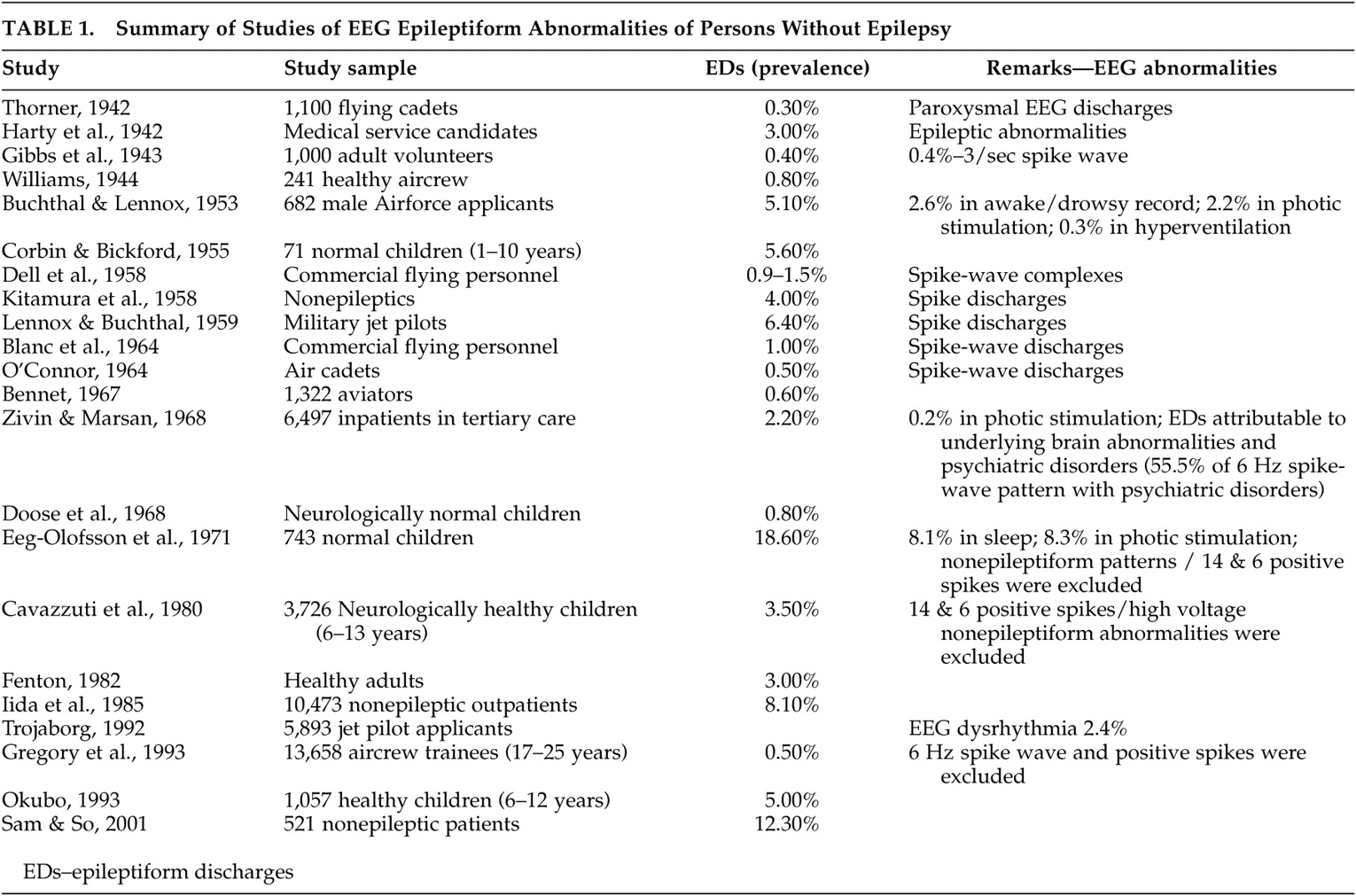
EEG Dysrhythmia in the Nonepileptic Population
Twenty-two papers were identified. Epileptiform discharges (EDs) ranged from 0.8% to 18.6% in reportedly normal children and 0.3% to 12.3% in reportedly normal adults. These studies have been summarized in
Table 1 .
