Prevalence of PD Depression
Forty-five Parkinson's disease and depression prevalence reports were identified and reviewed. Our analysis begins with Patrick and Levy's 1922 study
7 of 146 patients, in which 10 (7%) were determined to have depression. Mjones's 1949 study
8 reported 40% of his PD patients to have depression. Three studies in the 1960s
9–11 found occurrence of depression in patients ranging from 7% to 67%. In the 1970s, six studies
12–17 noted depression occurring in between 29% and 70% of patients assessed. In the 1980s, 21 studies
18–38 continued to report variability regarding the presence or absence of depression (12%–70%). The variability in reported depression persisted in the 1990s, with a range of reported depression between 7% and 68% in 13 studies.
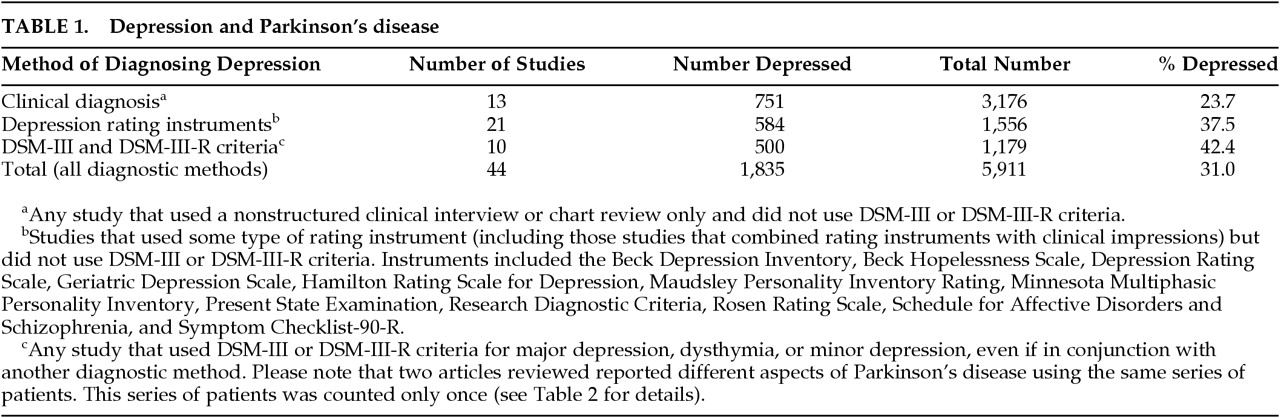
3,39–50 When all studies were combined, the number of PD patients equaled 5,911, the number depressed 1,835, and the percentage depressed 31.0%. Please see
Table 1 for the prevalence of PD depression in all the reports we obtained, broken down by method of diagnosis.
Of the 45 articles reviewed, 11 specifically used DSM-III and DSM-III-R criteria.
3,20,21,26,31,37,38,44,46,48,50 DSM-III criteria were first used for depression diagnosis in Parkinson's patients in the study by Mayeux et al. in 1984,
20 but this did not become commonplace until the late 1980s. The combined rate of occurrence of both major depression and minor depression found in these studies using DSM criteria was higher than the overall average prevalence of all studies examined. Please see
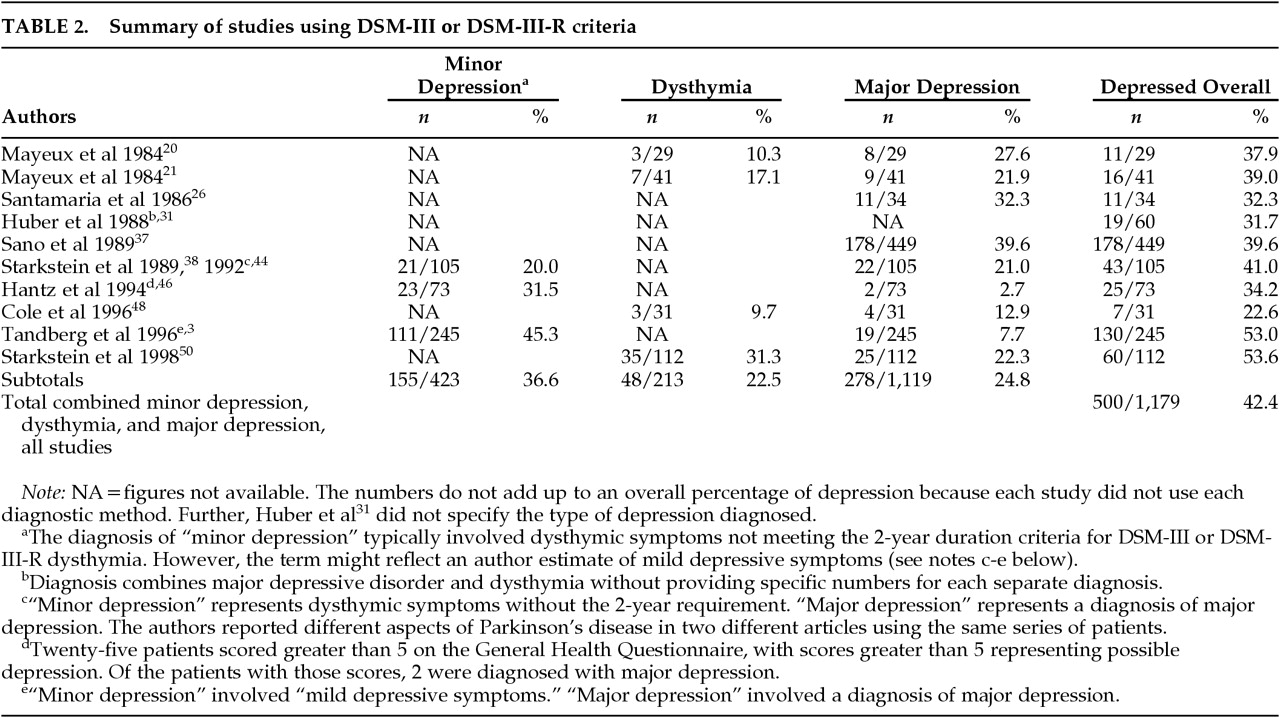
Table 2 for a specific breakdown of all reports that used any type of DSM diagnosis. The diagnosis of minor depression typically involved dysthymic symptoms not present for 2 full years or more, although one study applied the term to “mild depressive symptoms.”
3 In the four studies reporting dysthymia, it was noted present in 48 of 213 PD patients evaluated, or 22.5%.
20,21,48,50 Minor depression was diagnosed in three studies involving 155 of 423 PD patients evaluated, or 36.6%.
3,38,46 Major depression was found in 278 of 1,119 patients evaluated, or 24.8%.
