I n a recent paper,
1 we present extensive data and argue that although many authors
2 –
6 have associated the right hemisphere with a negative hemispheric emotional valence, many individuals have a left negative hemispheric emotional valence as a trait. We believe that knowing whether an individual’s hemispheric emotional valence is left or right negative could guide lateralized therapies such as rapid transcranial magnetic stimulation (rTMS). Lateral visual field stimulation, as described in detail below, is a simple, convenient, inexpensive method for determining hemispheric emotional valence, which correlated highly with probe auditory evoked potentials,
1 a technique that has been used
7,
8 for the determination of the direction of an individual’s hemispheric emotional valence. Our hypothesis is that activation, with rTMS, of a hemisphere with a positive hemispheric emotional valence should lead to improvement, but activation of a hemisphere with a negative hemispheric emotional valence should not.
Schiffer et al.
9 reported that affective responses to baseline lateral visual field stimulation predicted the clinical responses to a 2-week course of rTMS in 37 patients with a history of chronic major depression. In essence, the authors predicted that patients with a positive left hemispheric emotional valence by lateral visual field stimulation would do well with a treatment that stimulated the left hemisphere and that patients with a negative left hemispheric emotional valence by lateral visual field stimulation would do poorly with this treatment. In that study, the results showed that among 20 patients predicted to do well, the mean reduction in their Hamilton Depression Rating Scale (HAM-D) scores from baseline to 2 weeks posttreatment was 42%, while those 15 patients predicted to do poorly had only an 11% improvement. Seventy-five percent of those predicted to do well had greater than a 20% improvement in their HAM-D scores at 2 weeks posttreatment, and 80% of those predicted to do poorly had less than a 20% improvement.
In the present study, we attempted to replicate Schiffer’s rTMS findings.
9 Based on work by Wittling and colleagues
10,
11 that reported subjects’ differential physiological and emotional responses to videos shown to one visual field versus the other, Schiffer
12 found in a placebo-controlled study that 60% of 70 patients in a psychotherapy practice reported at least a 20% difference on a simple anxiety measure between sides. As Wittling and Schweiger
11 reported, Schiffer found that the side that evoked more anxiety varied among subjects. EEG, ear temperature,
13 and fMRI studies
14 indicated that lateral visual field stimulation activated the contralateral hemisphere. Thus, the combination of lateralized affective and physiological responses suggest that this technique may reveal something about the laterality of emotional processing in an individual subject that may influence his or her response to a lateralized treatment for depression.
In our 2002 report,
9 we showed a scatter plot that identified male and female subjects, but we did not report gender differences because we felt our sample was too small. In a reevaluation of that data, the 2-tailed Pearson’s correlation for men (N=11) between the measures of depression in response to lateral visual field stimulation and HAM-D percent change at 2 weeks posttreatment was strong (r=0.84, p=0.0011), whereas for women (N=26) it was weaker (r=0.26, p=0.19, nsec). In the present study, we sought to replicate the general finding that lateral visual field stimulation predicted responses to left-sided rTMS as well as to ascertain if these gender differences in predictive response held in an independent sample.
The procedures were performed at MindCare Centres, Vancouver, British Columbia, Canada, a clinic that specializes in the treatment of depression with rTMS. In a chart review study, we evaluated data from 23 consecutive patients who were treated at the clinic for depression with left-sided rTMS. Prior to the evaluation or treatment, each patient was offered an explanation of the procedures and asked to give signed informed consent. Twelve subjects (six women) were diagnosed with major depression based on the Structured Clinical Interview for DSM-III-R.
15 Four subjects (three women) were diagnosed with major depression and a generalized anxiety disorder, and four subjects (three women) were diagnosed with dysthymic disorder. Two women were diagnosed with bipolar affective disorder II and one man with bipolar affective disorder I. Two patients (one woman) were left-handed and the mean age of the 14 women was 51 years (SD=9). For the nine men the mean age was 51 (SD=18). All patients were screened for contraindications to rTMS therapy, such as a history of a seizure disorder or ferromagnetic material in the cranium. Each patient filled out a Beck Depression Inventory (BDI)
16 prior to rTMS and at discharge from the clinic 2 weeks later.