Several of these investigations had attempted to determine the prevalence of such epileptiform discharges in large “healthy” nonepileptic populations. In this regard, several publications have reported a wide range of prevalence of varying EEG dysrhythmia, some of which were in disagreement, in nonepileptic and purported normal populations. The results of such studies, unfortunately, therefore depicted conflicting EEG findings within the “healthy” nonepileptic populations.
It can be seen from
Table 1 that there were studies with relatively low rates of epileptiform discharges, and on the contrary, several studies did document a high prevalence of epileptiform discharges. The low estimates, as in the studies of Gibbs et al. (0.4%)
5 and Bennet (0.6%),
6 employed minimum EEG requirements, where only three head regions were examined, without a sleep record, and for a limited duration of 10–15 minutes. Bennett’s study focused only on spike-wave abnormalities and excluded all other epileptiform discharges. Eeg-Olofsson et al.
7 reported a high prevalence of epileptiform discharges but they considered all the EEG dysrhythmia in children during wakefulness, in addition to studies during sleep, photic stimulation, and hyperventilation, and they included non-epileptiform activities as well.
In other studies, factors that were incriminated in high prevalence estimates were the inclusion of individuals with psychiatric histories and/or history of significant head trauma. For instance, in a series of 6,497 nonepileptic subjects, Zivin and Marsan
8 had reported the prevalence of epileptiform discharges to be 2.2% when careful definitions of epileptiform discharges had been used with optimum recording standards. In this nonepileptic group, epileptiform discharges were attributable to underlying brain abnormalities (traumatic, vascular, tumor, metabolic), medications, and psychiatric disorders. The prevalence of epileptiform discharges in these groups was reported as 5.5% in those with mental handicap, 9.8% with congenital or perinatal brain insults, 10.6% after cranial operations, and 8.2% in individuals with cerebral tumors.
A similar conclusion was derived from a study of patients without epilepsy in the community. In this study, the prevalence of epileptiform discharges was reported as 12.3%, but 73.4% of the nonepileptic patients had underlying cerebral disorders.
9 This emphasized that the presence of epileptiform discharges in subjects without epilepsy should be inferred as “electrographic markers” of underlying brain dysfunction without the vulnerability to clinical seizures. These abnormal neuronal discharges, most closely associated with seizures, do occur in people who do not have epilepsy (subclinical epileptiform discharges), but most have been linked to underlying cerebral disorder.
After exclusion of contaminating factors, the true prevalence of epileptiform discharges in the healthy normal population should be extremely low. The current estimate of EEG epileptiform dysrhythmia in the nonepileptic healthy population should be less than 1%, as supported by the work of Gregory et al.
10Struve
11 reported the prevalence of EEG abnormalities in the nonepileptic “normal” adult population ranging from 4% to as high as 57.5%. This wide range reflected the lack of rigorous selection criteria for choosing the normal healthy control comparison subjects. A study by Boutros et al.
12 emphasized the priority for clearly defining the boundaries of the normative EEG, which is critical in deriving valid generalizations for consensus opinion on the electroencephalographic correlates of neuropsychiatric disorders. They proposed a seven point normality criteria for selecting healthy comparison subjects. Their search of the relevant published literature on selection methodology for “normal” comparison subjects from 1936 to 2005 included 38 articles. The majority of included studies did not fulfill any of their specified normality criteria. The study confirmed the inadequate definition for EEG normality, and also reiterated the fact that the literature concerning the prevalence or significance of EEG correlates in neuropsychiatry remains preliminary after all these years.