3,20,21,26,37,38,46,48,50 When all diagnostic categories were combined—minor depression, major depression, and dysthymic disorder—500 of 1,179 PD patients were reported depressed, or 42.4%.
Clinical Manifestations of PD Depression
A review of the aforementioned studies revealed some proposed unique characteristics of depression complicating Parkinson's disease. Taylor et al.
27 described episodes of “emotional upset” usually accompanying exacerbation of PD symptoms. Brown et al.
51 noted “lowered arousal” involving apathy and diminished self-initiated planning, psychomotor retardation, and a mood that was “environmentally dependent” (involving an externalized locus of control for mood and mentation as well as movement) accompanied by marked decrease in concentration. Brown et al.
51,52 noted a tendency for dysphoric states to complicate more the “off” than the “on” periods in PD. Cummings
5 noted the following as the most reliable indicators of depression in Parkinson's disease: dysphoria, pessimism, irritability, sadness, and suicidal ideation.
Starkstein et al.,
53 in a series of 105 patients (21 with major depression, 20 with minor depression, and 64 with no depression), observed that major depression significantly correlated with longer duration of Parkinson's disease and greater frequency of a personal history of depression prior to the onset of PD. Starkstein et al. considered that unilateral left hemispheric presentation of PD conveyed a greater risk of depression than right hemispheric presentation.
Although PD patients may experience more suicidal ideation, suicide is not common in the Parkinson's disease patient population.
5,54 Stenager et al.
54 reviewed the cause of death in 458 previously well-characterized PD patients (226 men, 232 women). Death certificates were examined for primary and secondary causes of death. When the PD patients' causes of death were compared with those in the general population, there was no increased risk for suicide in that patient population. It remains unclear why an increased rate of depression is not accompanied in PD patients by an increased risk of suicide.