RESULTS
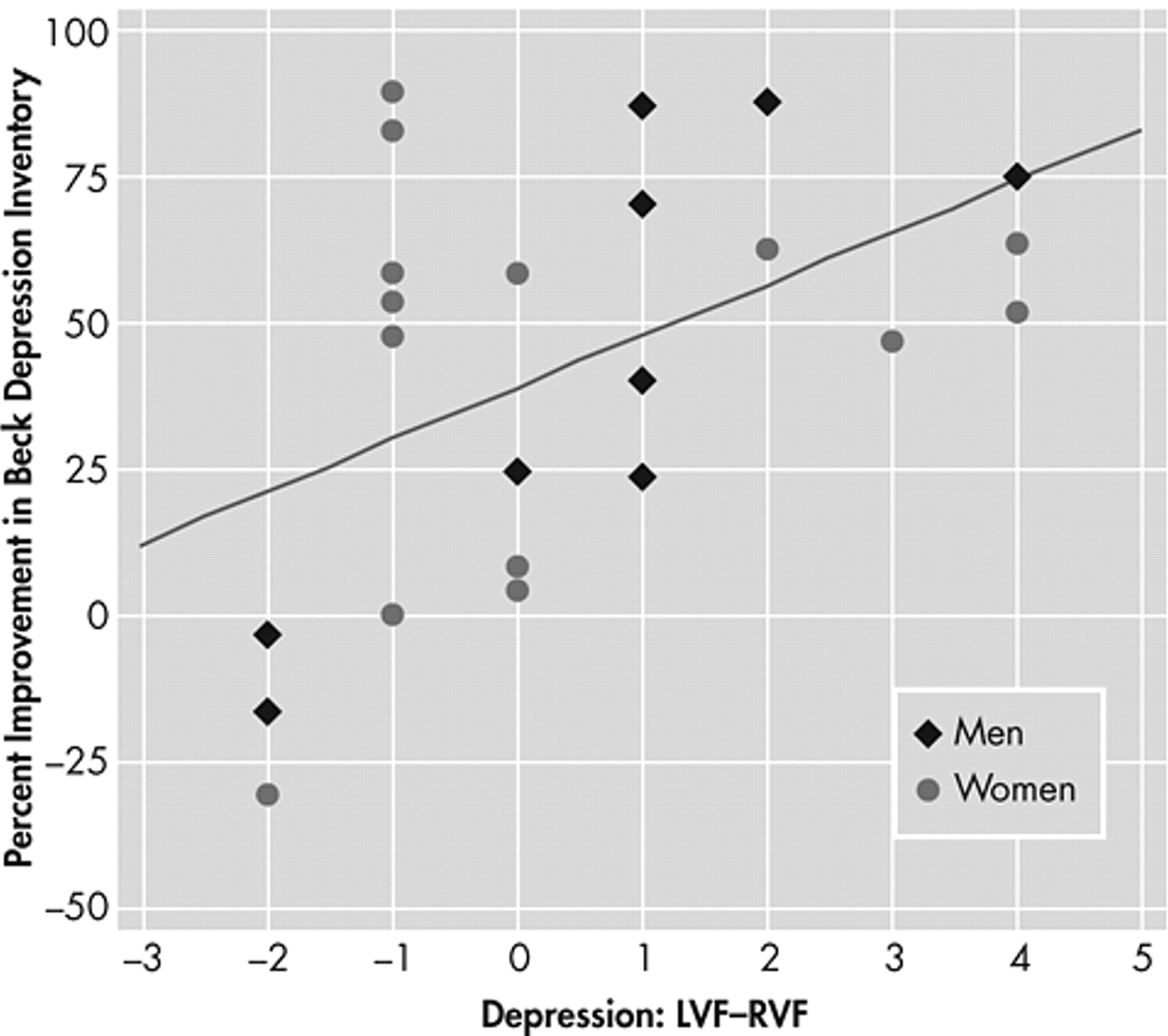
For all 23 patients there was a significant Pearson’s correlation between the percent improvement in BDI from initial score to discharge score and the intensity of depression rated by patients as they looked out the left visual field (LVF) minus that from their right visual field (RVF) (r=0.48, p<0.01). Neither the initial BDI (p>0.6), age (p>0.6), diagnostic category (p>0.13), nor handedness (p>0.33) acted as a significant covariate with lateral visual field stimulation in predicting the outcomes to the rTMS. For the nine men, this correlation was strong (r=0.82, p<0.005), and for the 14 women it was weaker (r=0.27, p=0.18, nsec).