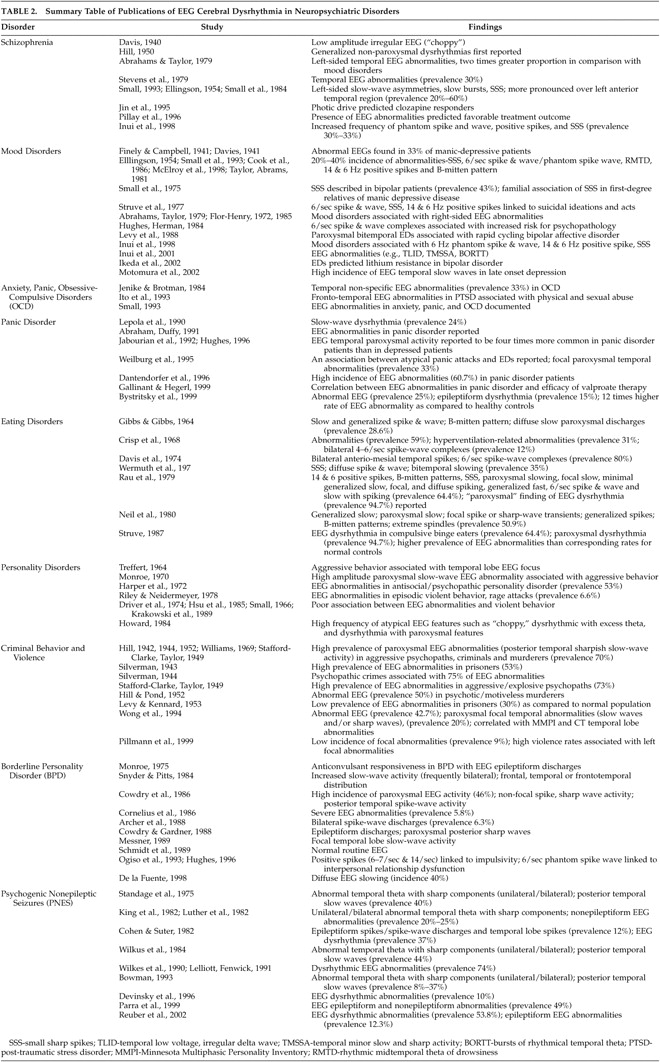
EEG Dysrhythmia in Neuropsychiatric Disorders
Sixty-three papers were identified. Ten papers examined the conventional EEG in schizophrenia populations (
Table 2 ). Eight of the 10 papers reported varying degrees of abnormalities and two papers reported that such deviations may be related to treatment responses. Eighteen papers were related to mood disorders and reported varying degrees of abnormalities. Eleven papers addressed anxiety disorders (including panic attacks), seven addressed eating disorders, 20 addressed personality disorders (11 of those on borderline personality disorder), 12 papers addressed criminal behavior and violence, and 11 papers examined the EEGs of patients with psychogenic nonepileptic seizures. The overwhelming majority of papers reported varying degrees of abnormalities (
Table 2 ).
During the last six decades there has been a large amount of literature on electroencephalographic abnormalities in a high proportion of psychiatric patients. No comprehensive review of this large body of psychiatrically relevant literature has been critically presented. Our extensive search of publications on the EEG correlates of psychopathology is summarized in
Table 2 . The published work of Kennard
13 reviewed two decades of pioneering literature affirming the positive correlations of abnormal EEGs in psychological disorders. This section, even after six decades of psychiatric EEG research, attempts to dissect the same behavioral/EEG equation as it applies to our current state of EEG understanding and evidence-based research methodology.
About two decades earlier, the work of Bridgers
14 again confirmed the occurrence of epileptiform dysrhythmic abnormalities in a population of nonepileptic hospitalized psychiatric patients. The EEG findings were found to correlate with conditions such as anorexia nervosa, depression, mania, personality disorders, suicidality without depression, schizophrenia, nonpsychotic explosive behavior, and the effects of psychotropic medications. The epileptiform EEG abnormalities were documented in 2.6%, and consisted of photoparoxysmal responses, focal temporal complexes, generalized spike-wave or polyspike-wave discharges, and focal central/frontal complexes. This study did emphasize that EEG epileptiform dysrhythmia does occur in nonepileptic psychiatric populations and may reflect underlying cerebral dysfunction without necessarily indicating an increased liability to seizures.
