Acquired Obsessive-Compulsive Disorder Associated With Basal Ganglia Lesions
Abstract
PATIENTS
CASE HISTORY/CLINICAL COURSE
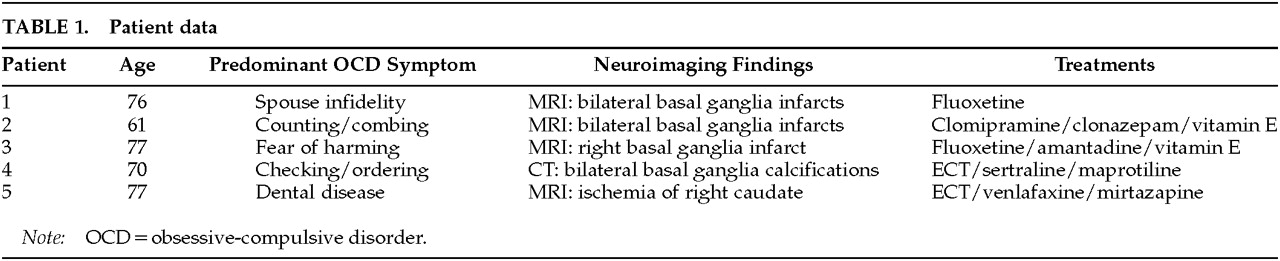
Patient 1 is a 76-year-old married Caucasian woman who began treatment for depression when she was in her late 50s. After more than a decade of treatment for depression with tricyclic antidepressants, she developed OCD at age 72, with a prominent obsession that another woman might seduce her husband. The obsession was ego dystonic, but she nevertheless acted on a compulsion to continually monitor his location. At hospitalization, an MRI of the brain showed lacunar infarcts in the basal ganglia bilaterally. The etiology of the lesions is not known; there is nothing in her medical history that points to a causative factor. Her OCD was treated successfully with fluoxetine 40 mg qd, and her depressive symptoms subsequently resolved as well.
Patient 2 is a 61-year-old divorced African-American woman who developed OCD in her late 50s. She became obsessed with the thought that her neighbor might set her house on fire. She began counting drawers and cabinets in her kitchen many times per day and combing her hair repetitively, despite being sufficiently groomed. The thoughts were ego dystonic, and she became very anxious if she did not perform the counting and combing behaviors. She was misdiagnosed in a community clinic as having a psychotic disorder and treated with a typical antipsychotic. Her OCD did not improve, and she developed tardive dyskinesia (TD).As her mood became more depressed, she was admitted to the hospital. Our evaluation included an MRI of the brain, which revealed bilateral basal ganglia infarcts. Borderline hypertension was noted in her past medical history at admission, and this may have been an etiological factor for the infarctions. She was diagnosed with OCD and major depression. We discontinued her antipsychotic treatment and placed her on clomipramine 225 mg qd, clonazepam 1.75 mg qd, and vitamin E 400 IU tid for TD. Her TD has resolved partially over 6 months.
Patient 3 is a 77-year-old married Caucasian woman who was admitted to our hospital service with ego-dystonic obsessions of a sexual nature regarding God, as well as obsessions that she would inadvertently harm someone in public and that she might kill her husband. Before coming to our attention she was treated for 10 years in another clinic for a psychotic disorder. She did not have psychiatric symptoms necessitating treatment prior to age 67. At that time she began treatment with haloperidol and then, after developing parkinsonism, was switched to risperidone. Upon admission to our service she had tongue fasciculations, bilateral upper and lower extremity tremors, head tremors, and truncal movements. Her Abnormal Involuntary Movements Scale score was 20. An MRI of the brain showed a right basal ganglia infarction. We discontinued risperidone and began treatment with fluoxetine for OCD and amantadine and vitamin E for parkinsonism. Both the OCD and the parkinsonism improved prior to discharge.
Patient 4 is a 70-year-old married Caucasian woman who had suffered from depression for almost 25 years. She had had five prior psychiatric hospitalizations since 1975 and was treated with maprotiline. Over the past several years she had begun developing OCD symptoms. She would ask her husband for reassurance in performing daily routine tasks, check the mirror for facial abnormalities, and organize her bathroom, all on a repetitive basis. Clinically, her depression always exacerbated her OCD. For approximately 2 years she has been treated with ECT and an outpatient combination of maprotiline 200 mg qhs and sertraline 50 mg qd. A CT of the head obtained at her last admission revealed bilateral basal ganglia calcifications. The etiology of these lesions is unknown, and there is nothing in her history to indicate a causative factor. At discharge, following another course of ECT, she was started on sertraline 100 mg qd and had remissions of both OCD and depression.
Patient 5 is a 77-year-old widowed Caucasian woman admitted to our service for the treatment of OCBs that developed precipitously about 2 years prior to admission. From 1988, following her husband's death, until the onset of OCBs, she was stabilized with pharmacotherapy. The OCBs developed after undergoing routine dental work. She developed an obsession that her teeth remained diseased and spent an inordinate amount of time seeking dental evaluations from various dentists. Her ego-syntonic obsessions and compulsions were treated initially with paroxetine, with temporary improvement. The symptoms returned and were followed by a decline in her mood and functioning. Several other outpatient treatments were attempted but failed, including venlafaxine, fluvoxamine, and lithium augmentation.At admission, an MRI of the brain revealed ischemic changes in the head of the right caudate, the right lateral frontal convexity, and the left lateral parietal convexity. The etiology of these lesions is unknown. She underwent ECT with a course of six uncomplicated treatments. After the treatments her mood returned to premorbid baseline and she no longer mentioned having problems with her teeth.
DISCUSSION
References
Information & Authors
Information
Published In

History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).