Psychosis in PD is not uncommon and is often associated with an excess of dopaminergic agents. Whether psychotic depression is common in PD has not been established.
55Proposed Etiology of PD Depression
Physical morbidity suggests that the etiology of depression complicating Parkinson's disease is likely related to the neuropathology of PD. Gotham et al.,
66 Ehmann et al.,
67 Cantello et al.,
68 Brown and Jahanshahi,
69 and others
16,70,71 comparing depression in PD to depression in other medically ill patient populations found that PD did appear to result in a greater degree of depression than other comparable medical illnesses.
Tandberg et al.
3 argue that PD depression is more likely due to neuropathological changes in the brain than to environmental and psychological factors. They base their conclusions on a study of 245 PD patients in which those with depression and those without depression were compared. Tandberg et al.
3 noted that those meeting diagnostic criteria for major depression scores on the Montgomery-Åsberg Depression Rating Scale experienced greater cognitive impairment on the MMSE,
58 as well as an increased risk of thought disorder measured by the Unified Parkinson's Disease Rating Scale (UPDRS) and greater impairment in activities of daily living. Starkstein et al.
53 also observed greater cognitive impairment as measured by the MMSE, and they saw the pattern of deficits on neuropsychological measures that indicates greater involvement of frontal lobe functions than other brain regions. Cognitive impairment is associated with both duration of PD and severity of the movement disorder.
57 Improvement in physical symptoms alone, however, does not predict recovery from depression.
44Mayeux et al.
21 report the association of decreased levels of serotonin in the central nervous system, as measured by decreased levels of 5-hydroxyindoleacetic acid (5-HIAA) in the cerebrospinal fluid (CSF). Levels of 5-HIAA were significantly lower for depressed PD patients (major depression or dysthymia) than nondepressed PD patients or control subjects. Further, patients diagnosed with major depression have lower 5-HIAA levels than those diagnosed with dysthymia.
21 Paulus and Jellinger
43 reported more severe reduction of dorsal raphe nucleus serotonergic neurons in the brains of PD depressed patients than nondepressed PD patients.
The role of other neuromodulator, neurotransmitter, and neuropeptide abnormalities associated with PD in the production of PD depression awaits elucidation. The decrease of dopamine in PD may confer an increased risk of depression. Dopamine neurons in the ventral tegmental area (VTA) deteriorate in the course of PD and may contribute to depressed mood.
72 However, it is clear from our own anecdotal experience and that of others
72,73 that dopaminergic agents alone do not alleviate depression. Norepinephrine may also play a part in PD depression. Chan-Palay and Asan
74 noted a correlation of cell loss in locus ceruleus with “atypical depression” in PD. Chia et al.
75 noted that PD depression correlates with decreased CSF levels of homovanillic acid and 3-methoxy-4-hydroxyphenyl glycol (MHPG), reflecting a presumed decrease in dopamine and norepinephrine. However, Paulus and Jellinger
43 did not find a positive correlation of PD depression with a decrease in neurons in the locus ceruleus.
Rogers et al.
29 suggested that PD patients with major depression might have progressive frontal lobe dysfunction, either secondary to pathologic changes in the frontal cortex itself or due to decreased dopaminergic input to the frontal cortex. Mayberg and Solomon
73 proposed that selective disruption of the dopaminergic efferents from the VTA to the orbital frontal and prefrontal cortex, and/or disruption of the orbitofrontal cortex efferents to the dorsal raphe serotonergic neurons, may give rise to PD depression. They hypothesize that disruption of these connections at any point along these two major brainstem-to-frontal-lobe pathways may result in PD depression. If their hypothesis is correct, it remains to be explained why if disruption of the VTA-to-frontal-lobe pathways leads to some PD patients' depression then dopamine replacement alone does not result in amelioration of depression. Perhaps patients with these particular disruptions represent a subset of PD depressed patients who may in fact be responsive to dopaminergic agents but do not routinely have their depression subsequently identified because of this early response of their depression to dopamine. The remaining depressed PD patients may then be those with primary disruption of the serotoninergic pathway. This interplay of dopaminergic and serotonergic pathways in PD depression awaits further elucidation. The potential contribution of norepinephrine, glutamate, or other neurotransmitters and neuropeptides is much less clear at the present time.
