrest resulting in a new charge that qualified the individual for participation in MHC. For the control group, the index offense was the first new charge that occurred during the same time period (2008–2010). The following index offense variables were used: severity of offense, categorization as misdemeanor or felony (0 or 1), and categorization as nonviolent or violent (0 or 1). Severity of offense was determined by a scale from 1 to 13, with 1 indicating noncriminal violations; 2, second-degree misdemeanors; 3, first-degree misdemeanors, and 4–13, felony offenses. Classification of felony offenses was based on the felony sentencing guidelines of the State of Florida (
32). If an index arrest involved two or more charges, the most severe charge was used for analyses. Following McNiel and Binder (
26), a violent offense was defined as harm or threat to a person; all others offenses were considered nonviolent.
Independent variable.
A dichotomous variable indicated assignment to traditional criminal court or MHC (0 or 1).
Dependent variables.
Data were collected for the following outcome variables during the 12 months after the index offense: any arrest resulting in a new charge (rearrest), sum of rearrests, number of months between index offense and rearrest, and severity of charge at first rearrest. In cases of two or more charges at rearrest, the most severe was used for analyses. Rearrest severity was coded by using the scale described above.
Pre-MHC variables.
Data for the 12 months before the index offense were obtained for MHC participants. The following variables were used: total number of arrests, type and severity of offense closest in time to the index offense, classification of offense closest in time to index offense as misdemeanor or felony and as nonviolent or violent, and number of months between the offense closest in time to the index offense and the index offense. Classification of severity and type of offense was defined and coded by using the procedures described above.
Control variables.
Along with index offense variables, the following covariates were used in the between-group analyses: diagnosis of mental illness, homelessness, and demographic information. Age at index offense was calculated by using date of birth and date of index offense. Two individuals were identified as Asian/Pacific Islander and were combined with African-American individuals to create a dichotomous race variable (white or nonwhite).
Data analysis
An intent-to-treat approach was utilized for all analyses.
Between-group analyses.
Analyses were conducted to compare recidivism between MHC and control group participants for the full sample and for each offense subgroup. Univariate comparisons were conducted for continuous (t tests) and categorical (chi square tests) recidivism variables. Multivariate techniques allowing for the consideration of the covariates’ impact on the relationships of interest were employed. Logistic regression analyses tested the hypotheses that court membership predicted rearrest in the 12 months after the index offense. Cox proportional hazards models tested the effect of court assignment on time to rearrest. Proportional hazards models assess group differences in survival time and consider time to failure (rearrest) in estimating the coefficients while controlling for the effects of covariates. In this study, individuals who had not reoffended by the end of the 12-month period were censored at month 12. For ease of interpretation, odds ratios [ORs] less than 1.00 were converted to ORs greater than 1.00. If univariate comparisons indicated that severity of rearrest was associated with group assignment, we were prepared to conduct multiple regression analyses to determine the impact of MHC enrollment on rearrest severity.
Within-subjects analyses.
Changes in outcomes in the MHC sample before and after enrollment in MHC were explored by using paired t tests. In addition, the bivariate and multivariate analyses described above were repeated to compare results for the MHC sample before and after participation. In these analyses, classification of index offense as felony or misdemeanor or as violent or nonviolent served as the independent variables.
Results
Propensity score matching
Propensity score matching was utilized to control for nonrandom assignment, resulting in a data set of 396 offenders (N=198 in each group) (
33,
34). [Detailed information on this procedure as well as overall data issues is available in the
data supplement.] No significant differences were found between the two groups for the 32 variables assessed (
Table 1). After the matching procedure was completed, tests of the proportionality of hazards assumption and multicollinearity were conducted, and the values were within acceptable levels (
35).
Between-group analyses
Full sample.
The MHC group had superior recidivism outcomes relative to the control group on nearly all observed outcome variables (
Table 2). The MHC group had a significantly lower occurrence of rearrest (χ
2=20.89, df=1, p<.001, φ=–.23), took longer to reoffend (t=–4.66, df=394, p<.001, d=–.47), and accrued a significantly lower number of rearrests (t=4.70, df=393, p<.001, d=.47). Severity of the rearrest offense did not significantly differ between the groups; therefore, multivariate analyses involving rearrest severity were not conducted.
