As to the first difficulty, there are several key issues in establishing TBI as the etiology of a psychotic condition. 1) What severity of TBI is significant enough to cause a psychosis? 2) How long after an injury is the TBI considered to be etiologically relevant to the development of a psychosis? and 3) What laboratory findings are associated with psychosis?
Another difficult differential is with Psychosis Due to Seizure Disorder (PDSD). Schizophrenia-like psychosis occurs 6 to 12 times more frequently in patients with seizure disorder than in the general population.
15,16 At the same time, seizure disorder is also a common sequela in patients with posttraumatic psychosis. Studies have found that 33% to 58% of patients with PDTBI also experienced seizures.
7,13 In addition, EEG abnormalities in the temporal lobes have been reported in patients without a documented history of seizure disorder. It is also possible that these patients experienced seizures that were not reported.
13 This high comorbidity between psychotic symptoms, head injury, and seizure disorder has led some researchers to speculate that the subsequent psychosis in PDTBI patients may actually result from the secondary seizures. Thus the secondary seizure disorder would be the intervening variable between TBI and the development of psychosis.
17 In such cases the differential between PDTBI and PDSD is difficult to determine.
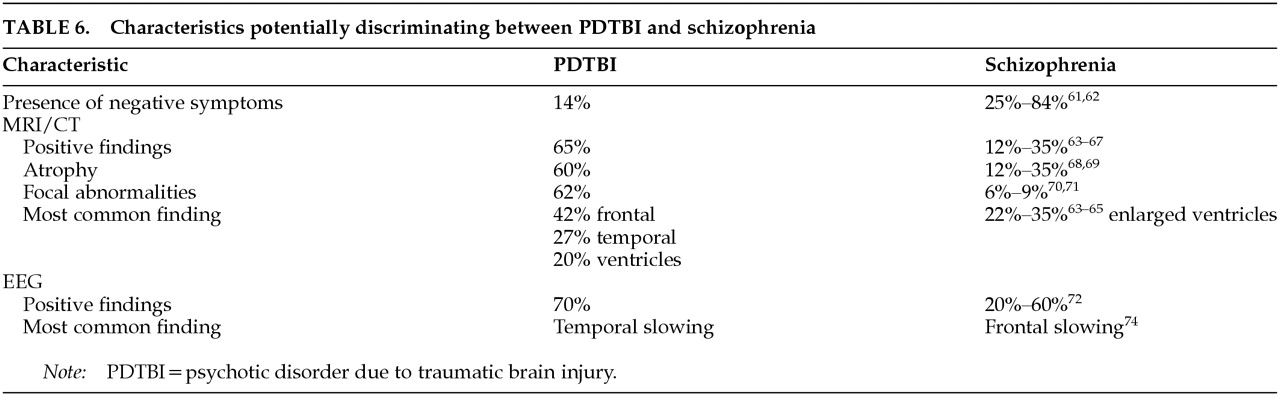
The present study examines characteristics of PDTBI through an analysis of case studies in the literature. The purpose of the study is to provide descriptive information to assist in diagnosis of PDTBI. This information would be useful in ruling out other mental conditions such as schizophrenia or seizure disorder when formulating a diagnosis for a psychotic patient who has a history of TBI. Specifically, we focus on three questions: 1) What are common characteristics of PDTBI? 2) What historical, physical, or laboratory findings are associated with PDTBI? and 3) What are some characteristics that discriminate between PDTBI and schizophrenia, and PDTBI and seizure disorder?
METHODS
A comprehensive literature search of psychiatric, psychological, neurological, and medical journals written in English and listed in the PubMed data base was made from the year 1971 to 1997. The literature search focused on cases in which a psychosis developed after a traumatic brain injury and which also reported results of neurological studies such as computed tomography (CT), magnetic resonance imaging (MRI), and electroencephalography (EEG). Specific criteria for inclusion were based on DSM-IV criteria for PDTBI.
