T raumatic brain injury (TBI) is a major cause of disability,
1 with North American hospitalization rates of approximately 156/100,000 in older adults.
2 While severe traumatic brain injury in older adults is associated with high rates of mortality,
3 approximately 86% of traumatic brain injury in the elderly is of mild or moderate severity,
2 and most of these injuries do not lead to hospitalization. Little is known about the cognitive outcomes following this milder spectrum of traumatic brain injury severity in older adults. The few controlled prospective studies to date examining the consequences of mild-to-moderate traumatic brain injury sustained in older adulthood have shown impairments in memory
4 –
7 and executive dysfunction
4 –
6 compared with healthy controls. The largest controlled prospective study of cognitive outcome of traumatic brain injury occurring in old age, however, was of 35 subjects,
5 and the longest study was of average 3 months’ duration.
7 Traumatic brain injury has been investigated as a risk factor for eventual development of Alzheimer’s disease. The results have been contradictory and largely of a case-control nature, with traumatic brain injury in the remote past.
8 No studies to date have examined a potential relationship between late-life traumatic brain injury and dementia or mild cognitive impairment (a milder intermediate cognitive condition, predictive of dementia).
The present report is of a 2-year longitudinal study of cognitive outcome following traumatic brain injury in older adults. We have previously published the results of the cognitive and psychosocial outcome at 1 year postinjury,
9 and in that study we found that patients with TBI had worse performance than a matched control group on a broad spectrum of cognitive domains and they were rated by their close friends or relatives as having more impairment on instrumental activities of daily living (IADLs). In that report, however, follow-up was limited to 1 year and no data were available on the risk of clinically defined cognitive impairment or on the role of the Apolipoprotein E-ϵ4 (APOE-ϵ4) genotype.
APOE-ϵ4 has been linked to the development of Alzheimer’s disease in older adults.
10 The association of APOE with cognition following traumatic brain injury is equivocal in studies with younger adults: two studies linked APOE-ϵ4 with worse cognition in acute traumatic brain injury recovery,
11,
12 but four studies of outcome at or beyond 6 months after injury showed no relationship between APOE and cognition.
13 –
16 A traumatic brain injury cohort at greater risk of cognitive impairment by virtue of advanced age may demonstrate a more robust relationship between APOE and cognition.
The primary purpose of the present study is to investigate the impact that mild-to-moderate traumatic brain injury sustained in older adulthood and the APOE genotype have on cognition. We hypothesized that 2 years following injury, traumatic brain injury and APOE would be associated with cognitive and functional deficits, as well as an increased risk of clinically defined impairment, as indicated by the diagnosis of either dementia or mild cognitive impairment.
METHOD
Subject Selection
A consecutive sample of patients age 50 and over attending a traumatic brain injury clinic after attending an emergency room or trauma ward was assessed within 2 months of their injury and followed prospectively for 2 years. Subjects were admitted to the study if they met criteria for mild
17 or moderate traumatic brain injury.
18 Subjects who met criteria for mild traumatic brain injury but had an intracranial complication of traumatic brain injury (e.g., contusion) were categorized as having had a moderate traumatic brain injury.
18 We excluded subjects with preinjury history of neurological disease, serious acute medical illness, schizophrenia, bipolar disorder, or significant levels of alcohol consumption. Evidence of preexisting cognitive decline based on history or a cutoff of >3.38 on the Informant Questionnaire for Cognitive Decline in the Elderly (IQCODE)
19 was grounds for exclusion from the study.