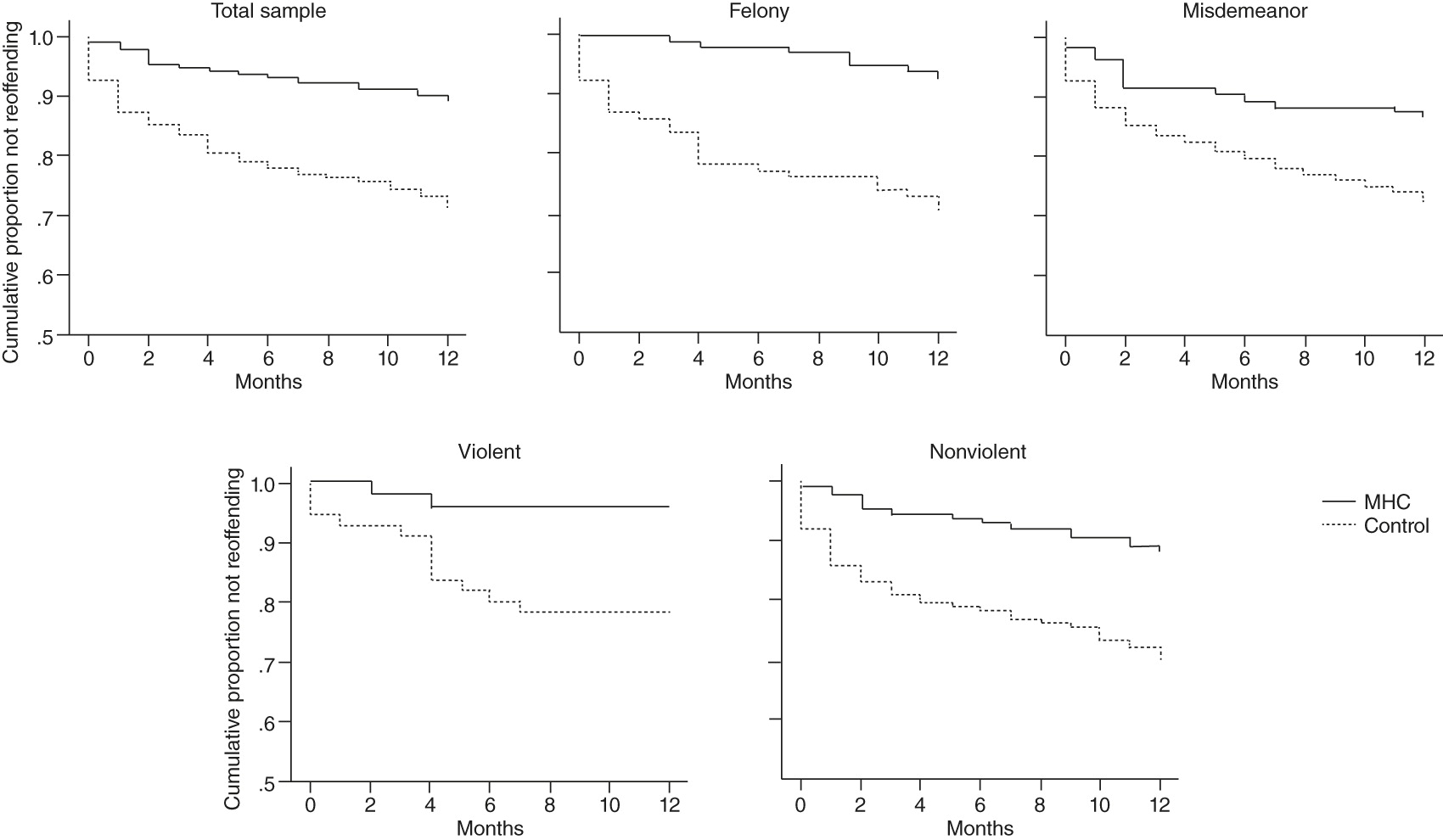
To assess the extent to which assignment to MHC predicted rearrest and time to rearrest, logistic and Cox regressions were conducted (
Tables 3 and
4,
Figure 1). The addition of court membership in the second step of the logistic regression contributed significantly to the model (Δχ
2=19.47, df=1, p<.001), and the overall model was significant (χ
2=43.71, df=14, p<.001). Assignment to the traditional criminal court compared with assignment to MHC significantly increased the odds of rearrest by 251% (
β=–1.25, p<.001, exp[
β]=3.51) (
Table 3). Likewise, addition of court assignment significantly contributed to the Cox proportional hazards model (Δχ
2=18.75, df=1, p<.001), and the overall model was significant (χ
2=38.38, df=14, p<.001) (
Table 4). MHC participation compared with assignment to traditional criminal court predicted a longer time to rearrest for the full sample (
β=–1.08, p<.001, exp[
β]=2.94). In addition, being male predicted a shorter time to rearrest for the full sample (
β=.70, p=.021, exp[
β]=2.01).