1 In addition, cases reporting a family history of mental disorder were excluded.
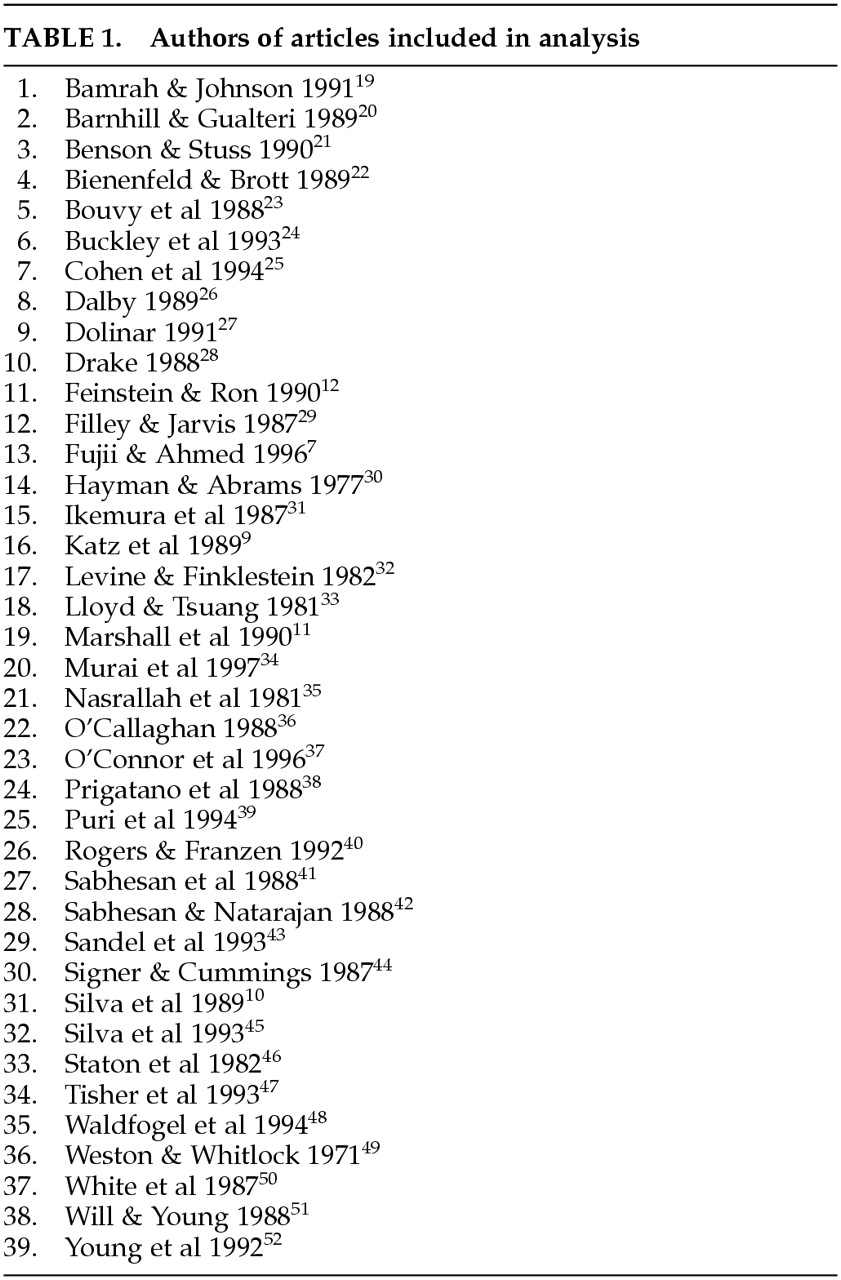
A total of 39 articles were included, yielding 69 cases. The authors of articles are listed in
Table 1.
