Comorbidity of mental disorders, substance use disorders, and chronic pain unrelated to cancer is common and contributes to overall disability and poor treatment outcomes. Studies of persons with depression in outpatient clinical settings have found prevalence rates for pain symptoms ranging from 40% to 85% (
1,
2 ). In an analysis of data from the National Comorbidity Survey Replication, rates of chronic spinal (back or neck) pain were 29.3% among individuals who met criteria for any mental disorder in the past 12 months, 34.5% among those with a mood disorder, 31.4% among those with an anxiety disorder, and 23.4% among those with a substance use disorder; the rate of chronic spinal pain among those who did not meet criteria for a mental disorder was 15.9% (
3 ). Sixty-three percent of persons with depression surveyed in the first wave of the Healthcare for Communities Survey (HCC) reported having a chronic pain condition (
4 ). Studies have also found high rates of pain-related diagnoses among persons with substance use disorders (
5,
6,
7 ). Pain severity is associated with poor depression outcomes (
2 ), and persons with both chronic pain and depression have been found to have greater emotional distress, poorer health-related quality of life, and poorer physical functioning than those with only one of these conditions (
1,
2,
4 ).
Previous studies have assessed the individual effects of mental disorders and chronic pain on work and employment outcomes. Depression or depressive symptoms have been associated with increased work disability (
8,
9,
10,
11,
12 ), reduced productivity, reduced aggressiveness in job seeking, reduced ambitions in job choice (
13 ), and higher rates of unemployment (
8,
14,
15 ). Similarly, chronic pain has been associated with negative employment outcomes, including increased sick leave, among individuals with frequent headaches (
16 ); reduced productivity and absenteeism among those with migraine (
14,
17 ); unemployment and lost work days among those with chronic low back pain (
18,
19,
20 ); and work disability among those with rheumatoid arthritis (
21 ).
A few studies have examined the relationship between work-related outcomes and comorbid mental disorders and chronic pain. Several studies have identified psychological factors as predictive of return-to-work status among persons with low back pain (
22,
23,
24 ). In a survey of Dutch adults, those with chronic back troubles, rheumatism, migraine, or mood disorders lost significantly more days of work because of health in the previous year than those without these conditions (
25 ). When a mood disorder was present with a physical condition, the number of lost work days increased. When both chronic back troubles and a mental disorder were present, the number of work days lost was greater than the sum of days lost associated with each condition alone (that is, the effects were synergistic). In a survey of adults from several European countries, the presence of painful physical symptoms and major depression had an additive effect on the number of lost work days (
26 ).
In an analysis of data from the Health and Retirement Study, persons with comorbid pain and depression were more likely to be unemployed and to report health-related work limitations than those with either pain or depression alone, and the percentage who reported either outcome increased with pain severity (
27 ). A separate analysis found that participants with depression plus severe pain were also more likely to lose their jobs than those with depression alone (
28 ). The study focused on individuals who were near retirement, however, and thus did not assess all persons of working age. In addition, the presence and severity of pain but not its location were assessed, and assessment of mental health was limited to depressive symptoms.
In the study reported here, we sought to examine the independent and interactive effects of common mental disorders and chronic pain conditions on several employment and work outcomes. The data were obtained from a population-based survey of U.S. adults between the ages of 18 and 65 and included information on varying levels of impairment. We hypothesized that individuals with both chronic pain and a mental disorder would report higher rates of health-related unemployment and work limitations than those with either a mental disorder or a chronic pain condition alone.
Methods
Data source
Data are from the second wave of HCC (HCC2), a part of the Robert Wood Johnson Foundation's Health Tracking Initiative conducted in 2000–2001. HCC was a nationwide telephone survey designed to track the effects of the changing health care system on individuals at risk of alcohol, drug, and mental disorders (
29 ). The HCC respondents were a stratified probability sample of participants in the Community Tracking Study (CTS), a nationally representative study of the U.S. civilian population (
30 ). Details of the sampling design have been presented elsewhere (
29 ).
The initial HCC survey was conducted in 1997–1998 (HCC1). HCC2 was conducted in 2000–2001 and was designed to follow up on all individuals who responded to HCC1. Of the 14,985 respondents selected for HCC1, 9,585 complete interviews were obtained, for a response rate of 64%. A total of 6,659 of the 9,585 HCC1 respondents (70.9%, weighted) completed the HCC2 survey. Informed consent was obtained verbally before the interview, and the study was approved by the institutional review boards at the University of California, Los Angeles, and RAND. Respondents with missing data for mental disorders and chronic pain conditions were excluded; thus the number of respondents in the sample for this study was 5,328.