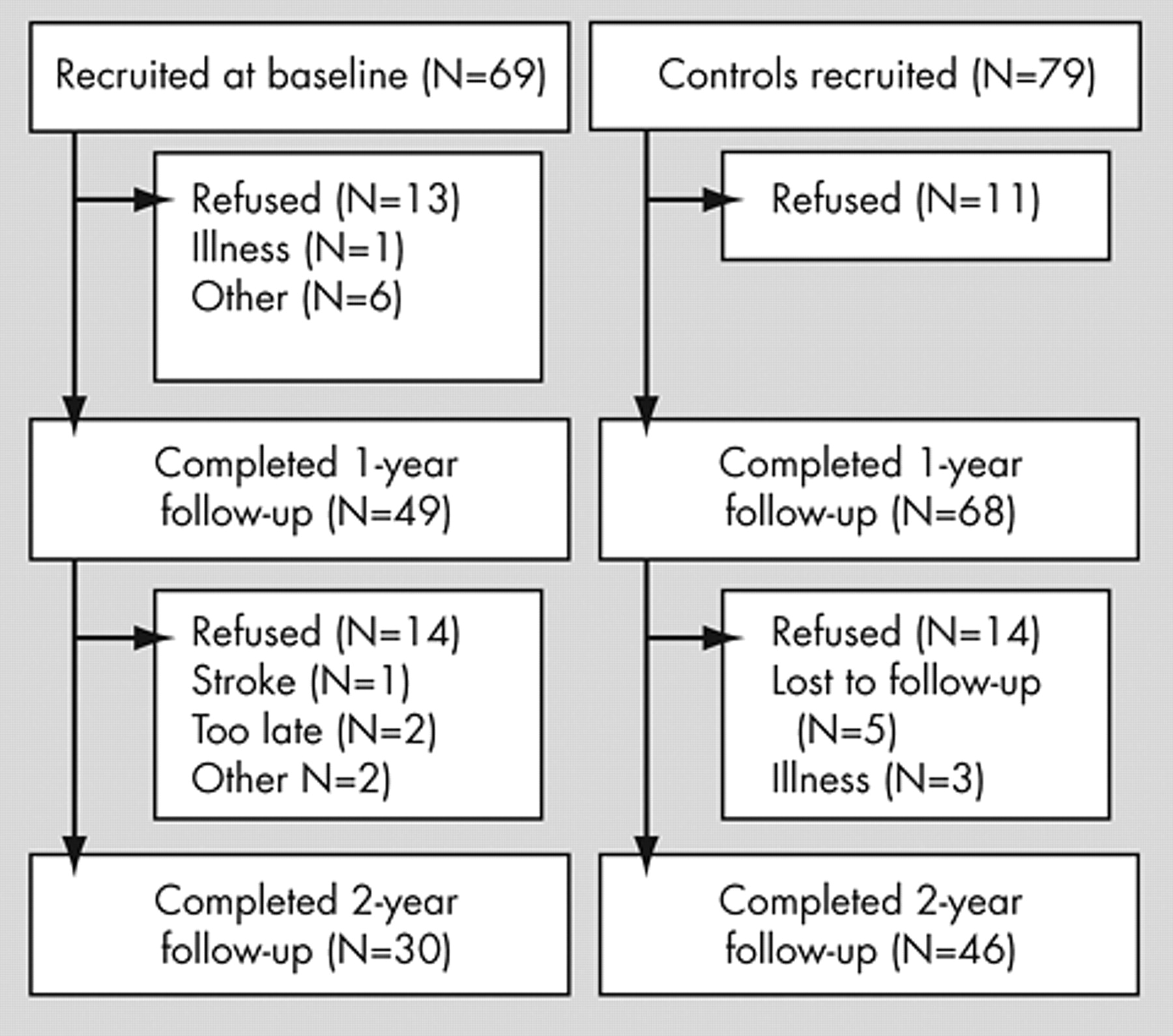
Figure 1 illustrates the subject selection process.
Cases were compared with a community control group recruited from newspaper advertisements. Each case was matched with one control (or more where available) by age decade, education group (i.e., less than 13 years of education or greater than or equal to 13 years of education), and gender. Exclusion criteria for controls were the same as those for cases. The IQCODE was conducted over the telephone for the controls.
The institutional ethics board approved the study and participants provided written informed consent.
Data Collection
Background information about patients and controls was collected at baseline through discussion with the subject and informant, as well as a chart review for the patients. Details of these variables collected are described in our previous publication.
9 Medical history was coded using the severity subscale of the Cumulative Illness Rating Scale (CIRS).
20Neuropsychological tests that demonstrate cognitive deficits consistent with traumatic brain injury and/or dementia were selected and administered 1 and 2 years after injury for the patients, and 1 and 2 years after the baseline visit for the controls. The battery of tests was made up of: The Mattis Dementia Rating Scale (DRS),
21 the Mini-Mental State Examination (MMSE),
22 the WAIS-III
23 digit span and digit symbol subtests, the logical memory total delayed recall of both stories from the Wechsler Memory Scale-III (WMS-III),
23 the long-delay free recall score of the California Verbal Learning Test (CVLT),
24 the delayed recall from the Rey-Osterrieth Complex Figure Test (RCFT),
25 the total score on the Boston Naming Test,
26 the Controlled Oral Word Association Test (COWAT)
26 and the Wisconsin Card Sorting Test (WCST) total categories completed and perseverative responses.