Subgroup analyses.
The results of subgroup analyses are reported in
Tables 2–
4 and in
Figure 1. For each subgroup, assignment to MHC versus traditional criminal court significantly decreased the odds of rearrest (
Table 3). MHC assignment was also significantly related to longer time to rearrest of participants charged with felony, misdemeanor, and nonviolent offenses. In addition, being male predicted a shorter time to rearrest for participants charged with misdemeanor (
β=1.28, p=.005, exp[
β]=3.61) and nonviolent (
β=.73, p=.026, exp[
β]=2.07) offenses. For violent offenders, the overall Cox regression model was nonsignificant, and the prediction of time to rearrest by MHC participation failed to reach statistical significance. All subgroup analyses involving severity of rearrest offense failed to reach significance.
Within-subjects analyses
Within-subjects analyses were conducted by using the full sample of MHC participants (N=450). [A table presenting the results of the analyses is available in the online
data supplement.] The total number of arrests resulting in a new charge in the 12 months preceding the index offense was significantly higher than the total number of rearrests in the 12 months after the index offense (t=8.77, df=358, p<.001, d=.62). In addition, the number of months between the index arrest and the closest previous arrest was significantly less than the number of months between the index offense and the first rearrest (t=7.47, df=130, p<.001, d=1.02). Contrary to expectation, severity of the offense associated with rearrest was significantly higher than the severity of the offense associated with the arrest prior to the index offense (t=–2.16, df=110, p=.033, d=.25).
Hypotheses predicting greater success for felony offenders relative to misdemeanor offenders and for violent offenders relative to nonviolent offenders within the MHC were largely not supported by the results (data not shown). MHC defendants charged with a misdemeanor had a significantly higher occurrence of rearrest, relative to those charged with a felony (χ2=4.87, df=1, p=.027, φ = –.104); however, defendants charged with misdemeanors and felonies did not differ on odds of rearrest or time to rearrest. Defendants charged with violent and nonviolent offenses did not differ on any recidivism outcomes.
Discussion
This study adds to increasing evidence supporting the effectiveness of MHC in reducing recidivism among offenders with mental illness. Consistent with previous findings (
16,
20,
22,
23,
25,
26), MHC participants demonstrated better recidivism outcomes than a control group of offenders assigned to traditional criminal court as well as improvements in the occurrence of rearrest and time to rearrest before and after their participation. The results build upon previous findings in three important ways: employing propensity score matching to control for nonrandom assignment, utilizing a control group of mentally ill offenders in traditional criminal court in the same jurisdiction, and exploring differences between felony and misdemeanor participants and violent and nonviolent participants.
The inclusion of subgroup analyses is a significant contribution to the literature (
31). Between-group findings remained unchanged across subgroups, with the exception of a nonsignificant finding for the prediction of time to rearrest by violent offense. Furthermore, within the MHC sample, misdemeanor offenders had higher rearrest prevalence than felony offenders but did not significantly differ on time to rearrest or severity of rearrest offense. Violent and nonviolent offenders did not significantly differ on any recidivism outcome. This demonstration of benefit across subgroups of offenders offers preliminary evidence that classification of offense is an inefficient variable for excluding individuals from MHC.