Variables
The presence of four common mental disorders in the past 12 months—major depression, dysthymia, generalized anxiety disorder, and panic disorder—were assessed by using the short-form version (
31 ) of the World Health Organization's Composite International Diagnostic Interview (CIDI-SF) (
32 ), which is based on the
DSM-III-R (
33 ). The presence of lifetime mania and psychosis were assessed by single screening questions. Chronic pain conditions and other chronic conditions were identified by self-report. The HCC survey asked about 17 different chronic conditions, four of which were defined for this analysis as chronic pain conditions: arthritis, chronic back problems, migraine or chronic headaches, and "other" chronic pain conditions. The four chronic pain categories and four common mental disorders were used to create four categories indicating the presence of chronic pain or a mental disorder or both: a mental disorder without chronic pain, a mental disorder with chronic pain, chronic pain without a mental disorder, and neither a mental disorder nor chronic pain.
Problem alcohol use was defined as a core total score of 8 or higher on the Alcohol Use Disorders Identification Test (AUDIT) (
34 ). Problem drug use was defined as a positive answer to either of two questions, adapted from the CIDI, assessing tolerance of a drug's effects or emotional or psychological problems as a result of drug use. The physical component summary score and mental component summary score from the Short-Form 12-Item Health Survey (SF-12) (
35 ) were used as aggregate measures of physical functioning and mental functioning, respectively. Both summary scores have a mean±SD score of 50±10 in the U.S. adult population; a higher score indicates better functioning. Level of pain interference with the respondents' daily activities was derived from the SF-12 pain interference item (responses are extremely or a lot, moderately or a little bit, and not at all).
Employment outcomes were assessed by self-report. These included the number of weeks worked in the past 12 months, the number of days of work missed in the past 30 days, and the number of work days on which the respondent arrived late or left early in the past 30 days. Respondents were also asked how many of the work days missed or shortened were because of health problems. Whether a respondent's ability to work was limited by health problems was assessed with the following question: Are you unable to work or unable to work as much as you'd like to because of your health?
Data analysis
Sample weights designed by the HCC study's statisticians were used to weight the data to make them representative of the U.S. population and to adjust for the probability of selection, nonresponse, and the number of households in the CTS survey that did not have a phone. Statistical differences were assessed with chi square tests for categorical variables and F tests for continuous variables. Logistic regression analysis was used to estimate odds ratios for work impairment on the basis of risk factors, while controlling for sociodemographic covariates, mean number of other chronic health conditions (the other 13 health conditions asked about that were not defined as chronic pain), and presence of an alcohol or drug use disorder. Linear regression analysis was used to estimate coefficients for days of work missed; coefficients were assumed to be distributed normally on the basis of the sample size (
36 ). For nondichotomous categorical covariates (race, marital status, and education level), dummy variables were created for use in the models.
No work in the past 12 months was defined as a negative response to questions concerning current employment and whether any work for pay was done in the past 12 months. A composite variable to estimate work missed was created by summing days of work missed and 40% of the days where the respondent arrived late or left early because of health problems in the past 30 days; the variable was modeled after the approach taken by Kessler and colleagues (
10 ). In sensitivity analysis, logistic regression analyses were rerun in which no work in the past 12 months included only respondents not currently working; no significant differences in results were noted. Dichotomous variables that indicated the presence of a mental disorder and the presence of a chronic pain condition were included in all the models, and an interaction term concerning the presence of a chronic pain condition and the presence of a mental disorder was added to estimate the effect sizes for individuals with both a mental disorder and comorbid chronic pain. All analyses were conducted with software for the statistical analysis of correlated data (SUDAAN, version 9.01).