In addition to the abnormalities of neurochemistry in PD, psychological factors play a role in PD depression. For example, there is an increased likelihood of early onset depression when Parkinson's disease begins before age 55, even though symptoms may not be severe at this younger age.
38,76 Also, there is the possibility that the degree of disability resulting from the PD itself may convey a greater risk of depression in PD patients. However, Starkstein et al.
44 note that physical improvement in PD symptoms per se does not predict a concomitant reduction in depression. It may be argued that although PD depression and PD disability from physical symptoms of PD are strongly correlated, this association may be more an indication of the severity of underlying neurochemical abnormalities than a psychological depressive reaction to the physical limitations of PD.
Pharmacological Treatment of PD Depression
Given the large number of PD patients who suffer from depression, it is surprising that few controlled clinical trials have been undertaken to evaluate the efficacy and tolerance of pharmaceutical treatment in this population. Of the four classes of antidepressants, tricyclics (TCAs), selective serotonin reuptake inhibitors (SSRIs), norepinephrine reuptake inhibitors, and combined reuptake inhibitors, only the TCAs have undergone the rigorous testing of placebo-controlled, double-blind clinical trials.
5,77TCAs such as amitriptyline and nortriptyline block the reuptake of serotonin and norepinephrine and produce long-term increases in sensitivity in these receptors.
78 Formally, these medications have been the cornerstone in general antidepressant therapy and may be preferred by some neurologists who believe that their anticholinergic properties will contribute to the amelioration of underlying parkinsonian symptoms. However, anticholinergic side effects may induce unwanted conditions in PD patients, including delirium and memory impairment.
79 TCAs are additionally associated with orthostatic hypotension due to alpha-adrenergic blockade. In the course of PD, many patients will experience lowering of blood pressure, and a blockade would be unwelcome. TCA adverse effects depend on plasma concentrations,
80 and with advancing age, levels may insidiously become elevated.
Many clinicians prefer to use SSRIs in treating depression associated with PD. A recent survey of 49 investigators from the Parkinson's Study Group or PSG (this group has experience with over 23,000 PD patients) found that 51% of these physicians use SSRIs first when implementing drug therapy. This is contrasted with the 41% who use TCAs and the 8% who use “other” drugs.
81As previously noted, serotonin levels, as reflected by decreased 5-HIAA CSF levels, are lowest in those PD patients who meet the criteria for major depression,
24 suggesting that SSRIs may be effective in treating PD depression. These medications have some benign side effects, but SSRIs are not associated with alterations in cardiac conduction
80 or alpha-adrenergic blockade,
82 and they neither decrease the seizure threshold
78 nor possess significant quinidine-like properties.
78,82 Possessing no significant anticholinergic properties, SSRIs avoid worsening memory function in PD patients, who are at increased risk of dementia.
Of some concern in using SSRIs is that they are metabolized in the liver by the cytochrome P450 enzyme (CYP) system and may therefore, via competitive inhibition, increase the risk of toxicity from other medications broken down by this system. Specifically, SSRIs competitively inhibit xenobiotic enzymes, which are responsible for the oxidative metabolism of exogenous substances.
82 The main isoenzyme of interest when using these drugs is CYP 2D6, which is involved in metabolizing drugs such as haloperidol, perphenazine, thioridazine, TCAs, codeine, certain beta-blockers, type I-C anti-arrhythmics, methamphetamine, and phenytoin.
82 Among the SSRIs, sertraline and citalopram show less competitive inhibition of CYP 2D6 than does fluoxetine or paroxetine and may carry less risk of toxicity.
Apart from the inhibition of the CYP system, there have been anecdotal reports of a “serotonin syndrome” resulting from the co-administration of antidepressants (including both SSRIs and TCAs) and selegiline.
83 A survey of all investigators in the PSG (75% response) and a study of published cases revealed that in 0.24% (11 cases) of patients taking both an SSRI or TCA and selegiline, patients reported symptoms possibly consistent with the “serotonin syndrome.”