27 The WAIS-III vocabulary score
23 was used as an index of fluency in English to control for the confound of English as a Second Language, with those scoring less than the 14th percentile considered “nonfluent.”
Informant ratings of instrumental activities of daily living (IADLs) were provided using the Functional Activities Questionnaire (FAQ)
28 at 1 and 2 years after injury.
Subjects were classified as having “clinically significant cognitive impairment” (i.e., mild cognitive impairment or dementia) or not at the end of year one and year two. Mild cognitive impairment was defined according to Petersen’s criteria for amnestic mild cognitive impairment.
32While most of the studies to date exploring APOE and cognitive disorders have used Alzheimer’s disease as the outcome, the requirement of gradual onset and progression as well as the exclusion of other neurological causes made Alzheimer’s disease an inapplicable outcome for the present study. Dementia, for the present study, was defined according to DSM-IV criteria for dementia due to head trauma. Subjects were rated as having dementia, mild cognitive impairment or neither based on independent reviews of case and control medical charts, and of cognitive test results by three neuropsychiatrists at year one (MJR, AF, NH) and two neuropsychiatrists at year two (MJR, NH). Raters were blinded to case and control status of the subjects. Disagreements were resolved in consensus meetings.
The major depressive episode module of the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID)
29 was administered at baseline, and major depressive episode was treated as a confound for the present study.
The APOE genotype was determined for each subject at the 1-year evaluation. DNA was extracted from buccal epithelial cells using the Qiagen Mini Kit, and PCR amplified with primers specific for the APOE alleles ϵ2, ϵ3, and ϵ4. For present study analysis the variable of interest was the presence or absence of APOE-ϵ4 alleles.
Statistics
Demographic and past illness variables were compared between cases and controls. Analyses accounted for the matched nature of the cases and controls. For continuous variables, a repeated measures analysis of variance was used to compare the group differences. For categorical variables, a generalized linear model was used to compare the group differences. T tests and χ 2 tests were used to compare the background variables between subjects who dropped out of the study before 1 year with those who remained.
Analysis of covariance (ANCOVA), accounting for the matched nature of sample and repeated measures, was conducted to assess the role of traumatic brain injury, APOE, and the interaction of traumatic brain injury with APOE on the individual cognitive measures, controlling for age, gender, time, traumatic brain injury by time, education level, Cumulative Illness Rating Scale (CIRS) severity index, major depression, and fluency in English. For those ANCOVA models in which traumatic brain injury was found to be significant, a post-hoc reanalysis was conducted excluding subjects with English as a second language.
ANCOVA, accounting again for matching and repeated measures, was conducted for the Functional Activities Questionnaire, with the main effects of traumatic brain injury and APOE, and the interaction of traumatic brain injury with APOE, controlling for time and for traumatic brain injury x time, as well as age, gender, and baseline MMSE.
“Impairment,” as defined by either “mild cognitive impairment” or “dementia” by consensus, and the effects of traumatic brain injury, APOE and APOE x traumatic brain injury were assessed using a logistic regression analysis controlling for age, gender, education, major depression, and CIRS severity index.
In order to account for the effects of attrition, multiple imputation was used for the continuous models by creating several datasets with imputed values, running each through the statistical analysis, and combining the individual model estimates for a final model.
30RESULTS
Subjects
Sixty-nine cases with traumatic brain injury were included in the study at baseline (
Figure 1 ). Ninety-four controls were recruited through newspaper advertisements; 78 of these were matched to the subjects and included in the study. Three cases were unmatched and the analysis included all cases but treated the matched ones as correlated observations. The findings remained the same when the 3 unmatched cases were excluded. By the end of 1 year, 31 of the subjects had been lost to attrition, and 117 remained (85% overall; 71% of traumatic brain injury group). By the second year, 76 subjects remained, yielding an overall retention rate of 55.4% and 43.5% of the traumatic brain injury group (see
Figure 1 ). Subjects were seen for their follow-up assessments (mean of 46.4 days, SD=34) and had follow-up assessments on average at 13 months (mean of 393.2 days, SD=42) postinjury (or postbaseline for controls) and 25 months (mean 763 days, SD=37) postinjury. At the 1-year evaluation, cases were seen approximately 16 days later than controls (mean of 402.53 days [SD=57.3] versus mean of 386.47 days [SD=24.5],
F (1, 116)=4.27, p=0.0410), but there were no differences in time postinjury/baseline at the 2-year evaluation.