7,9–12,19–52 The following data were taken for each case: 1) gender, 2) etiology of TBI, 3) loss of consciousness, 4) age when TBI was sustained, 5) age at onset of psychotic symptoms, 6) presence of seizure disorder, 7) family history of mental illness, 8) medications, 9) clinical outcome, 10) presence of negative symptoms, 11) inpatient/outpatient status, 12) diagnosis, 13) presence and type of delusions, 14) presence and type of hallucinations, 15) EEG findings, 16) MRI/CT findings, 17) presence of neurological signs, and 18) neuropsychological test findings.
Severity of TBI was based on criteria set by the Mild Traumatic Brain Injury Committee of the Head Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine (ACRM).
53 According to their criteria, a head injury is considered mild if the duration of loss of consciousness (LOC) is 30 minutes or less and moderate to severe if LOC is longer than 30 minutes.
Psychotic symptoms were rated in the following manner. The presence of negative symptoms was determined by reports of affective flattening, alogia, and avolition. The absence of these behavioral descriptions resulted in the rating of “no” negative symptoms. Positive symptoms of delusions and hallucinations were based on reports and case descriptions. In several cases, more than one type of delusion or hallucination was described; thus the total number of positive symptoms exceeds the total number of subjects. Clinical outcome was based on rating case descriptions of outcome. A three-point system was used to rate outcomes as follows: 1) improved, 2) no improvement, or 3) decline in status.
Localization on EEG and CT/MRI was calculated by the system used by Fujii and Ahmed.
7 In this system, each occurrence of abnormalities is tallied individually. Thus the total number of abnormalities exceeds the total number of subjects.
In many cases, there were missing data because of differences in reporting. All data points for each variable were included in individual analyses despite missing data for the case. Thus for individual variables, the number of cases is often less than the sample size of 69. Given that most data were nominal in nature, analyses were primarily chi-squares. When base rates were known or appropriate, these figures were used in the chi-square calculations. All other calculations are based on chance differences. We also conducted t-tests when appropriate. Because of the exploratory nature of the study and relatively lower power of nonparametric (versus parametric) statistics to detect significant differences between groups, a nonconservative significance level was set at 0.05.
RESULTS
Demographics
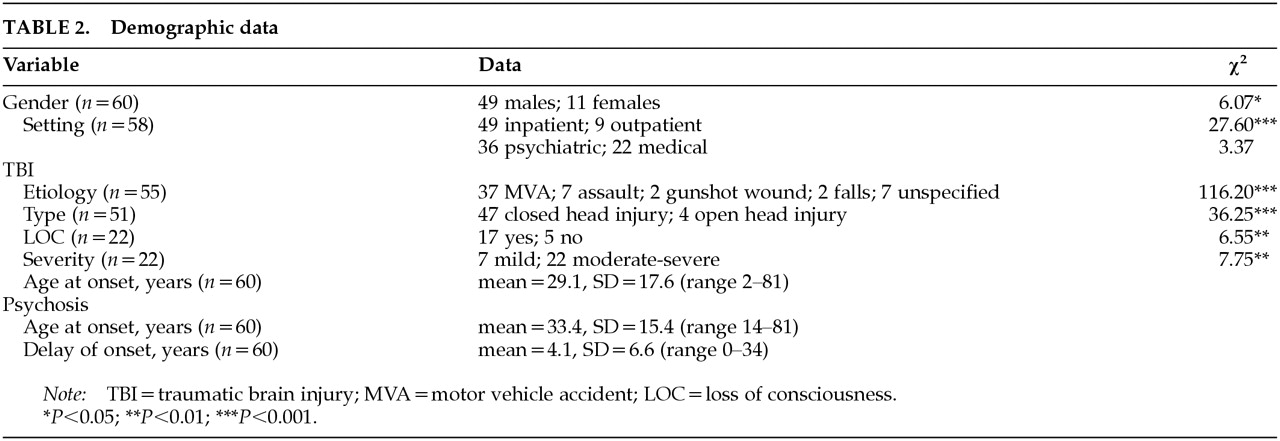
Known demographic data are presented in
Table 2. The sample was composed of 49 males and 11 females. The proportion of males to females was significantly different from the expected (2:1) base rate for TBI (χ
2=6.07, df=1,
P<0.02). The significant majority of our subjects sustained TBI from motor vehicles accidents (67%; χ
2=116.20, df=4,
P<0.001). The second most frequent etiology of TBI was assault (13%), followed by gunshot wounds (4%) and falls (4%). The etiology in 13% of the cases was unspecified. Of the known cases, 92% sustained closed head injuries and 8% open head injuries (χ
2=36.25, df=1,
P<0.001).