Figure 2 shows these data graphically.
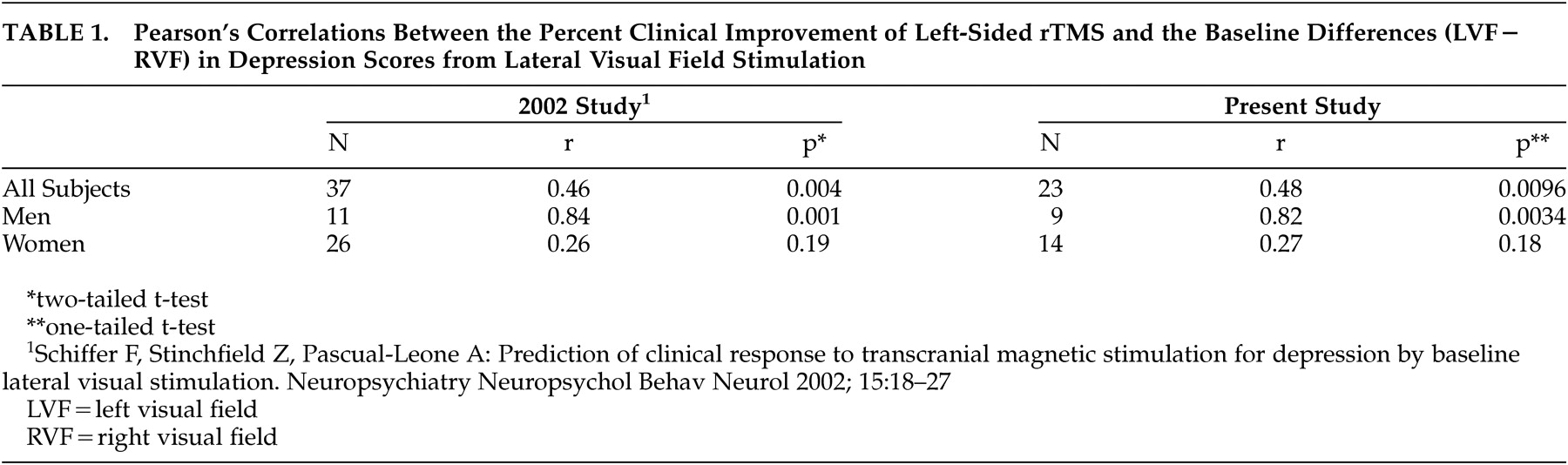
Table 1 shows the comparable correlations from the 2002 study
9 alongside those from the present study, and shows almost identical correlation values for the data from the two independent studies.