As reported previously,
9 in 37 cases of traumatic brain injury (53.6%), severity was mild. The remaining 32 subjects (46.4%) had moderate traumatic brain injury. There were no differences in severity or mechanism of injury, associated other injuries, or computerized tomography (CT) abnormalities between those who remained in the study at 2 years (N=30) and those who were lost to attrition (N=69).
Comparison of Background Variables
At baseline, the mean age of the cases was 67.00 (SD=7.9, range=50–89), and 68.04 (SD=8.5, range=51–89) for the controls (p=0.63). Men made up 47.8% and 48.1% of the cases and controls, respectively (p=0.71). The controls had approximately one and a half years more schooling than the cases (mean 14.07 [SD=3.0] versus mean 12.47 [SD=4.1], respectively;
F (1, 113)=6.00, p=0.016). As reported previously,
9 there were no differences between cases and the controls in background variables of marital status, prior traumatic brain injury, past or family psychiatric history, IQCODE or CIRS severity index scores. Fluency in English was present for 62.3% of the cases and 81.0% of the controls (χ
2 (1)=6.43, p=0.011). The APOE-ϵ4 allele was present in 28.9% (33/114) of the sample, with data missing on 3 subjects, but no differences in ϵ4 allelic prevalence between cases and controls.
Among those who remained in the study at 2 years, the control group had on average 2 years higher education than cases (mean 14.04 [SD=2.8] versus 12.14 [SD=4.4], respectively, F (1, 74)=5.73, p=0.024). Those who remained in the study at 2 years were more likely to have a positive family psychiatric history than those who dropped out of the study (40.8% versus 23.6%, χ 2 (1)=4.979, p=0.026), but there were no other differences in other background or traumatic brain injury variables.
Formal Cognitive Outcome
There were no significant differences between patients with traumatic brain injury and the control group on the general cognitive tests, tests of attention/processing speed, language, verbal or visual memory, or executive function. APOE genotype and its interaction with traumatic brain injury were not significant predictors of cognitive test performance.
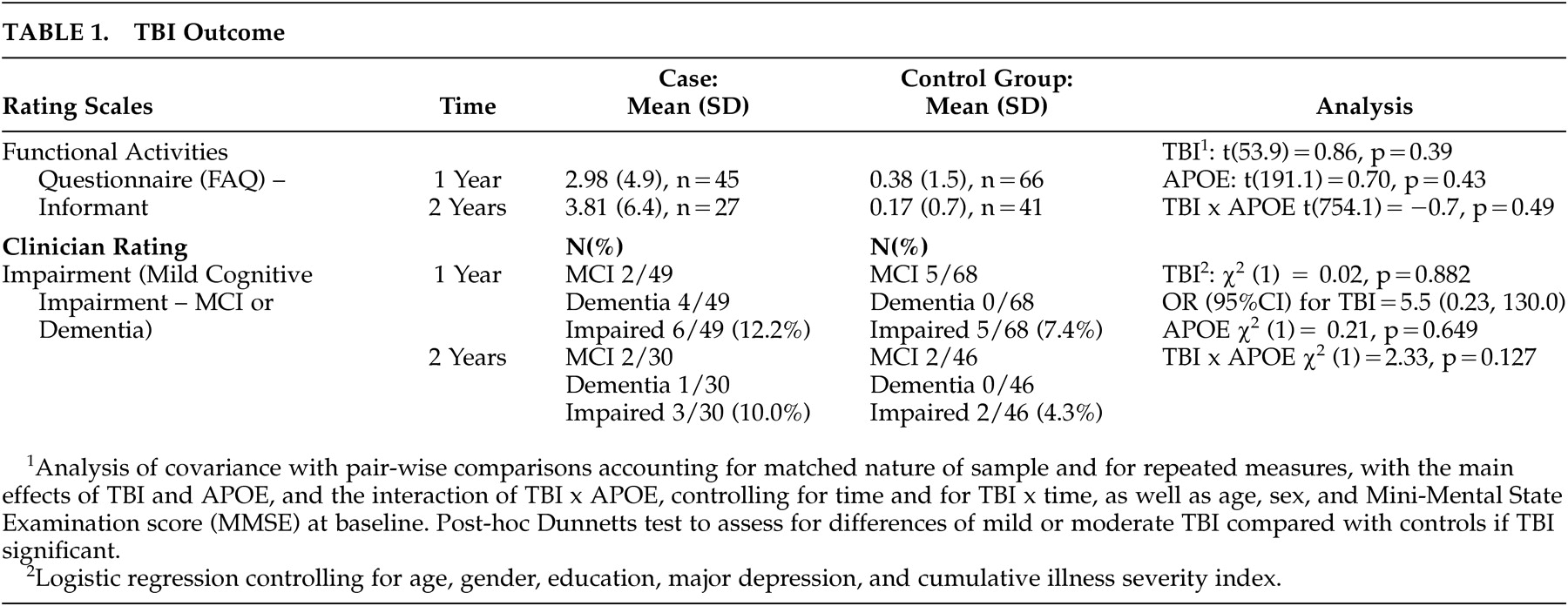
Informant and Clinician Ratings
Fifty-two percent of the patients’ informants and 39% of the controls’ informants were spouses. There were no differences in informant-rated disability between the traumatic brain injury and control group, and there was no significant effect of APOE (
Table 1 ). Traumatic brain injury, APOE, and their interaction did not predict the development of mild cognitive impairment or dementia in this group (
Table 1 ).
