In the second half of the 19th century there was a rapid expansion of asylums in many of the more economically developed countries (
1,
2), followed by a decline in capacity over the past 50 years (
3). The three components of deinstitutionalization are the prevention of inappropriate admissions to psychiatric hospitals through the provision of community facilities, the release to the community of all institutional patients who have received adequate preparation, and the establishment and maintenance of community support systems for noninstitutionalized patients (
4). More succinctly, deinstitutionalization is the contraction of traditional institutional settings with a concurrent expansion of community-based services (
5).
This policy has now been replicated throughout most of the economically developed world, and evidence on the cost-effectiveness of these far-reaching changes comes from several key studies (
6,
7,
8,
9,
10,
11,
12) and reviews (
7,
13,
5,
8). The most comprehensive assessment was conducted by the Team for the Assessment of Psychiatric Services (TAPS) (
14,
15,
16,
17,
18,
19), which interviewed all long-term inpatients with a length of stay of more than a year at two large psychiatric hospitals in North London (
5). One year after discharge, patients who had left the hospital were reinterviewed and were compared with a control group who had remained in the hospital during the study period. Few differences were found between those who left the hospital and those who did not in terms of individual patients' clinical and social outcomes one year after discharge. The benefits conferred by community placements were more diverse social networks, more autonomy, and a marked preference by patients for community rather than hospital residence (
16). The TAPS findings are also notable for demonstrating that very few of the long-stay patients became homeless after discharge, that it was rare for discharged patients to engage in crime, that the mortality rate did not differ between those who were discharged and those who were not, and that the discharged patients continued to need brief hospital admissions for acute relapses of their psychotic disorders (
17,
18,
19,
20).
The study reported here tested the replicability of these findings in relation to changes in symptoms, social behavior, and social networks and added a focus on the patients' own attitudes and preferences about hospital and community care. The aims of the study were to evaluate the effects on patients of moving from the hospital to community-based settings, to compare these individuals who left the hospital with a control group who stayed on as inpatients, to address the question of whether discharge from the hospital reverses institutionalism, and to evaluate the overall success of hospital closure in the first year after discharge.