Numerous studies have documented conventional EEG abnormalities in 20%–60% of patients with schizophrenia, and have been summarized in
Table 2 . Abrahams and Taylor
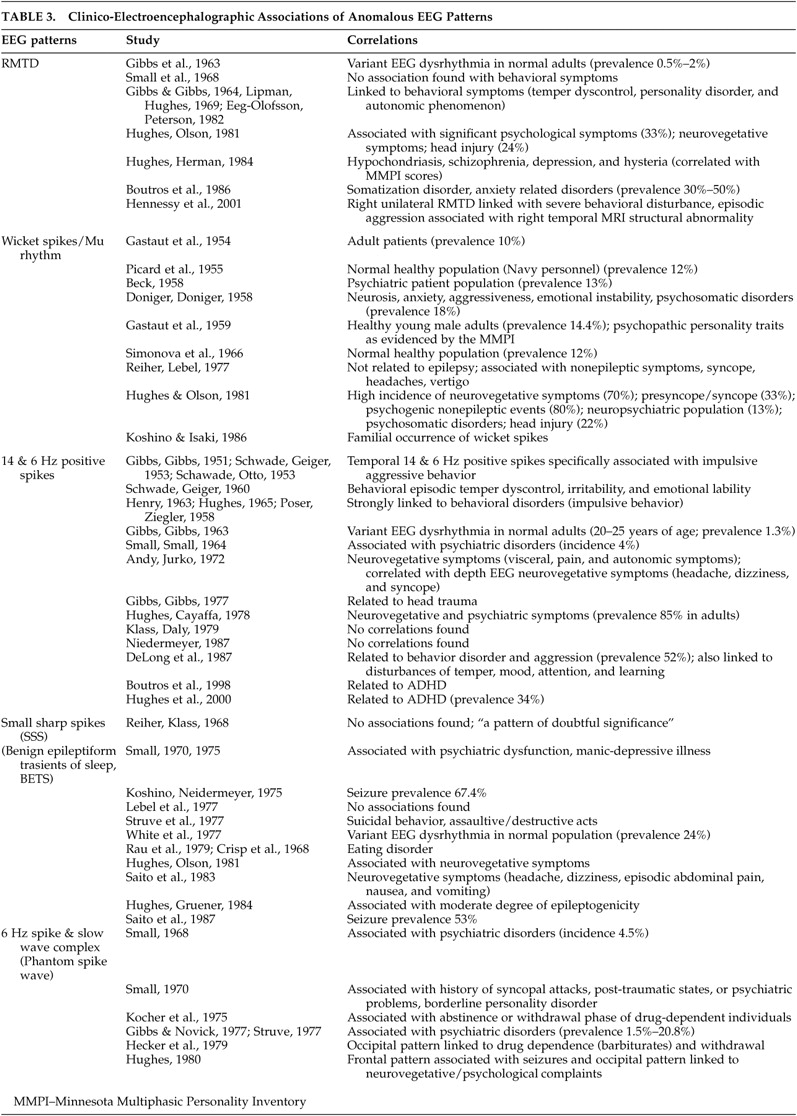
15 showed that schizophrenic patients had twice as many left-sided temporal abnormalities than patients with affective disorders who had more right-sided EEG findings. Definite EEG abnormalities have been documented in a high proportion of schizophrenia patients, but perhaps were minor, quite nonspecific, and conjectural. EEG abnormalities were more frequent in the cohort of schizophrenic patients who had a positive family history suggesting that genetic factors may be contributing to EEG traits. The EEG aberrations possibly reflected abnormalities in cortical neuronal architecture, cellular neuropathology, and neurochemical transmitter abnormalities that underpin the schizophrenia pathophysiology, in addition to possible neuroleptic medication effects. These EEG aberrations, along with neuroimaging and neuropsychological abnormalities, lend objective evidence for brain dysfunction in the genesis of schizophrenia. Furthermore, specific differences have also been reported among subgroups of functional mental illness. Psychotic mood disorders and “atypical” psychoses are reported to have a higher frequency of epileptiform variants, including the phantom spike and wave, positive spikes, and small sharp spikes, as compared with nonpsychotic mood disorders and schizophrenia.