Given the nature of the MHC studied (as described in the online
data supplement), these data, in conjunction with existing literature, suggest that the mere act of keeping mentally ill offenders out of jail may be one primary mechanism by which MHCs affect offending outcomes. The criminology literature has established that, at best, incarceration does not reduce recidivism and, at worst, is iatrogenic (
36,
37). It is not unreasonable, therefore, to posit that placing vulnerable mentally ill offenders in a jail or prison, resulting in poor treatment access and exposure to a potentially dangerous environment, may be acutely harmful. As this study and others show, programs to keep mentally ill offenders in the community seem to have a positive impact on recidivism.
The increased attention and supervision paid to the MHC participants through regular status hearings also bear consideration as an explanation for the effects of MHC participation, but they are likely an associated mechanism rather than a primary mechanism of change. Perhaps the attention and supervision increase accountability and decrease criminal behavior among mentally ill offenders. Frequency of judicial status hearings varies greatly between MHCs. For example, Redlich and colleagues (
38) reported a small, inverse relationship between court appearances and MHC completion, such that having fewer hearings was related to completion. This relationship, however, became nonsignificant after the study controlled for other predictor variables (
38). Notably, whereas many authors have asserted that participant-judge interaction style results in positive MHC outcomes (
39–
45), others have pointed to the importance of the entire MHC team’s knowing the defendant and treating him or her with empathy and respect (
44). Given the limited judge-defendant interaction in the MHC studied (
45), future studies should consider not only frequency of hearings but also team-defendant interactions as well. More globally, future studies should dismantle the components of MHC and experimentally test their importance in order to fully understand the mechanisms of change in MHCs.
Contrary to prediction, comparisons of severity of the rearrest offense between the MHC and the control groups failed to reach significance, and severity of rearrest offense was significantly higher after participation in the MHC. Although examination of this outcome is considered important by many, findings in the literature regarding rearrest severity are limited and equivocal (
20,
46). Utilization of a Florida statute as the basis for severity ranking, a system developed by the legislature, could have influenced the findings of this study.
Although this study had a number of strengths, it should be considered in light of the limitations. Generalizability of findings is concerning for a variety of reasons, including findings of lower rearrest rates than reported by other studies and the use of data from only one jurisdiction. Aggregate observations of multiple courts are necessary to determine the overall effect of MHC independent of the idiosyncrasies of individual courts (
21). Although we believe that the use of a control group in the same jurisdiction strengthened the study, we were unable to determine the reasons that members of the control group did not qualify for MHC.
Another limitation was the lack of random assignment. Although propensity score matching was utilized to reduce risk of selection bias, it remains possible that factors we were unable to control for influenced court assignment. Likewise, data on jail time during the follow-up period were unavailable, and the absence of this information could have had an impact on the results; however, individuals in the control group would be more likely to spend time in jail, causing an overestimation of the control group’s success and an underestimation of the effect of MHC. Finally, one judge presided over each branch of the MHC (felony and misdemeanor); thus, no comparisons could be made across the court’s two judges, given that their cases did not overlap.
Conclusions
These findings add to the evidence that MHC produces favorable recidivism outcomes. The results also indicate that felony and violent offenders can benefit from inclusion in MHCs. Despite lacking some “essential” characteristics of MHC, the MHC studied engendered significant improvements. Such findings highlight a need for more studies investigating the necessity of common MHC characteristics. Future research would benefit from a focus on the mechanisms of change in MHC and on identifying characteristics of individuals who respond best to participation in MHC.
Acknowledgments and disclosures
This study was in part supported by a State of Florida Substance Abuse and Reinvestment Grant (2009–2011). Dr. Anestis completed this research in partial fulfillment of the degree of Doctor of Philosophy at Florida State University and thanks her dissertation committee for their feedback and guidance regarding the manuscript: Chris Schatschneider, Ph.D., Mark Licht, Ph.D., Edward Bernat, Ph.D., and William Bales, Ph.D. She also thanks Amanda Gallagher, M.S., Emily Gottfried, M.S., Haley Gummelt, M.S., and the undergraduate lab members who aided in data collection; Scott Vrieze, Ph.D., and Sylia Wilson, Ph.D., for statistical advice; and Michael Anestis, Ph.D., for his feedback.
The authors report no competing interests.