In the present study, the group predicted to do well (LVF−RVF>0, N=10) had a 60.8%±20.6 decrease in BDI from initial to discharge score while those with LVF−RVF<0 (N=9) had a decrease in BDI of 31.2%±44.4. This difference was significant by a one-tailed t test (t=−1.83, df=11, p=0.047). The hypothesis that subjects who had higher depression ratings when looking out left visual field than right visual field (LVF−RVF>0) would have a positive response to left-sided transcranial magnetic stimulation (TMS)
10,
11 was fulfilled in all 10 cases (
Figure 2 ). However, the hypothesis that subjects with LVF−RVF<0 would do poorly with left-sided TMS failed in five of nine cases. Interestingly, all of the predictive failures occurred in women and all were less than 55 years old (42.6±6.5 years). There was a strong correlation between lateral visual field stimulation and change in BDI (r=0.83, N=13, p<0.0003) for men and women 55 years or older. There was a weak correlation between lateral visual field stimulation and percent change in BDI for women less than 55 years old (r=0.07, p>0.8, nsec). Two subjects (one man) were left-handed and their responses to rTMS were predicted by lateral visual field stimulation.
Nine subjects had at least a 2-point difference between left visual field and right visual field on lateral visual field stimulation. Of these, six (two men) had a positive difference and three (two men) had a negative difference, and all had responses to rTMS that were correctly predicted by the lateral visual field stimulation. For these nine subjects, the correlation between BDI percent change and lateral visual field stimulation (LVF–RVF) depression scores was quite high (r=0.88, p=0.0008).
DISCUSSION
In this study we were able to replicate the overall and within gender correlations that we reported in 2002.
9 In both studies, patients with a relative right negative hemispheric emotional valence (reporting more intense feelings of depression while looking out of the left visual field than the right visual field) tended to do well in response to left-sided rTMS at 10 Hz. In the present study, those who did not follow the predictions were women predicted to do poorly by lateral visual field stimulation, and of these five, all were younger than 55 years. Transcranial magnetic stimulation studies
17,
18 indicate that menstrual cycle hormonal changes can affect the corpus callosal transit time which would be expected to alter the predictability of lateral visual field stimulation. Throughout the literature on laterality, there has been an impression that for many tasks women may be less lateralized than males,
19 –
21 and if true, this premise may relate to our findings. However, lateral dichotic listening tests predicted the response to fluoxetine in females,
22 so the meaning of our gender findings will need further exploration.
Regardless of the theoretical basis for our findings, the idea—that we have been able to predict in two studies which males would respond to left-sided rTMS—represents an important step in improving the efficacy of rTMS. A next step would be to see if subjects who are predicted by lateral visual field stimulation to do well in response to right-sided rTMS do so. If so, the efficacy of rTMS would be markedly improved.
Speer et al.
23 studied 10 adult patients with major depression who were treated with two trials of TMS, one at 20 Hz and one at 1 Hz. In addition to outcome measures, they studied each patient with baseline positron emission tomography (PET) scans that were repeated after each of the two 10-day treatment protocols. They found that subjects who responded to 20 Hz did poorly with 1 Hz and that subjects who responded to 1 Hz did poorly with 20 Hz. The PET scans showed the largest changes in the left hemisphere in the prefrontal cortex, cingulate, and amygdala. On average these areas showed increased activity following the 20 Hz treatment and decreased activity following the 1 Hz treatment. This study suggests that patients seem to be divided into two groups, one that benefited from left sided activation and one that did not. A future study might investigate whether those who responded to the left-sided 20 Hz course of treatment would feel improvement when they look out of the right visual field compared to the left visual field after lateral visual field stimulation, and whether those who responded to the 1 Hz treatment would respond to lateral visual field stimulation with more improvement in affect when looking out of the left visual field compared to the right visual field.
Kimbrell and associates
24 also found that patients who responded to left-sided TMS at 20 Hz tended to do poorly with 1 Hz stimulation and vice versa. Those who responded better to the 20 Hz stimulation tended to have a relative hypoperfusion of generalized cerebral blood flow by baseline PET. Inspection of the authors’ data suggests that the baseline hypoperfusion was greatest in left anterior sites, especially the left anterior cingulate. The authors presented a case of the one patient who received PET scans after treatment as well as before. This patient, a 46-year-old man with refractory unipolar depression with marked baseline left-hemispheric hypoperfusion, had his perfusion normalized after clinically successful TMS at 20 Hz. This patient did poorly with 1 Hz. We feel that future studies would do well to include baseline lateral visual field stimulation measurements to see if baseline imaging measures and outcomes to TMS bear a relation to it.