Results
Sociodemographic characteristics
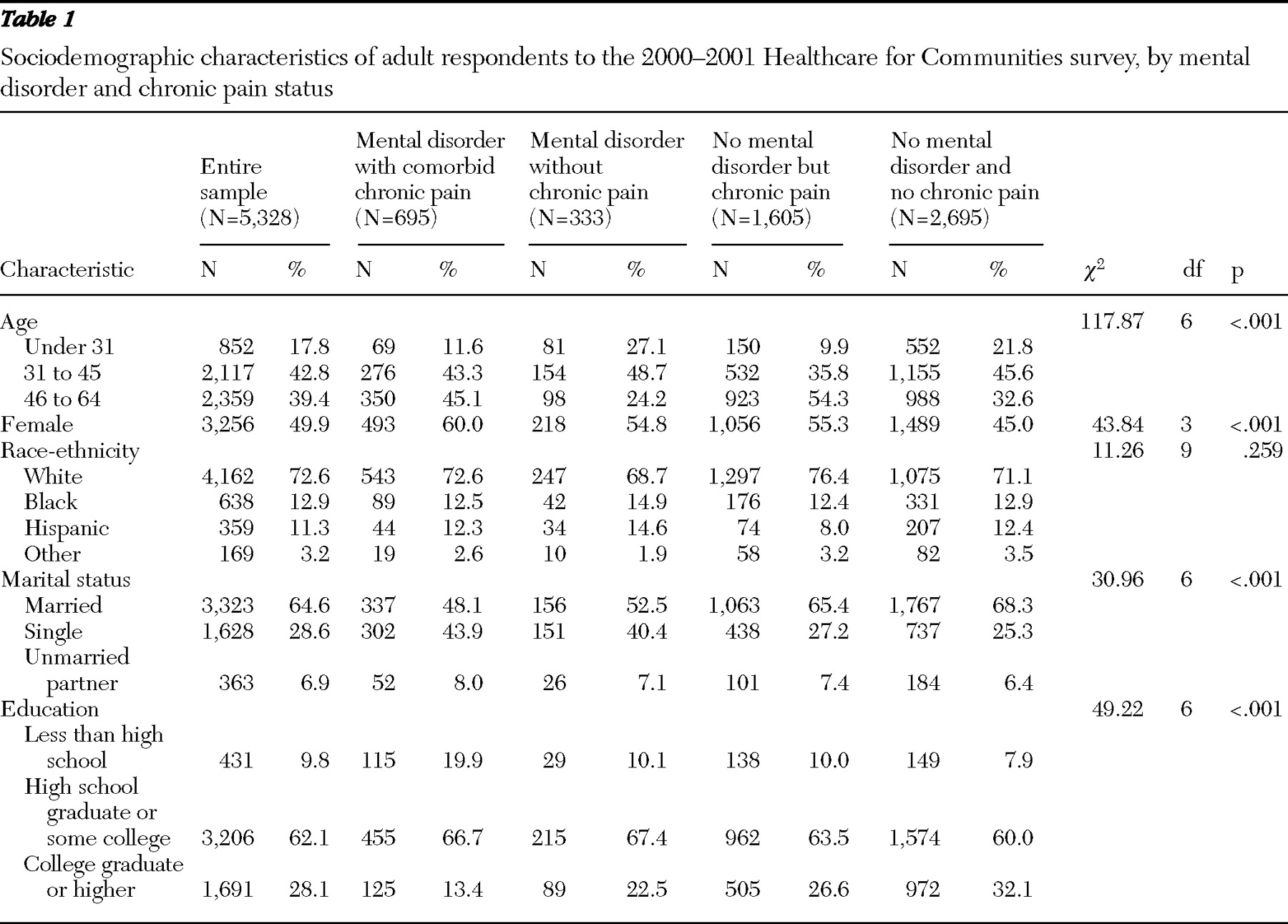
Table 1 presents data on the sociodemographic characteristics of the HCC2 respondents ages 18 to 64, by chronic pain and mental health status. The four groups differed significantly in all characteristics except race-ethnicity. The proportion of women was significantly higher in the group with a comorbid mental disorder and a chronic pain condition than in the other three groups. Individuals in this group were also least likely to have graduated from college or to be married.