16Many previous EEG findings in individuals with personality disorders, violent and criminal behavior, and forensic populations have been found to suffer from methodological problems. The EEG data were thus considered nonspecific as the results could not always be replicated by all investigators. Therefore, the significance of these EEG abnormalities is still a matter of debate. Abnormal EEG findings reported in association with personality disorders, criminal behavior, and borderline personality disorder are summarized in
Table 2 . One of the interesting findings in earlier studies was that relatively good personality structure relates to a normal EEG.
17 The initial studies did reveal positive trends in relating EEG dysrhythmic abnormalities to personality traits, and a psychopathic MMPI profile.
17 –
19 These EEG aberrations noted in personality disorders and impulsive behaviors reflect the presence of cerebral dysfunction that may hamper the natural process of psychological maturation.
Hill and Watterson
18 were the first to postulate that EEG dysrhythmia in aggressive psychopaths reflected a failure in functional cortical development (maturational retardation hypothesis). Although some evidence supports the maturational retardation hypothesis,
20,
21 the finding that many aggressive psychopaths had normal EEGs argued against it. Other studies, however, failed to find a relationship between EEG abnormalities and aggressive tendencies.
22 –
25 Ribas et al.,
26 on the other hand, found evidence of cerebral dysrhythmia in 69% of youngsters with behavior disorders with a predominance of aggressiveness. Earlier literature did link criminal behavior and aggression to an “epileptic etiology.” However, there is lack of convincing current evidence for such a proposition of an association between violence and epileptiform EEG disturbances.
27Studies of antisocial and criminal populations have revealed EEG abnormalities in 24%–78% of individuals. These EEG abnormalities were found to be more prevalent in subjects with violent crimes, repeated violence, and motiveless crimes. No specific relationship had been found between the type of EEG abnormality and characteristics of the crime, or between EEG changes and the degree of violence committed.
28,
29 Several types of EEG abnormalities have been found in violent offenders: generalized slowing, focal slowing, and epileptiform discharges. A few studies summarized in
Table 2 had established violent behavior to be linked to left-sided temporal lateralization of EEG abnormalities.
28,
30 These EEG aberrations suggested an underlying brain dysfunction in violent behavior.
31 The validity of these EEG aberrations has also been confirmed by quantitative EEG
32 and neuropsychological data.
33 These studies lend support to the concept of a connection between left hemispheric (frontal, temporal) cerebral dysfunction and the propensity for violence. However, the presence of EEG dysrhythmia, instead of having any specific associations with criminal behavior, may actually represent underlying comorbid factors such as multiple head injuries, coexisting substance abuse, and associated toxic and metabolic disorders, although a laterality effect would not be expected.
In borderline personality disorder (BPD), the literature suggests two types of conventional EEG abnormalities: epileptiform dysrhythmia and diffuse EEG slowing. The presence of epileptiform discharges in bipolar disorder possibly indicates cortical excitability disturbances that may be predictive of responsiveness to anticonvulsant therapy,
29 whereas diffuse EEG slowing possibly reflects underlying metabolic or degenerative etiologies. Boutros et al.
34 reviewed the literature from 1966 to 2000 on the electrophysiological aberrations in bipolar disorder. It was found that the EEG investigations of bipolar disorder were limited, as only nine articles could be retrieved. Furthermore, the majority did not have adequate control groups or adequate evaluation of Axis I or Axis II comorbidity and controls for medication effects.
Anorexia nervosa and other eating disorders have also been documented to have a higher prevalence of EEG dysrhythmia. EEG abnormalities documented include 14 and 6 positive spikes, B-mitten patterns, small sharp spikes, paroxysmal slowing, focal slowing, minimal generalized slowing, focal & diffuse spiking, generalized fast, 6/sec spike and wave and slow with spiking. The co-occurrence of EEG abnormalities consisting of B-mitten and small sharp spike (SSS) dysrhythmic patterns may reflect the cross relationships between anorexia nervosa, depressive disorder, and suicidality. These are possibly related to dietary factors, neuroendocrine, and nutritional deficiencies that would undoubtedly cause cerebral metabolic aberrations contributing to brain dysfunction.