A significant majority of the sample (89%) sustained TBI with loss of consciousness (χ2=6.55, df=1, P<0.01). Of the known cases, a significant proportion of subjects sustained moderate to severe head injuries (χ2=7.75, df=1, P<0.01). Most of the subjects (87%) were seen in inpatient settings (χ2=27.60, df=1, P<0.001). No differences were found for whether subjects came from psychiatric or medical settings (χ2=3.37, df=1, P<0.10).
The mean sample age for sustaining a TBI was 29.1±17.6 years (means and standard deviations reported). The mean age for onset of psychosis after head trauma was 33.4±15.4 years. The distribution of scores for mean delay for onset of psychotic symptoms was highly skewed, with a range of 0 to 34 years. The mean number of years after trauma for onset of psychosis was 4.1±6.6. The mode was less than 1 year (38%), and the median was 1 year. Seventy-two percent of the cases reported an onset of psychosis before the mean.
Clinical Presentation and Course
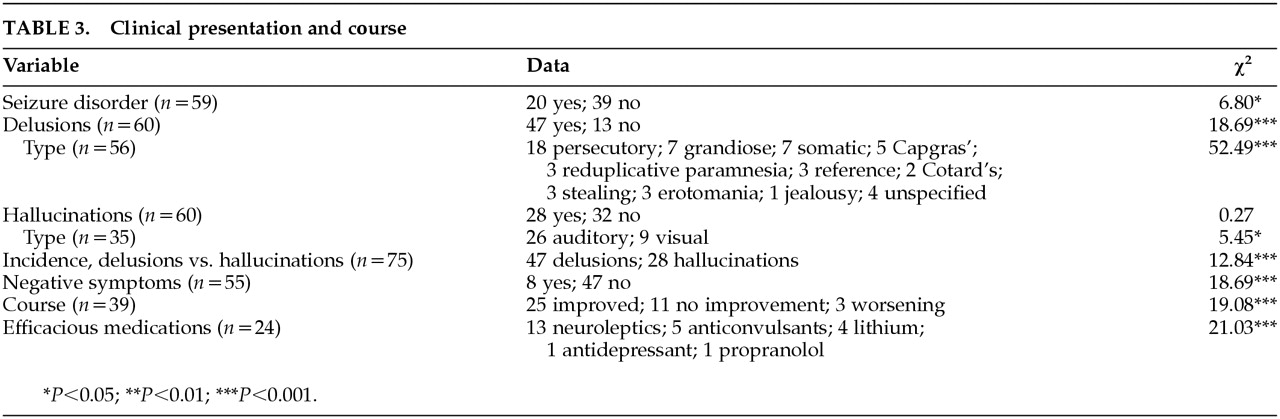
Data for the clinical presentation and course of psychosis are presented in
Table 3. Of the 59 known cases, 20 reported a history of seizure disorder. The resulting proportion of patients sustaining secondary seizures is significantly smaller if compared with chance (χ
2=6.80, df=1,
P<0.01). However, if compared with the highest base rate reported in the TBI literature (12%), the proportion of patients with diagnosed seizure disorder is significantly higher (χ
2=21.03, df=1,
P<0.001).
16A significant proportion of subjects experienced delusions (47/60; χ2=18.69, df=1, P<0.001). By far the most common type of delusion was persecutory (n=18), followed by grandiose and somatic (7 each); Capgras (5); reduplicative paramnesia, religious, reference, stealing, and erotomanic (3 each); Cotard's (2); and jealousy (1). In 4 cases the delusions were unspecified. The proportion of persecutory delusions was significantly higher than chance (χ2=52.49, df=10, P<0.001).