Clinical characteristics
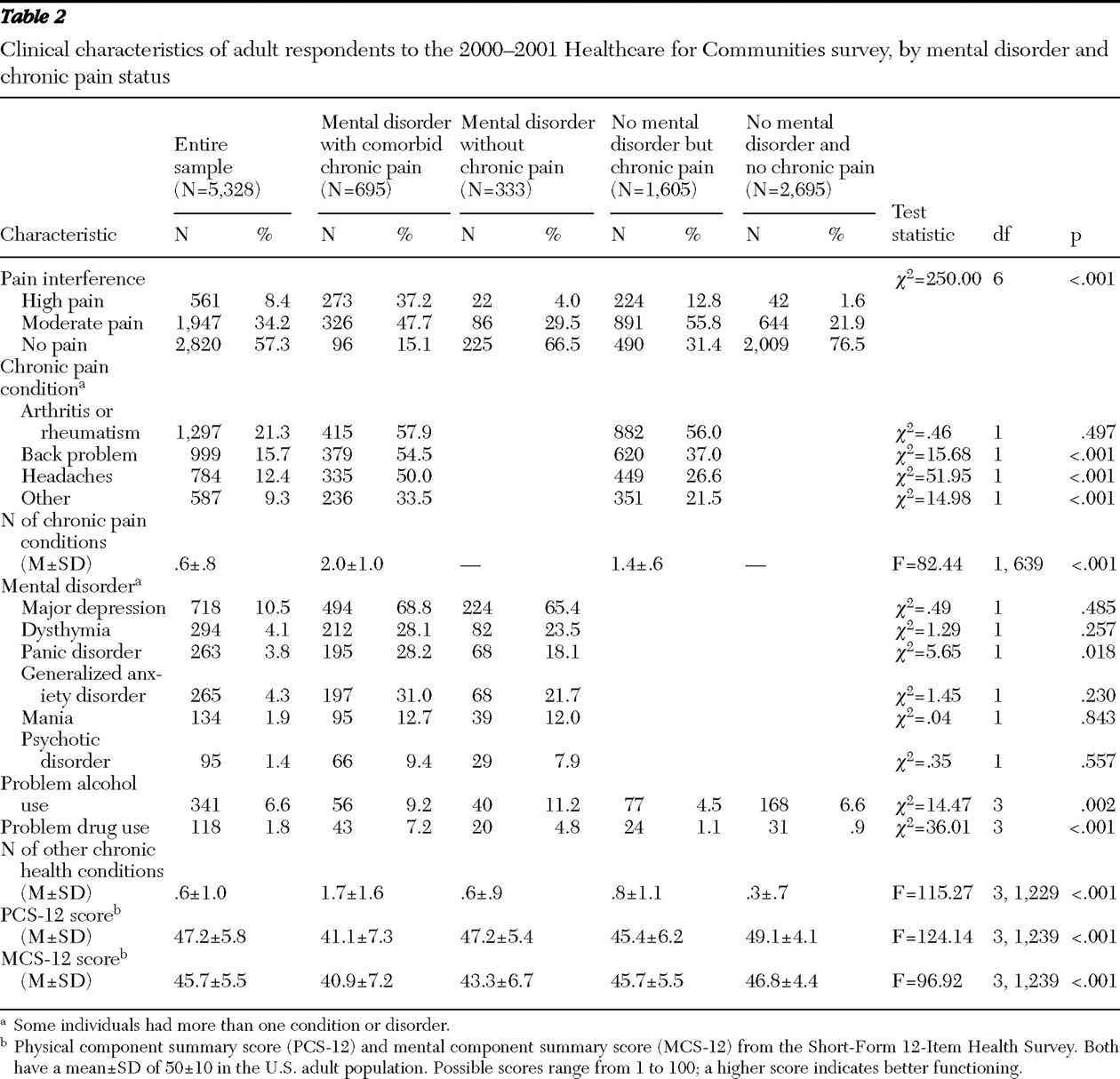
Table 2 shows the clinical characteristics of the respondents, by chronic pain and mental health status.
Pain types, interference, and other chronic conditions
Compared with respondents with chronic pain but no mental disorder those with comorbid chronic pain and a mental disorder had higher current prevalence rates of chronic back troubles, chronic headaches, and other chronic pain disorders; were more likely to report a high level of pain interference; and had a higher mean number of chronic pain conditions. The mean number of other chronic health conditions was highest and the mean physcial component summary score (PCS-12) was lowest in the group with a comorbid mental disorder and chronic pain compared with the other three groups.