As seen in
Table 2, several studies have suggested a high incidence of EEG abnormalities in patients with anxiety disorders, panic disorders, and obsessive-compulsive disorders. Hughes
35 reported that EEG paroxysmal dysrhythmia was four times more common in panic patients than in depressed patients. Our literature review indicated that about 25%–30% of panic attack patients had demonstrable EEG abnormalities, especially in atypical presentations of panic attacks. Some studies have documented an epileptic pathophysiology to underlie atypical panic attacks.
36Our literature review (
Table 2 ) suggests that the incidence of abnormal EEG findings in mood disorders is substantial, ranging from 20%–40%.
37,
38,
39 –
41 These abnormalities were found to be higher in manic patients than in depressed patients, in female than in male bipolar patients, and in nonfamilial cases with late-age onset disorder. Specific patterns noted in mood-disorders include the small sharp spikes (SSS), 6/sec spike and wave complexes (RMTD), B-mitten pattern, and positive spikes. Abrahams and Taylor
15 and Flor-Henry
42,
43 reported that mood disorders particularly showed more right-sided EEG abnormalities, in contrast to the left temporal EEG abnormalities in schizophrenia. Further, a few reports have demonstrated that rapid cycling bipolar affective disorder patients had more prevalent EEG evidence of bitemporal epileptiform paroxysmal activities than patients with nonrapid cycling mood disorders.
44Head injury with post-concussion syndromes may have a high incidence of underlying diffuse axonal injury and have been documented to be associated with abnormal EEGs, even in the presence of normal neurological examinations.
45 Thus, as pointed out earlier in the section ”EEG Dysrythmia in the Nonepileptic Population,“ head injury should form an exclusion criterion in the selection of healthy comparison groups in neuropsychiatric research.
Psychogenic nonepileptic seizure (PNES) is another area in the psychiatric EEG literature that merits a reappraisal. In our review of the literature, the only study that specifically focused on the prevalence of interictal EEG abnormalities in psychogenic nonepileptic seizures was that of Reuber et al.
46 Other studies related to psychogenic nonepileptic seizures have been summarized in
Table 2, and relevant data extracted from these articles pointed to a mean prevalence of interictal EEG abnormalities in psychogenic nonepileptic seizures to be estimated at 25.9%.
47 –
55 In Reuber’s study, the rates of abnormal, non-specific, and epileptiform EEG abnormalities in psychogenic nonepileptic seizures were documented to be 53.8% and 12.3%, respectively. When psychogenic nonepileptic seizures were compared with an appropriately selected control group, nonspecific EEG abnormalities were seen 1.8 times as often in psychogenic nonepileptic seizures as in healthy controls. Such EEG abnormalities may be attributed to the complex interaction of comorbid psychiatric disorders and various psychopathological variables, underlying brain abnormalities, head trauma,
56 –
58 and physical and sexual abuse, which plays a pivotal role in the final clinical expression of psychogenic nonepileptic seizure vulnerability. It is imperative to be cognizant of the fact that EEG dysrhythmias do occur in psychogenic nonepileptic seizures, and it is crucial to understand that the mere presence of paroxysmal EEG dysrhythmia in psychogenic nonepileptic seizures should not lead to an epileptic connotation.
Early childhood sexual abuse, early stress, and lifetime assaultive violence have been linked to cortical maldevelopment and increased electrophysiological abnormalities. Several studies reported that such severe early stress and abuse have the potential to alter brain development and cause limbic dysfunction during specific sensitive periods of cortical maturation.
59 The cascade of events is mediated through stress-induced neurohormones of the glucocorticoid, noradrenergic, and vasopressin-oxytocin stress response systems which affects neurogenesis, synaptic overproduction and pruning, and myelination. The aberrant cortical development has been reported to involve the corpus callosum,
60 left neocortex, hippocampus, and amygdala. During the last decade, studies have reported an emergence of EEG abnormalities in children with sexual and psychological abuse. An increased prevalence of fronto-temporal electrophysiological abnormalities with a left-sided localization was reported in abused children.