The following hypotheses were developed from a review of the relevant literature to establish the success or failure of the deinstitutionalization program. The first hypothesis was that, compared with patients who did not leave the hospital, patients who were discharged would have significantly better mental states, social functioning, and social networks at follow-up. The second hypothesis was that community settings would provide a significantly better environment than the hospital. The third hypothesis was that discharged patients would express a preference for community care after discharge from the hospital.
Discussion and conclusions
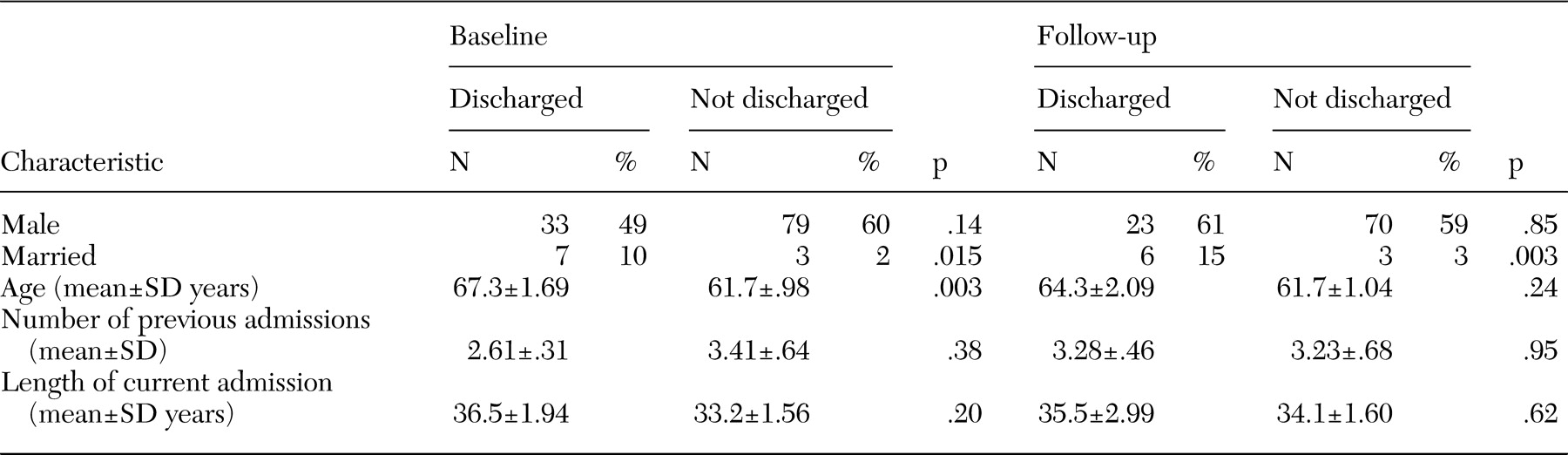
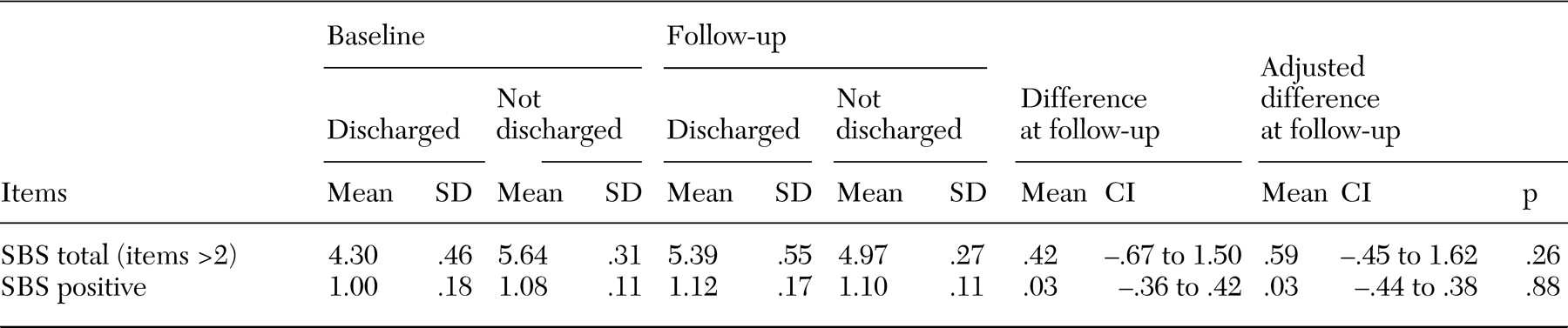
No overall differences were detected in the pattern or severity of symptoms between patients who were discharged from the hospital and those who were not, and nor were any changes over time noted, which is consistent with the results of earlier research (
16). Thus there was no evidence of any amelioration of the features of institutionalism one year after discharge, nor any differences in mortality rates between persons who were discharged and those who were not discharged from long-term hospital care (
20). Therefore our initial optimism (that hospital discharge would be associated with a reduced level of instititutionalism) as well as our concern (that death rates would rise after hospital transfer) were both misplaced, despite very substantial changes to the patients' immediate living environments.
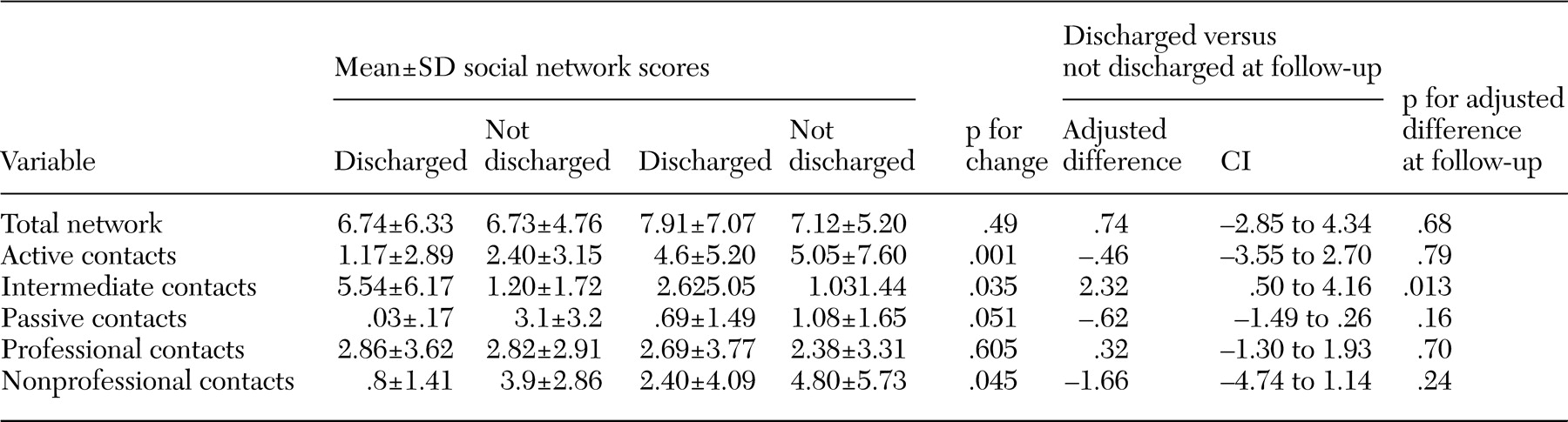
The results pertaining to patients' social networks were more subtle. As expected, after discharge from the hospital, patients kept contact with more staff and patients in the community and with fewer who were based in the hospital. The size of the total social network increased over time both for patients who left the hospital and for those who stayed. At the same time, more contacts were active—that is, involving a two-way exchange—rather than passive. In parallel, the number of friends and confidantes also increased for both groups of patients. The overall trend was for a modest improvement in the quantity and quality of social networks for both the discharged group and those who were not discharged. This finding suggests that the process of deinstitutionalization may confer benefits both on those who leave the hospital and on those who stay in the hospital for rehabilitation before discharge.