DISCUSSION
The present study found that in the 2 years following injury, patients with mild-to-moderate traumatic brain injury had no persisting cognitive or functional deficits, and there was no significantly greater conversion to the realms of mild cognitive impairment or dementia. Furthermore, APOE did not have an effect on cognitive outcome.
This is the first 2-year prospective study of cognitive outcome of traumatic brain injury sustained in older adulthood, and the strengths include exclusion of premorbidly impaired older adults, a detailed cognitive examination, and the matching of groups by age, gender, and education. An early report of a 21% rate of incident dementia following traumatic brain injury in older adults
31 was uncontrolled, subject to referral bias, and hence likely overestimated the frequency of clinically significant impairment. Unlike the previous shorter-term controlled studies of cognition following traumatic brain injury in older adults, the present study incorporated APOE testing and existing clinical definitions of impairment, as well as controlled for the potential confounding effects of medical illness and major depression.
The APOE-ϵ4 allele has been associated with poorer cognitive recovery in the first 2 months postinjury in two prospective studies of mild
12 and more severe traumatic brain injury,
11 whereas our finding of no relationship between measures of cognition and the APOE-ϵ4 allele is consistent with the three other prospective studies of traumatic brain injury and cognition 6 months postinjury.
13 –
15 In contrast, in a population study,
33 while no differences were found in post-traumatic brain injury cognitive performance between those with or without the ϵ4 allele, those with the allele had decreased performance from preinjury baseline using a pre-post design. The clinical nature of the sample in the present study precluded preinjury cognitive assessments. Age itself may be a factor in the relationship between APOE and traumatic brain injury outcome, as highlighted in a recent publication which showed a declining effect of APOE with advancing age.
34The present study is limited by the sample size and subject attrition. In order to detect a 10% difference in impairment between groups and maintain a power of 0.797 with alpha of 0.05, we would have needed 125 subjects in the study, and since we found less than a 10% difference between the groups, even more subjects would be needed. Attrition poses a significant bias in prospective longitudinal studies of traumatic brain injury, but the retention rate in the present study is comparable to other 2-year traumatic brain injury datasets in younger adults,
35 and the use of multiple imputation to adjust for attrition in the present study was an attempt to address this concern. Although selective recruitment of subjects without premorbid impairment, acute medical illness, or excessive alcohol intake limits the generalization of the present study to the mild-to-moderate traumatic brain injury in the community, the careful exclusion of these factors and control for confounding variables in the present study allows for greater confidence in the finding of relative executive and IADL difficulties.
Because of the high incidence of traumatic brain injury in the elderly, its associated morbidity, and its status as a potential risk factor for dementia, further studies should be considered exploring the longer-term cognitive effects of traumatic brain injury among older adults, using a broader variety of tests of frontal-subcortical dysfunction, and imaging measures to further delineate the underlying pathophysiology of those with persisting deficits.
Acknowledgments
Preliminary data from this investigation was presented at the American Neuropsychiatric Association Annual Meeting, March 1, 2005, Bal Harbor, Florida, and at the American Psychiatric Association Annual Meeting, May 20-25, 2006, Toronto, Canada. This work was supported by the Ontario Neurotrauma Foundation.