61 –
63 Another study reported dysrhythmic EEG abnormalities in 77% (N=22) of patients who were involved as the child or younger member in an incestuous relationship, of which 36% had clinical seizures.
64 These studies thus provide evidence for the neurobiological underpinnings through which early abuse increases the risk of developing various psychopathologies and its electrophysiological consequences.
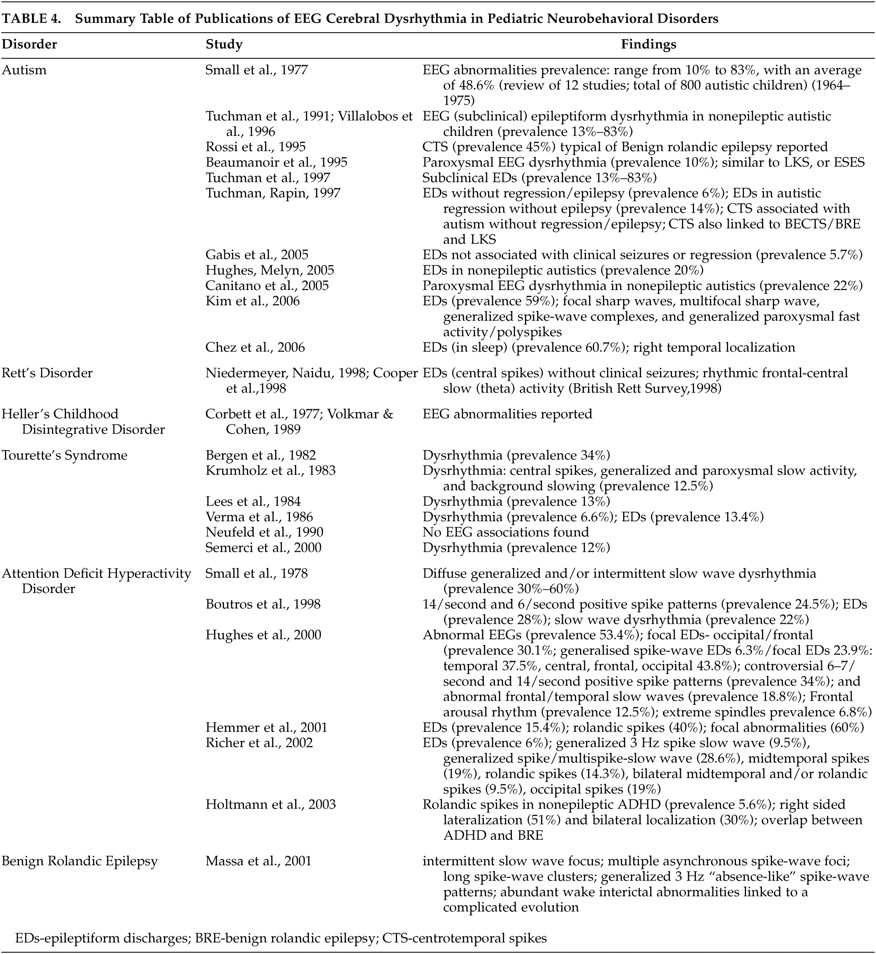
EEG Dysrhythmia in Pediatric Neurobehavioral Disorders
Twelve papers were identified addressing autistic spectrum disorders. All papers reported increased prevalence of EEG abnormalities ranging from 5.7%–60.7% (
Table 4 ). Five of the six papers examining the EEGs of patients with Gilles de la Tourette syndrome reported abnormal EEGs, as well as the six papers investigating attention deficit hyperactivity disorder (ADHD).
Two of the common neurobehavioral disorders of childhood are autistic spectrum disorders (autism, pervasive developmental disorder not otherwise specified, Asperger’s syndrome, Rett’s syndrome, and disintegrative disorder) and attention deficit disorders with or without hyperactivity (ADHD or attention deficit disorder). Autistic spectrum disorders, Landau-Kleffner syndrome, electrical status in slow wave sleep, developmental dysphasia, and benign rolandic epilepsy have overlapping features, and from our review, the high incidence of epilepsy and/or subclinical or infraclinical epileptiform EEG dysrhythmia does seem to be the interesting common thread that exists among these conditions. The studies that have linked the various pediatric neurobehavioral disorders without overt clinical seizures to EEG abnormalities have been summarized in
Table 4 .