Our first hypothesis—that, compared with the control group, those who left the hospital would have significantly better mental states, social functioning, and social networks at follow-up—was, overall, rejected. No psychiatric or social differences were noted between groups over time, a similar finding to that of the north London TAPS study (
26). Improvements in social networks were noted among patients who were discharged, but similar gains were noted in the control group of patients who were not discharged, which supports the interesting possibility that the hospital closure process produced benefits both for those who were discharged and for those who remained in the hospital during the initial stages of the closure.
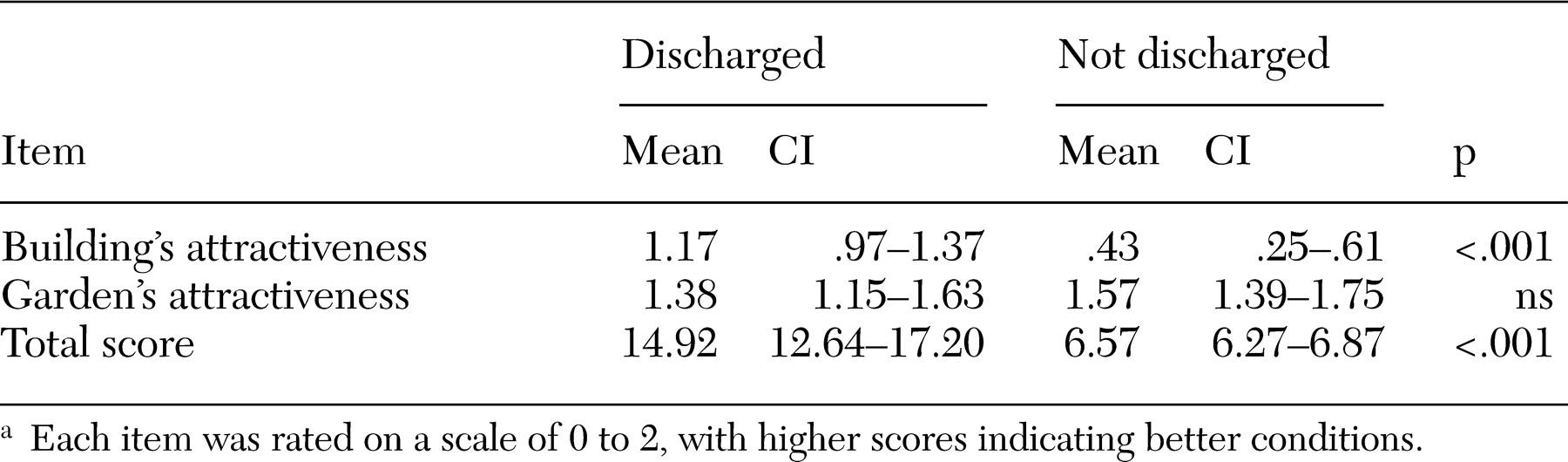
Our results led us to accept the second hypothesis—that community settings would provide a significantly better environment than the hospital. On almost all the environmental measures, the community settings were rated better than the hospitals, and the main effects of leaving the hospital for patients was to offer a less restrictive social environment.
