Patient Management Exercise A Person-Centered Approach to Treatment
Abstract
CASE VIGNETTE PART 1
Decision Point A:
| A1._____ | Taper fluoxetine to discontinuation and introduce another antidepressant. |
| A2._____ | Prescribe a mood stabilizer. |
| A3._____ | Introduce a 5-minute meditation, in which, with eyes closed, attention is concentrated on an internal experience, such as love or hope. |
| A4._____ | Monitor alcohol and drug use. |
| A5._____ | Offer that he take the Temperament Character Inventory (TCI), either with a paper copy or on a computer. |
CASE VIGNETTE PART 2
| Temperament | Novelty Seeking: 15th percentile (low) Harm Avoidance: 99th percentile (high) Reward Dependence: 45th percentile (average) Persistence: 55th percentile (average) |
| Character | Self-Directedness: 1st percentile (low) Cooperativeness: 65th percentile (high average) Self-Transcendence: 20th percentile (low) |
Decision Point B:
| B1._____ | Continue current regimen. Plan interim follow-up appointment. |
| B2._____ | Suggest he find a leisure pursuit in which he can lose track of time (that is, to cultivate self-forgetfulness, the first stage of Self-Transcendence). |
| B3._____ | Invite reflection, curiosity about himself and his experiences. |
| B4._____ | Encourage him to acquire a pet to build reward dependence. |
| B5._____ | Prescribe low-dose atypical antipsychotic medication. |
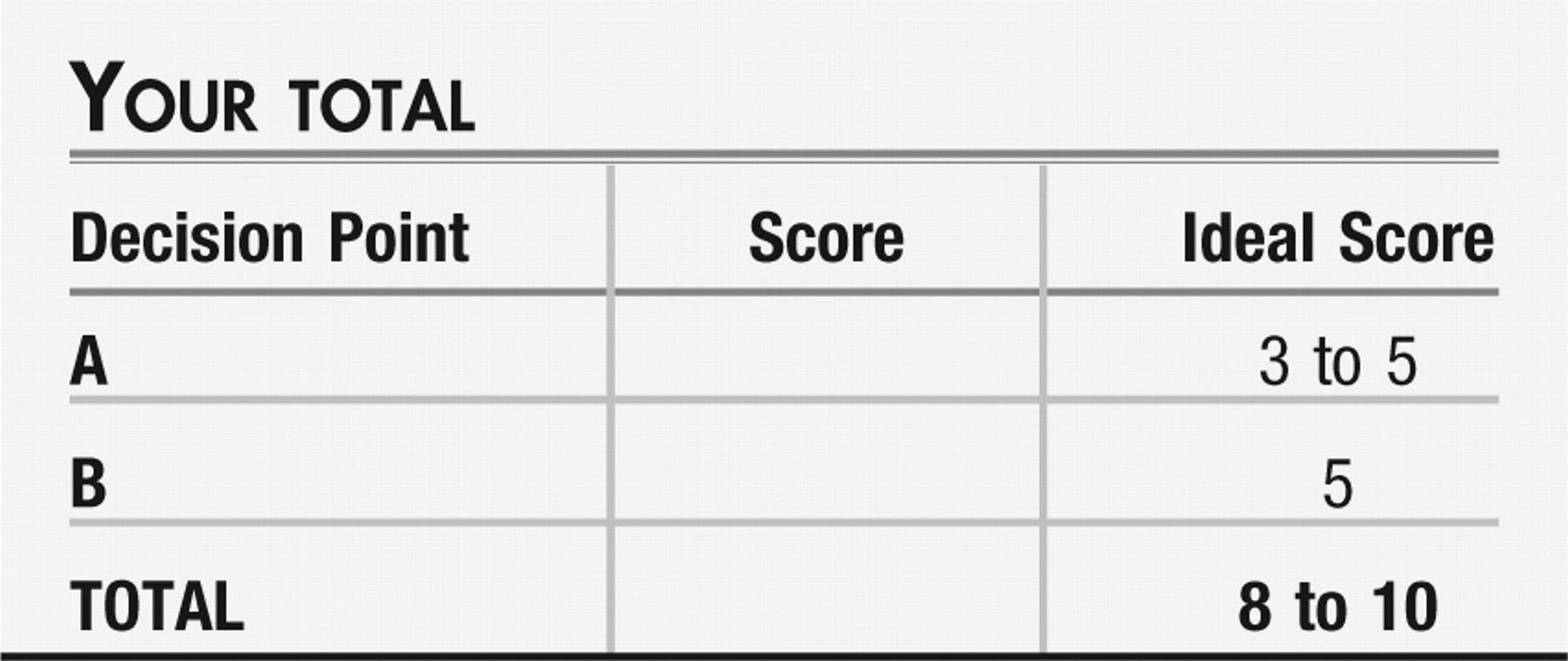
ANSWERS: SCORING, RELATIVE WEIGHTS, AND COMMENTS
Decision Point A:
| A1._____ | Taper fluoxetine. (−1) A reasonable current practice but not coming out of the Person-Centered Therapy approach being emphasized here. |
| A2._____ | Prescribe a mood stabilizer. (−2) Although this is entirely a reasonable intervention, it is an overtly directive response, emphasizing the professional expertise of the provider and minimizing the contribution of the particular person of the patient. This will be especially necessary when an individuals are deeply distressed by the symptoms of their mental illness and have restricted personal wherewithal to move toward well-being. One may need to stabilize them, recover function, and then help them to appreciate their own strengths, progressing into a more balanced and evenly regulated self-with the principles of Person-Centered Therapy. |
| A3._____ | Introduce a meditation. (+3) Clearly a Person-Centered Therapy response. The aim of this exercise is to offer a setting for the first stage of self-aware consciousness. |
| A4._____ | Monitor substance use. (0) A more directive response, shifting the balance of power in the therapeutic relationship more toward the psychiatrist. Again, at times, our patients need a more supportive approach. It is our best service to them to know when to “graduate” them to more independent thinking. |