Employment outcomes
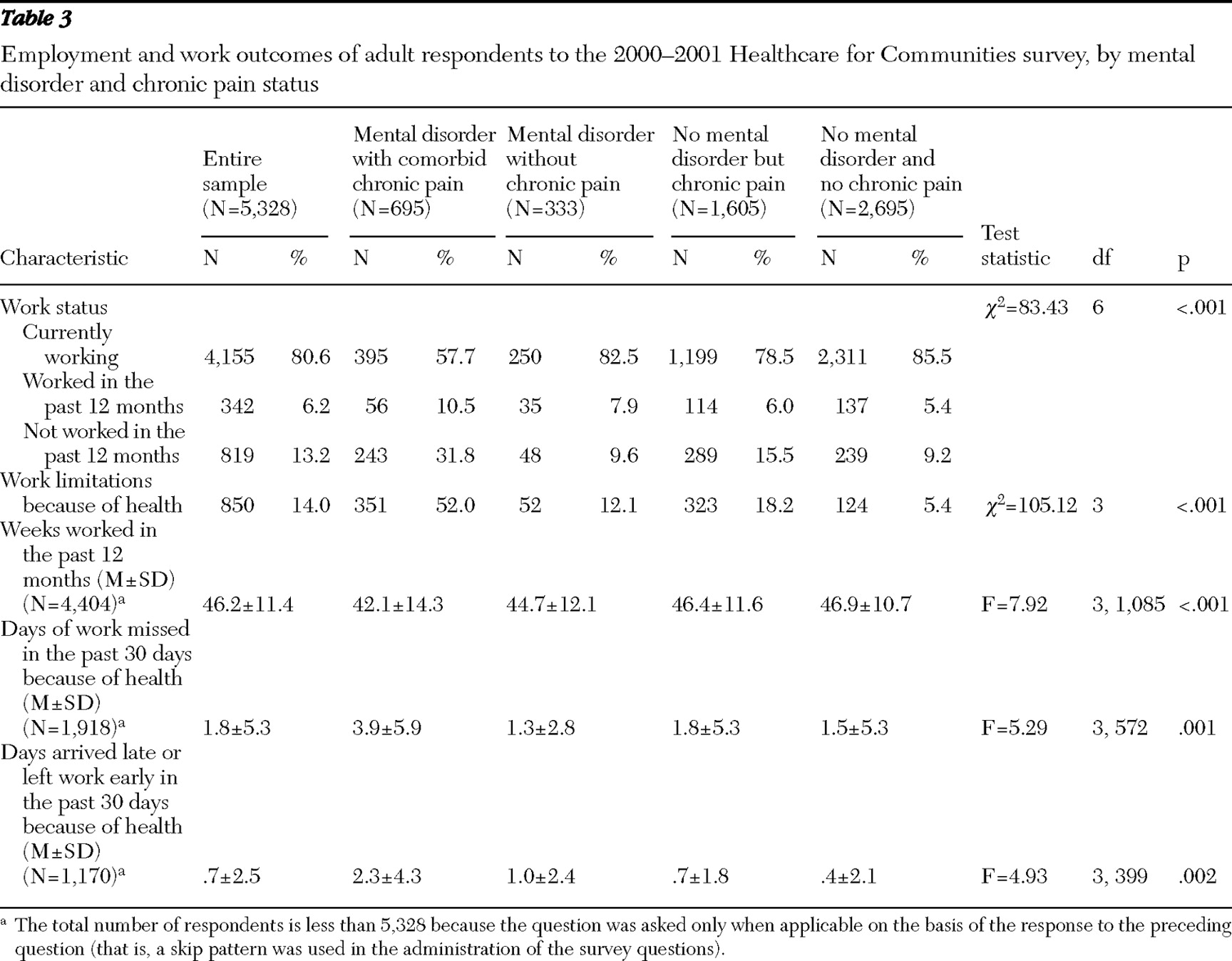
Table 3 presents data on employment outcomes, by respondents' chronic pain and mental health status. Individuals with a mental disorder and chronic pain were least likely of the four groups to be currently working and most likely to report that their ability to work was limited because of health. This group also had a higher mean number of days of work missed or on which respondents arrived late or left early in the past 30 days because of health compared with the other three groups. The mean number of weeks worked in the past 12 months was also lowest for this group, although in post hoc pairwise comparisons, this group did not differ significantly from the group with a mental disorder with no chronic pain.