Roughly half the subjects experienced hallucinations (28/60). The proportion of subjects demonstrating hallucinations was not significantly greater than chance (χ2=0.27, df=1, P>0.10). The most common hallucination was auditory (26) followed by visual (9). There was a significantly higher proportion of auditory versus visual hallucinations reported (χ2=5.45, df=1, P<0.02). A comparison of the incidence of delusions versus hallucinations indicates a significantly higher incidence of delusions in the sample (χ2=12.84, df=1, P<0.001).
Of 55 subjects, only 8 reported negative symptoms. The proportion negative symptoms is significantly lower than chance (χ2=18.69, df=1, P<0.001).
In the cases that described the course of psychosis, 25 patients were reported to be improved, 11 reported no improvement, and 3 reported a progressive worsening of symptoms. The proportion of improved outcome was significantly different from chance (χ2=19.08, df=1, P<0.001). In the cases that reported efficacious medications, neuroleptics were cited in 13 cases, anticonvulsants in 5 cases, lithium in 4 cases, antidepressants in 1 case, and propranolol in 1 case. The proportion of efficacious medications was significantly different from chance (χ2=21.03, df=4, P<0.001).
Neurological Investigations
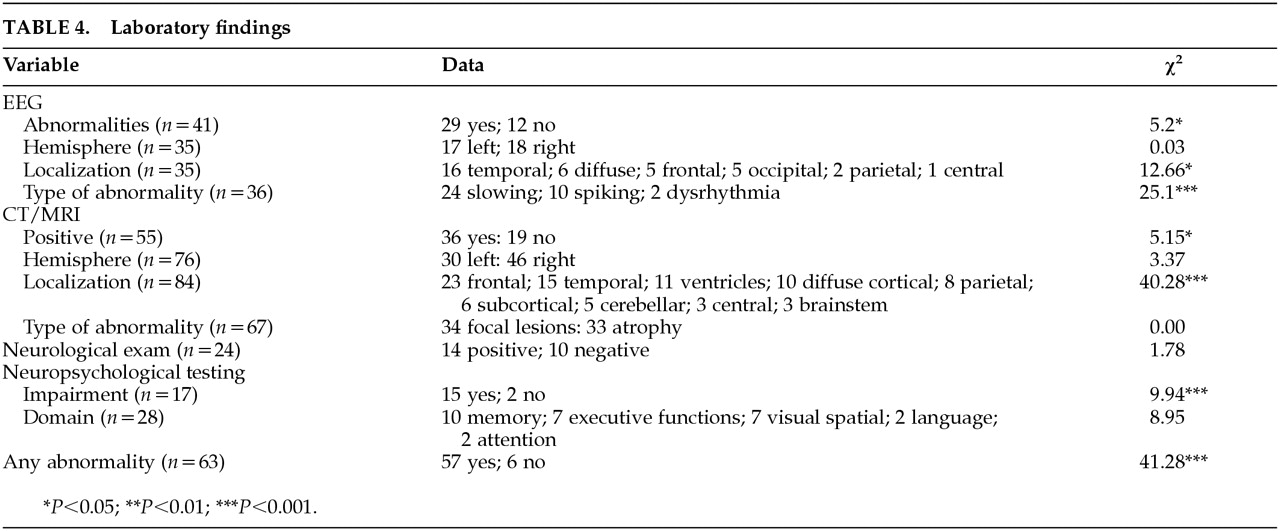
Data for neurological investigations are listed in
Table 4. EEG data were reported in 41 cases. Of these cases, 29 (about 70%) reported positive findings, which is significantly greater than chance (χ
2=5.2, df=1,
P<0.05). No differences were found in hemisphere location of EEG findings (left=17, right=18; χ
2=0.03, df=1,
P>0.10). Localization was as follows: 16 in the temporal areas, 5 frontal, 2 parietal, 5 occipital, 1 central, and 6 diffuse. The proportion of localized findings for specific cortical areas was greater than chance (χ
2=12.66, df=5,
P<0.05). In the cases that described the specific types of EEG abnormalities, 10 reported spiking, 24 slowing, and 2 dysrhythmia. The proportion of each abnormality type was greater than chance (χ
2=25.1, df=2,
P<0.001).