| A5._____ | Offer the TCI. (+2) Partly a Person-Centered Therapy response. This personality assessment tool will provide you and he with a description of himself, facilitating a greater understanding and the basis for validation and rapport. The possibility of transformation requires the recognition of the currently held position before authentic personal growth can occur. |
Decision Point B:
| B1._____ | Continue current regimen. (0) A neutral intervention, considered to be typical and reasonable current practice but not coming out of the Person-Centered Therapy approach being emphasized in this issue of FOCUS. |
| B2._____ | Suggest leisure pursuits. (+2) Partly a Person-Centered Therapy response. This intervention will give him the opportunity to build Self-Directedness, in that he will have to decide for himself what activity he would like to do to complete the assignment. Self-forgetfulness is the first stage in the development of Self-Transcendence, which needs to be cultivated to achieve a greater sense of overall well-being and satisfaction in life. The idea is to find a pastime in which he becomes so absorbed as to lose track of time; this may be challenging given his low Novelty Seeking (he would prefer a well-defined assignment with rules and a clear endpoint, for example, “Do a 500-piece jigsaw puzzle”). |
| B3._____ | Invite reflection. (+3) Clearly a Person-Centered Therapy response. With the patient showing some improvement in symptoms of depression, anxiety, and irritability, it is a reasonable time to encourage exploration of the principles of Person-Centered Therapy: letting go, working in the service of others, growing in awareness and increasing knowledge in the processes of thought. |
| B4._____ | Recommend a therapeutic pet. (−1) A more directive response and showing some “thinking outside the box,” but this again is using the physician's judgment in lieu of the patient's to suggest an activity. One must be careful in Person-Centered Therapy, because an individual with low Self-Directedness will look to the therapist anxiously for guidance, and one's natural tendency might be to offer counsel or advice. The optimal therapeutic benefit will be derived if the therapist can be supportive but not overtly directive, allowing the person to discover and declare his own inclinations. (Obtaining a plant or a pet could help an individual develop Self-Directedness and may contribute to promoting Reward Dependence.) |
| B5._____ | Prescribe a low-dose atypical antipsychotic. (−2) Although this could be an adjustment of the patient's medication regimen, it is another overtly directive response, emphasizing the professional expertise of the provider and minimizing the contribution of the particular person of the patient. |
RECOMMENDED RESOURCES
Information & Authors
Information
Published In


History
Authors
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).