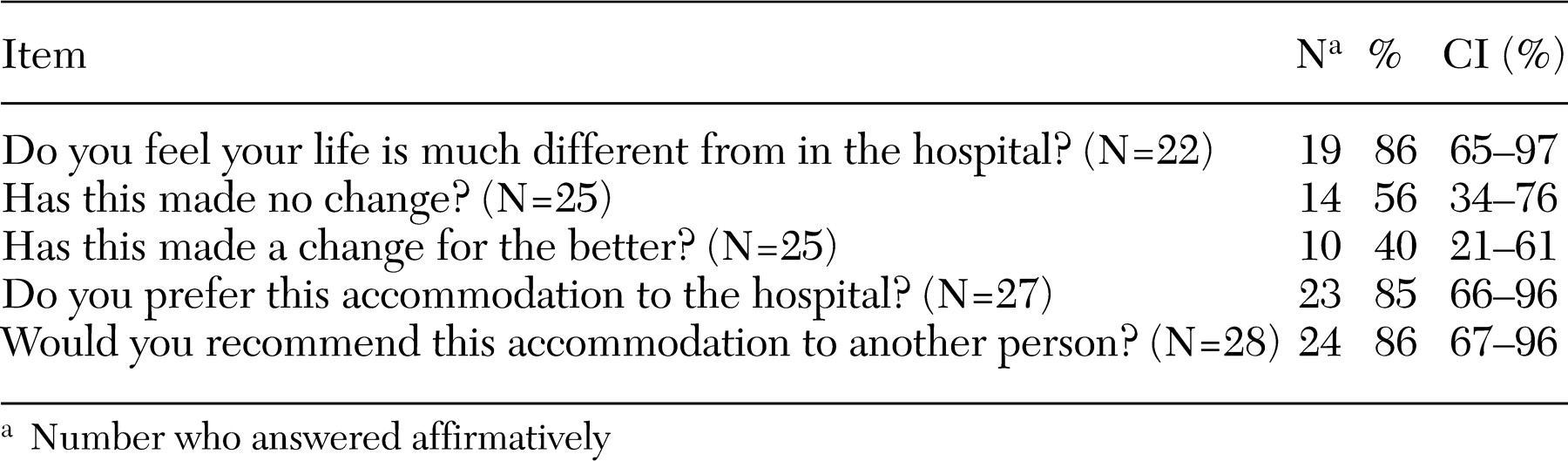
The results also gave us strong grounding to accept the third hypothesis—that discharged patients would favor community care after discharge from the hospital. For many of the discharged patients, discharge was one of the most notable events of their adult lives. They had lived in a hospital for an average of 32 years; it is difficult to imagine a more profound planned interruption to their daily routine. Before the patients left the hospital, few attitudinal differences were noted between the two groups. Only one-third of the discharged patients wanted to stay in the hospital. At follow-up, they were asked in detail about their experience of living outside the hospital, and their answers were quite clear: 86 percent said they would recommend their new home to others; these findings reinforce those of previous studies (
16). This accumulating evidence does now fairly clearly establish that the large majority of long-term patients discharged within a planned reprovision program prefer their new community homes to the hospital. Much of the change in patients' attitudes can be understood in relation to the environmental quality of these community homes, which offered greater choice and autonomy for their residents in terms of everyday activities.
Interestingly, the perspective of the patients has been discussed relatively little in the literature on deinstitutionalization. Any studies that have been conducted have tended to be small and uncontrolled (
27,
28,
29). Long-term patients themselves tend to be more optimistic than both their families and staff about their ability to live independently after discharge from the hospital (
30,
31,
32,
33) and to be more favorable about plans to transfer other long-stay patients to community-based residential settings (
19,
33).
The internal generalizability of the study results is reasonably strong. The patients selected for the study were representative of the wider population of all long-stay inpatients in the study hospitals. The study's external generalizability is also good in that patients who participated in studies of six other long-stay hospitals in England had very similar characteristics (
34).
Our study was limited by its focus on one patient group, largely elderly, long-stay general adult patients, at the exclusion of forensic patients and acute admissions. Although more detailed in its assessments and scope than comparable studies, our study nevertheless had a relatively small sample. The views of patients' relatives were not assessed; in fact, very few patients retained any contact at all with their relatives—the average number of family members in contact with each patient was less than one at both baseline and follow-up. Because some of the patients were frail, the numbers of patients who were able to complete some of the ratings, both at baseline and at follow-up, were limited, despite the fact that up to six attempts were made to interview some patients. Because most of the patients included in the study were elderly—and in some countries would be treated through psychogeriatric rather than general adult services—the results of this study need to be applied with caution to other treatment settings, depending on their configuration for long-term patients with psychotic disorders.
In terms of the study's strengths, the patients who were discharged were selected from a defined catchment area; interview data were collected prospectively; discharged patients were closely matched with patients in the control group of nondischarged patients, with a 1:2 matching ratio to increase the power of the analyses; and a wide range of outcome measures was used, including detailed assessments of symptoms, social behavior, physical illness, social networks, patients' attitudes, and quality of the environment.
These findings reinforce and extend those of similar studies worldwide, particularly those in Australia (
35), Canada (
36), Finland (
37), Germany (
38), Italy (
39), New Zealand (
40), Southern Europe (
41), and the United States (
42,
43). In effect, the service users themselves, who are the primary intended beneficiaries of the whole deinstitutionalization process, were strongly in favor of the community alternatives, which has emerged in some previous work (
44,
45), even though national policy in Italy has been to allow older patients who are already living in long-stay hospitals to remain there indefinitely but to change the pattern of care slowly by admitting all new patients to smaller local inpatient units (
46,
47). These results give further qualified support, consistent with earlier findings, for moving long-stay psychiatric patients from hospital to community settings, as long as sufficient funding is available to provide a good quality of care in the community (
40).