Data for CT and MRI were combined because both examine structural abnormalities. Of the 55 cases that included CT or MRI data, 36 reported positive findings, which is significantly greater than chance (χ2=5.15, df=1, P<0.05). A trend was found in hemisphere location of abnormalities (left=30, right=46; χ2=3.37, df=1, P<0.10). The frequency in localization of findings was as follows; 23 frontal, 15 temporal, 11 ventricular enlargement, 10 diffuse cortical, 8 parietal, 6 subcortical, 5 cerebellar, 3 central, and 3 brainstem. The proportion of localized findings was significantly greater than chance (χ2=40.28, df=9, P<0.001). In cases that described specific types of abnormalities, 34 reported focal lesions and 33 reported atrophy. No differences were found in type of lesion (χ2=0.00, df=1, P<0.10).
In 24 cases, either results from a neurological examination were reported or neurological symptoms were described. Of these cases, 14 reported positive findings, which was not different from chance (χ2=1.78, df=1, P>0.10). Neuropsychological test data were described in 17 cases, 15 of these reported impairments. The proportion of findings of impairment on neuropsychological test data was significantly greater than chance (χ2=9.94, df=1, P<0.001). Specific areas of impairment on neuropsychological test data were as follows: 10 memory, 7 executive functions, 7 visuospatial abilities, 2 language, and 2 attention. The proportion of impaired cognitive areas in comparison to each other approached significance when compared with chance (χ2=8.95, df=4, P<0.10).
Overall, when data from EEG, CT/MRI, neurological examination, and neuropsychological test data were combined, 57/63 or roughly 90% demonstrated at least one abnormality or impaired cognitive function. This proportion was significantly greater than chance (χ2=41.28, df=1, P<0.001).
Gender Differences
Gender differences in PDTBI were examined. There were trends for females to have sustained TBI at a later age than males (t=–1.81, df=58, P=0.10), and to have developed psychosis at a later age (t=–1.89, df=58, P=0.08). No differences were found for time of delayed onset in developing a psychosis (t=0.38, df=58, P=0.71) or for severity of TBI (χ2=0.37, df=1, P>0.05).
In terms of clinical presentation, no differences were found for proportion of seizure disorder (χ2=0.51, df=1, P>0.05), delusions (χ2=0.15, df=1, P>0.05), hallucinations (χ2=1.98, df=1, P>0.05), or negative symptoms (χ2=0.48, df=1, P>0.05). No differences were found on laboratory findings for EEG (χ2=1.22, df=1, P>0.05), CT/MRI (χ2=0.44, df=1, P>0.05), or neurological signs (χ2=0.01, df=1, P>0.05).