The earliest review of studies on autism was contributed by Small et al.
65 who, from 14 pooled studies, reported a wide range of prevalence of EEG dysrhythmia. This large range undoubtedly arose from differences both in the populations under study and, more importantly, the diagnostic criteria used for the abnormality. Kim et al.
66 reported 59% prevalence of interictal epileptiform EEG abnormalities that included focal sharp waves, multifocal sharp waves, generalized spike-wave complexes, and generalized paroxysmal fast activity/polyspikes in nonepileptic autistic children. These EEG dysrhythmias probably represent an age-dependent epiphenomenon of impaired brain maturation, with cumulative effects of these EEG discharges contributing to cognitive abnormalities.
Several studies summarized in
Table 4 have documented positive correlations between subclinical paroxysmal EEG dysrhythmia in nonepileptic autism
67 –
74 and nonepileptic ADHD,
75 –
78 and have also brought to light the clinical overlap between nonepileptic ADHD and typical benign rolandic epilepsy as evidenced by the increased frequency of EEG subclinical rolandic spikes in these nonepileptic groups.
79The electrographic dysrhythmia in these pediatric neurobehavioral disorders may represent an epiphenomenon of cerebral dysfunction or underlying cortical morpho-functional abnormalities, and/or reflect a brain neurophysiological disorder which is not sufficient to be expressed as epilepsy. This may be due to the lack of properly functioning corticocortical fibers which restricts the spread of epileptiform activity from one brain area to another and prevents its evolution to a clinical seizure. The “subclinical epileptogenesis” in the developing brain may also directly impair cognitive behavior functioning by way of “transient cognitive impairment” mechanisms, well described by Binnie and his colleagues.
80 –
82 A complicated evolution in benign rolandic epilepsy had been reported to occur in a proportion of benign rolandic epilepsy patients. This benign rolandic epilepsy subset developed behavioral, cognitive, and learning problems independent of their clinical seizures or treatment. The complicated evolutions were found to be correlated with certain interictal EEG variables: intermittent slow-wave focus, multiple asynchronous spike-wave foci, long spike-wave clusters, and generalized 3 Hz “absence-like” spike-wave discharges.
83 Complicated benign rolandic epilepsy does further implicate the role of subclinical interictal EEG discharges in the etiology of behavioral and cognitive problems unrelated to any seizure characteristics.
The studies summarized in
Table 4 put forward arguments for an association between subclinical epileptiform discharges and neurobehavioral disorders as well as about causality. Given the established link between EEG epileptiform abnormalities and neuropsychiatric symptoms in these overlapping disorders, EEG evaluation seems to be justified in children with cognitive and behavioral problems, even in the absence of overt clinical seizures. In this context, Engler et al.
84 showed beneficial effects of sulthiame on EEG features, neuropsychological deficits, and speech deficits in seizure-free children with rolandic spikes. Duane et al.
85 reported similar findings in their study demonstrating beneficial effects on cognitive, behavioral, and EEG indices using levetiracetam in those with learning and attention problems. In a recent study, Chez et al.
74 reported a frequency of 60.7% abnormal EEG epileptiform activity in autism spectrum disorder patients with no known genetic conditions, brain malformations, prior medications, or clinical seizures. In the valproate treated group, 45% normalized on EEG and about 20% showed EEG improvement when compared with the first EEG.
At the end of this section, we opine that the maxim “treat the patient, not the EEG” may perhaps be an oversimplified clinical standpoint as evidence is mounting that some of the disorders reviewed (autism spectrum disorder, ADHD associated with subclinical rolandic epileptiform EEG discharges) with coincident subclinical epileptiform discharges might benefit from antiepileptic therapy even in the absence of overt clinical seizures.
86,
87