Mottaghy and colleagues
25 used single photon emission tomography (SPECT) to predict subsequent clinical responses to left-sided rTMS in 17 patients. When a corrected threshold was used, baseline SPECT activity in the right periinsular cortex correlated positively with the rTMS outcomes.
Eschweiler et al.
26 used multisite near-infrared spectroscopy during an arithmetic and a left and a right mirror drawing task to predict the response to rTMS. The left-handed mirror drawing task and a total hemoglobin, but neither oxy nor deoxy-hemoglobin at F3 but not other sites, were able to predict which four of the 12 patients would have a greater than 30% reduction in HAM-D following left-sided rTMS. Compared with SPECT, PET, and near-infrared spectroscopy, lateral visual field stimulation is inexpensive and convenient.
A number of authors have asserted that hypoactivity of the left frontal cortex during baseline states is associated with depression, but this hypothesis has been inconsistently supported by the literature. For instance, Henriques and Davidson
27 have suggested that depression is associated with relatively less left frontal activity by alpha EEG, but this finding has often not been replicated.
28,
29 Some authors
30,
31 but not others
32,
33 have drawn a similar conclusion using functional imaging. Robinson et al.
34 have argued that left frontal strokes are more often associated with depression than strokes from other areas, but this assertion is countered by Carson and his associates.
35 Some studies,
36,
37 but not others,
38 –
40 have shown increased left frontal activation after successful treatment for depression with antidepressants or psychological treatment. Studies correlating left rTMS treatments with increases in left frontal cerebral blood flow have reported a significant relationship,
25,
41 but a relationship has not been found between positive outcomes from rTMS and increases in left frontal activation when comparing before and after a treatment course.
25,
41 We have argued
1 that some of the inconsistencies in research involving cerebral laterality may be due to the tendency for researchers to average their data without regard to hemispheric emotional valence, and we suggested
1 that by including hemispheric emotional valence as a baseline variable in the evaluation of such data, such findings might be further clarified. Although lateral visual field stimulation has been found by blood-oxygen-level-dependent (BOLD) fMRI
14 and EEG
13 to activate the contralateral hemisphere, we have not yet studied whether the side of negative hemispheric emotional valence correlates with alterations in cerebral frontal activity.
We reported
12 that among psychotherapy patients who had lateralized affective responses to lateral visual field stimulation, 73% of 15 patients with major depression had a right negative hemispheric emotional valence, and among 14 with posttraumatic stress disorder (PTSD), 71% had a left negative hemispheric emotional valence. Cohen et al.
42 reported the results of a double-blind, controlled trial of right-sided rTMS among 24 patients with PTSD. They found that these patients had highly significant reductions in PTSD symptoms in response to TMS over the right dorsolateral prefrontal cortex at a stimulating frequency of 10 Hz compared with a 1 Hz inhibitory frequency or with a sham condition. The fact that the positive right hemispheric emotional valences that we found in our patients with PTSD and Cohen’s results are consistent our hypothesis about rTMS and laterality could be coincidence but does deserve serious further study because of the potential benefit to patients with this disorder. To date no adequate hypothesis has been put forth to explain the benefits of rTMS,
43 and so the investigation of even novel hypotheses should be undertaken.
Our findings may apply as well to other lateralized treatments such as ECT. There is evidence that psychotropic medications have lateralized effects,
44,
45 and several authors have predicted responses to psychotropic medications by measurement of asymmetric brain activation by dichotic listening,
22,
46 EEG,
46,
47 fMRI,
48 and PET.
49 We feel that lateral visual field stimulation should be explored as a possible method for predicting such outcomes.