84 Only 2 of the 11 cases (0.04% of total population studied) were considered serious.
84 However, because of these reports, the FDA has requested that the makers of selegiline notify physicians of the possible risk of co-administration of their product with antidepressants.
Concerns have been expressed by some members of the PSG that SSRIs may worsen motor function in PD patients. A recent survey of 49 investigators involved in the PSG found that 37% of physicians administering SSRIs reported at least one patient in whom they felt the drug had been associated with worsening motor function.
81 However, 61% of these physicians continued using SSRIs preferentially to other medications, indicating that this potential risk may be overshadowed by the perceived benefits of these drugs. The survey admittedly did not determine the exact number of patients in whom such motor function impairment may have occurred, and therefore the number of cases may be relatively few. Additionally, PSG-published case reports indicate that discontinuation of the drug treatment will reverse any SSRI-induced motor effects.
81 The most common reasons given by physicians for choosing SSRIs were the side effects profile and perceived greater efficacy of these drugs. Users of TCAs, on the other hand, noted the soporific benefit of TCAs and the physicians' experience with this class of medication
81 as reasons to utilize them.
An open-label trial involving 15 patients taking sertraline for approximately 7 weeks found that 10 improved, 1 was unchanged, and 4 worsened (according to the Beck Depression Inventory).
85 Their UPDRS scores and evaluations of individual energy levels were unchanged.
85 Note that 2 of the 15 patients included in the final data discontinued treatment during the trial and 1 was taking a reduced dose of 25mg/day as opposed to the predetermined 50 mg/day.
85 Our own unpublished experience with 10 consecutive patients on open-label sertraline (1 receiving 25 mg and 9 receiving 50 mg) revealed that 9 of 10 patients had moderate to complete resolution of depression symptoms on the Clinical Global Rating of Depression. The 10th patient reported an increase in anxiety and motor restlessness requiring discontinuation of sertraline and introduction of lorazepam 0.5 mg morning and afternoon and 1.0 mg at bedtime. After treatment of anxiety, this patient resumed sertraline 50 mg in the morning with resolution of depressive symptoms. No worsening of PD symptoms resulted from the sertraline treatment. No patient was considered to have a change in PD symptoms as measured by a clinical rating of Parkinson's symptoms by the treating neurologist.
Recent review articles concerning the treatment of depression in the elderly and/or PD patients indicate that medications such as venlafaxine, nefazodone, and mirtazapine may prove to be efficacious.
80,83,86,87 These medications appear to have comparable efficacy to drugs more commonly used (TCAs, SSRIs) but may have fewer adverse side effects than TCAs.
80,83,86–90 However, an extensive literature search did not yield a case series or clinical trial of any of these newer drugs in PD patients. The few case reports on non-TCA and non-SSRI medications in PD are initially negative or lacking altogether. In one case the patient became “much worse” the day after starting on nefazodone and greatly improved after discontinuing the drug.
91 A case report noted psychosis in a PD patient after mirtazapine was added to the patient's chronic levodopa regimen.
92Bupropion, thought to act by means of a norepinephrine effect, was reported by Goetz et al. to alleviate depression in 5 of 12 PD patients.
93 Concerns have been noted regarding bupropion's potential to cause seizures and its dopaminergic effects.
79,81,86,93 It may be most prudent to use bupropion after attempts with TCAs and SSRIs have failed.
81Although citalopram has been available in Europe for 10 years, our MEDLINE search of studies with depressed PD patients revealed no reports regarding citalopram usage in PD depression. Our MEDLINE search did not identify articles reporting venlafaxine usage with PD patients. Venlafaxine's dual effects on serotonin and norepinephrine may prove beneficial in PD patients deficient in these neurotransmitters. Its potential side effect of elevating blood pressure, which occurs in 3% of treated patients, may benefit hypotensive PD patients.
Double-blind control studies indicate the efficacy of TCAs in the pharmacotherapy of PD depression, although at the risk of potential lowering of blood pressure secondary to alpha-blockade, and of delirium and worsening of comorbid dementia from anticholinergic side effects. Current anecdotal experience with large numbers of patients by members of the PSG,
82 ourselves, and others,
85 suggests the efficacy of SSRIs in the resolution of PD depression.