The notion has been gaining support that for some patients with schizophrenia, origins of the illness date back to aberrations in early brain development. Previously, we reported on 2 cases of patients with schizophrenia who had evidence on MRI brain scans of a neuronal migration abnormality, gray matter heterotopia (GMH).
1 GMHs are collections of normal neurons in abnormal locations secondary to an arrest of radial migration of neurons. In the era of computed tomography, this type of abnormality was thought to be associated only with very gross developmental delay in cognition, motor, and language skills. However, with the advent of magnetic resonance imaging and clearer distinction between gray and white matter, gray matter heterotopias have been shown to occur in patients without significant mental or motor retardation, although they are frequently associated with seizures.
2Our previously published report of the 2 patients with schizophrenia and GMH was the first to document this type of abnormality in association with schizophrenia, although there has been 1 case report of gray matter heterotopia in a patient with bipolar affective disorder.
3The case reports we published previously were not identified through a systematic study looking at consecutive scans, so we were unable to estimate how frequently this abnormality is found in patients with schizophrenia or in normal individuals. The present study was a visual inspection of brain MRI scans specifically designed to assess the incidence of neuronal migration abnormalities, in particular GMH, in a population of patients with schizophrenia compared with healthy control subjects.
METHODS
Patients were obtained through the Mental Health Clinical Research Center at The University of Iowa Hospitals and Clinics. Recruitment was based on psychiatric diagnosis within the schizophrenia spectrum. Control subjects were obtained from the community via advertisement. Subjects (patients or controls) were excluded if they had histories of major head trauma, neurological disease, or serious medical disease. Patient diagnoses were established by consensus of at least four psychiatrists (the authors). All subjects provided written informed consent.
The sample was defined as all the scans obtained consecutively within the preceding 24 months. The study included 55 patients with DSM-III-R diagnoses of schizophrenia (n=52) or schizoaffective disorder (n=3) and 75 healthy control subjects. There were no significant differences between the two samples for male/female ratio, age, parents' education, or parents' socioeconomic status.
All subjects were scanned with a 1.5-tesla GE Signa Scanner using a spoiled GRASS (gradient radiofrequency at steady state) sequence with the following parameters: 1.5-mm coronal slices, flip angle 40, 24/5 (TR/TE), number of excitations=2, field of view=26 centimeters, matrix 256×192. This sequence yields 124 contiguous slices through the entire brain. Three separate imaging sequences are obtained: T1, T2, and proton density (PD). Hard copies of the films were used for visual inspection. All control and patient films were combined in random order and visually inspected by two psychiatrists, blind to diagnosis and well versed in neuroanatomy (P.N., V.S.). The films were viewed slice by slice through the entire brain for evidence of ectopic areas of gray matter. Any GMH identified was confirmed by a neuroradiologist.
RESULTS
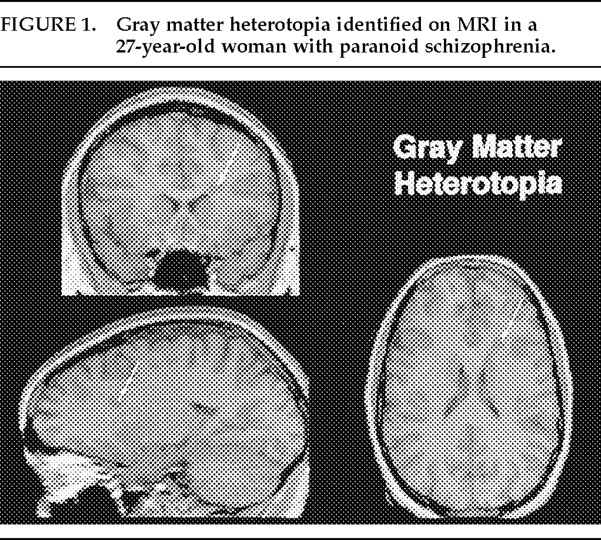
Within the control group, there was no evidence of any brain with ectopic gray matter. However, within the patient group, 1 patient was found to have a well circumscribed, lobular GMH located in the left frontal lobe near the superior portion of the lateral ventricle (
Figure 1). This patient was one of the two we had described in our previous case report. The patient was a 27-year-old woman with paranoid schizophrenia. She had no history of developmental delay, cognitive deficits, seizures, or abnormal movements.
The differential diagnosis of the lesion found in this case is broad and includes neoplastic, inflammatory, and vascular lesions. However, the clinical picture is inconsistent with any of these processes. In addition, the MRI findings would be quite different in such conditions. The lesion showed a signal intensity in all three imaging sequences that was analogous to cortical gray matter—the most important finding in the MRI diagnosis of GMH.
4,5 Although the subependymal lesions of tuberous sclerosis are a consideration, these nodules are usually iso- to hypointense compared with white matter
6 and can therefore be ruled out by radiological evidence as well as by lack of supporting clinical findings.
DISCUSSION
The process of neuronal migration is vital to the formation of the cortex and begins early in gestation. The development of GMH has been suggested to be caused by an underlying genetic susceptibility coupled with an environmental insult (toxic, infectious, or teratogenic) during the second trimester of gestation.
7 This proposed etiology is very similar to a proposed etiology of schizophrenia in which environmental insult during the second trimester of gestation may increase the likelihood of developing the disorder. Reports have indicated not only viral infection,
8 but also maternal malnutrition
9 and Rh incompatibility
10 as factors that increase the risk of developing schizophrenia. Therefore, it appears that the type of stress is not as important as the timing of stress during a critical point in gestation that may lead to an increased risk. By the fifth month of fetal development, most neurons destined to compose the neocortex have been generated, but many have not yet migrated to their target structures, nor have they become positioned or appropriately connected
11—thus implicating the second trimester as a pivotal period for possible disruption of normal cortical development.
The low incidence of GMH (1 in 55, or 1.8%) in this study makes generalizing the findings difficult. However, this abnormality may occur more frequently at a microscopic level that is undetectable by current brain imaging methods. This possibility is supported by the report by Akbarian,
12 which shows microscopic evidence of neuronal migration in both the frontal and temporal lobes of patients with schizophrenia.
GMH was not present in any of the control scans. With the understanding that the pathophysiology of GMH is a relatively gross disruption of normal brain development, it seems unlikely that such an aberration would go unmanifested or be considered incidental. Indeed, there is no literature to suggest that this anomaly occurs in normal persons.
2 Recruitment of control subjects by advertisement can, however, introduce ascertainment bias because it does not sample the entire community, only those who respond to the advertisement. Yet if healthy control subjects had this type of anomaly, it is unlikely that they would be systematically excluded from this type of ascertainment.
Although the proposed etiologies of GMH and schizophrenia are very similar, this abnormality is clearly not specific to schizophrenia. It is quite likely that GMH is associated with a variety of developmental neuropsychiatric illnesses. For example, a type of neuronal migration abnormality, cortical dysplasia, has been reported to be associated with autism.
13 Further research into the pathophysiology of early brain development may be of help in understanding the mechanisms that underlie such illnesses.
ACKNOWLEDGMENTS
Special thanks to William T.C. Yuh, M.D., Ph.D., Department of Radiology, for his assistance in reviewing scans. This research was supported in part by National Institute of Mental Health Grants MH31593, MH40856, and MHCRC 43271; the Nellie Ball Trust Fund; Iowa State Bank and Trust Company, Trustee; and NIMH Research Scientist Award MH00625.