Delay in Onset of Psychotic Symptoms
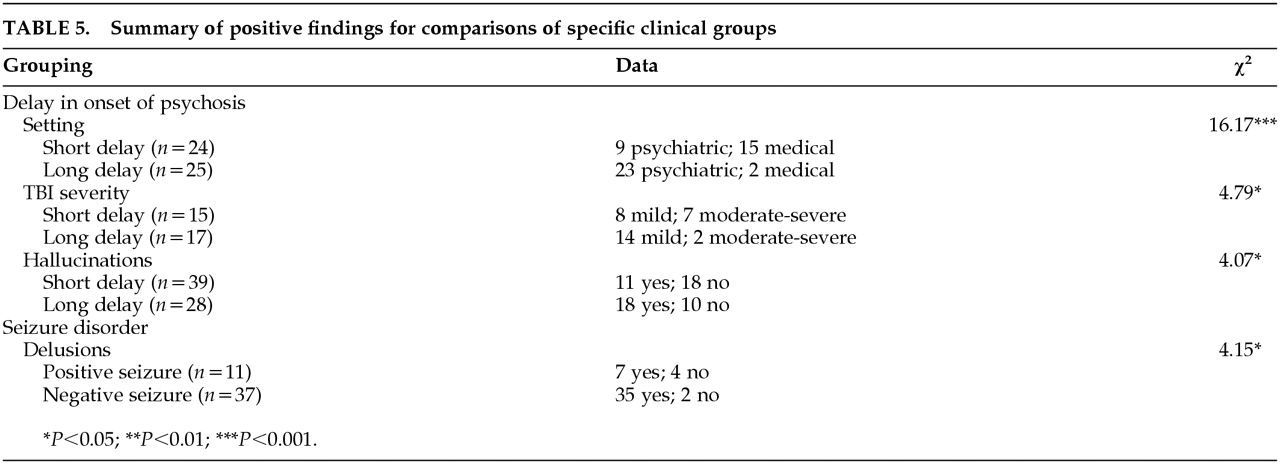
Comparisons were also made for patients with a short versus long delay in onset of psychotic symptoms. Patients were divided into two groups based on scores in relation to the median (1 year). Those with onset of symptoms 1 year and less after TBI were compared to those with onset of symptoms of more than 1 year. Results are presented in
Table 5.
Analyses reveal several significant differences between the groups. Differences were found in the setting at the time of evaluation, with the short-delay group having a higher proportion of inpatient medical versus psychiatry setting than the long-delay group (χ2=16.17, df=1, P<0.001). Significant differences were found for proportion of mild versus moderate/severe TBI, with the brief-delay group having more mild brain injury (χ2=4.79, df=1, P<0.05). The long-delay group showed a higher proportion of hallucinations than the short-delay group (χ2=4.07, df=1, P<0.05). By contrast, a trend was found for the short-delay group to show a higher proportion of visual hallucinations (χ2=3.78, df=1, P<0.10).
No significant differences were found for gender (χ2=0.11, df=1, P>0.10), clinical outcome (χ2=3.03, df=2, P>0.10), proportion demonstrating delusions (χ2=0.30, df=1, P>0.10), seizure disorder (χ2=0.94, df=1, P>0.10), negative symptoms (χ2=1.59, df=1, P>0.10), successful medications (χ2=3.47, df=3, P>0.10), positive EEG findings (χ2=0.31, df=1, P>0.10), EEG hemispheric localization (χ2=0.05, df=1, P>0.10), EEG lobe localization (χ2=7.12, df=4, P>0.10), CT/MRI positive findings (χ2=0.13, df=1, P>0.10), CT/MRI hemispheric localization (χ2=2.57, df=1, P>0.10), temporal lobe abnormalities (χ2=2.57, df=1, P>0.10), ventricular abnormalities (χ2=2.27, df=1, P>1.0), neurological signs (χ2=0.02, df=1, P>0.10), or neuropsychological testing (χ2=0.08, df=1, P>0.10).
Seizure Disorder
Specific analyses were also conducted for subjects with a diagnosis of seizure disorder versus those without a diagnosis. Data are presented in
Table 5. No differences were found in age at time of TBI (
t=0.35,
P>0.10), age at onset of psychosis (
t=0.56,
P>0.10), or delay in onset of psychosis (
t=0.52,
P>0.10). In terms of clinical presentation, there were no differences in proportion of subjects presenting with hallucinations (χ
2=1.88, df=1,
P>0.10); however, nonseizure patients demonstrated a significantly higher proportion of delusions (χ
2=4.15, df=1,
P>0.05). On laboratory tests, no differences were found in proportion of positive findings on EEG (χ
2=0.0, df=1,
P>0.10) or type of finding on EEG (χ
2=4.02, df=2,
P>0.05). No differences were found in proportion of positive CT/MRI findings (χ
2=0.45, df=1,
P>0.10).