The presence of both a mental disorder and a chronic pain condition was significantly more likely than the presence of either condition alone to be associated with no work or with limitations in work in the past 12 months. In pairwise comparisons, individuals with a chronic pain condition without a mental disorder were not significantly different from those with neither condition with respect to mean weeks worked, mean days of work missed because of health, or mean days arrived late or left early because of health. Those with a mental disorder without chronic pain were not significantly different from those with neither condition in respect to mean days of work missed or arrived late or left early because of health.
Logistic and linear regression analyses
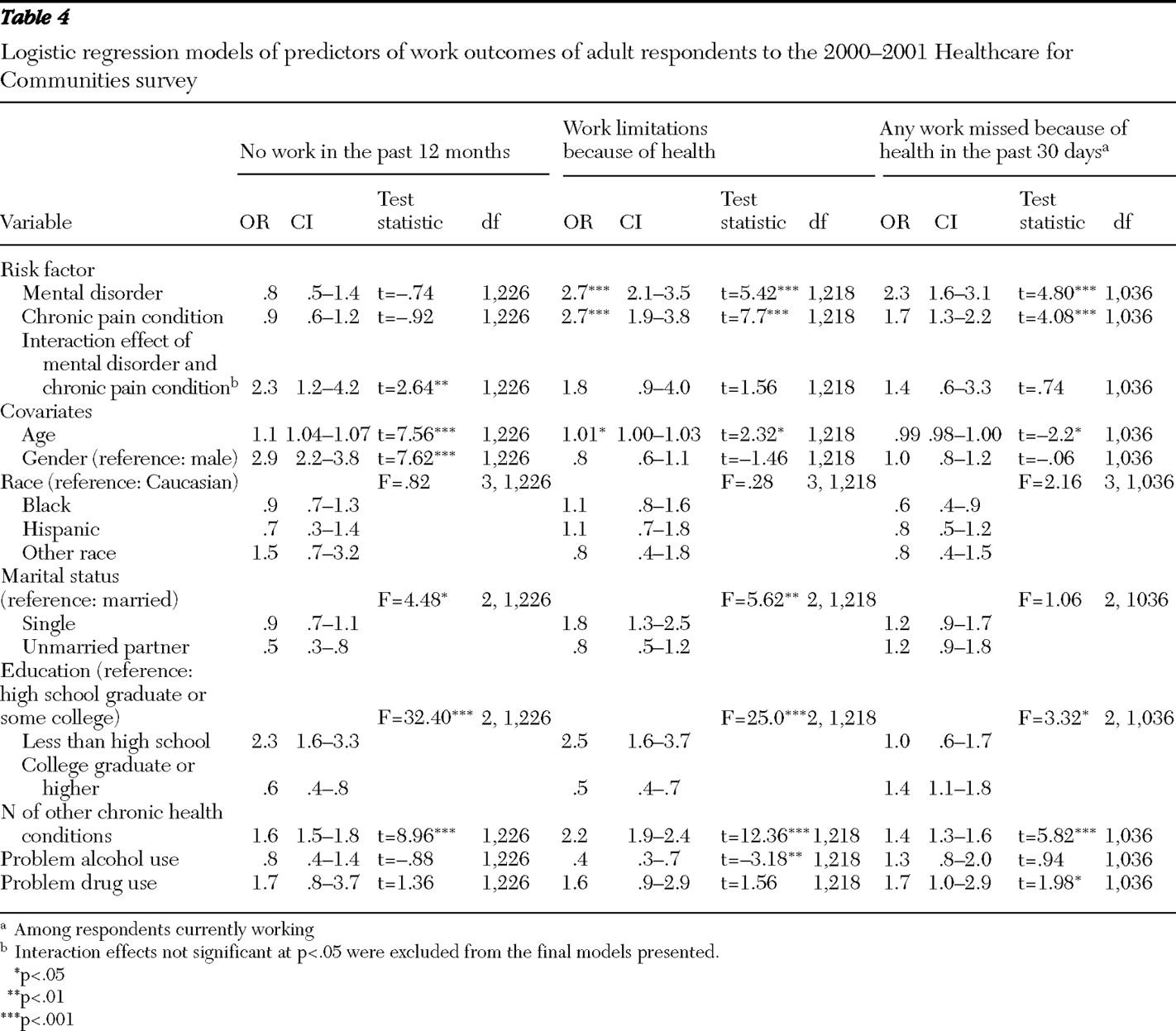
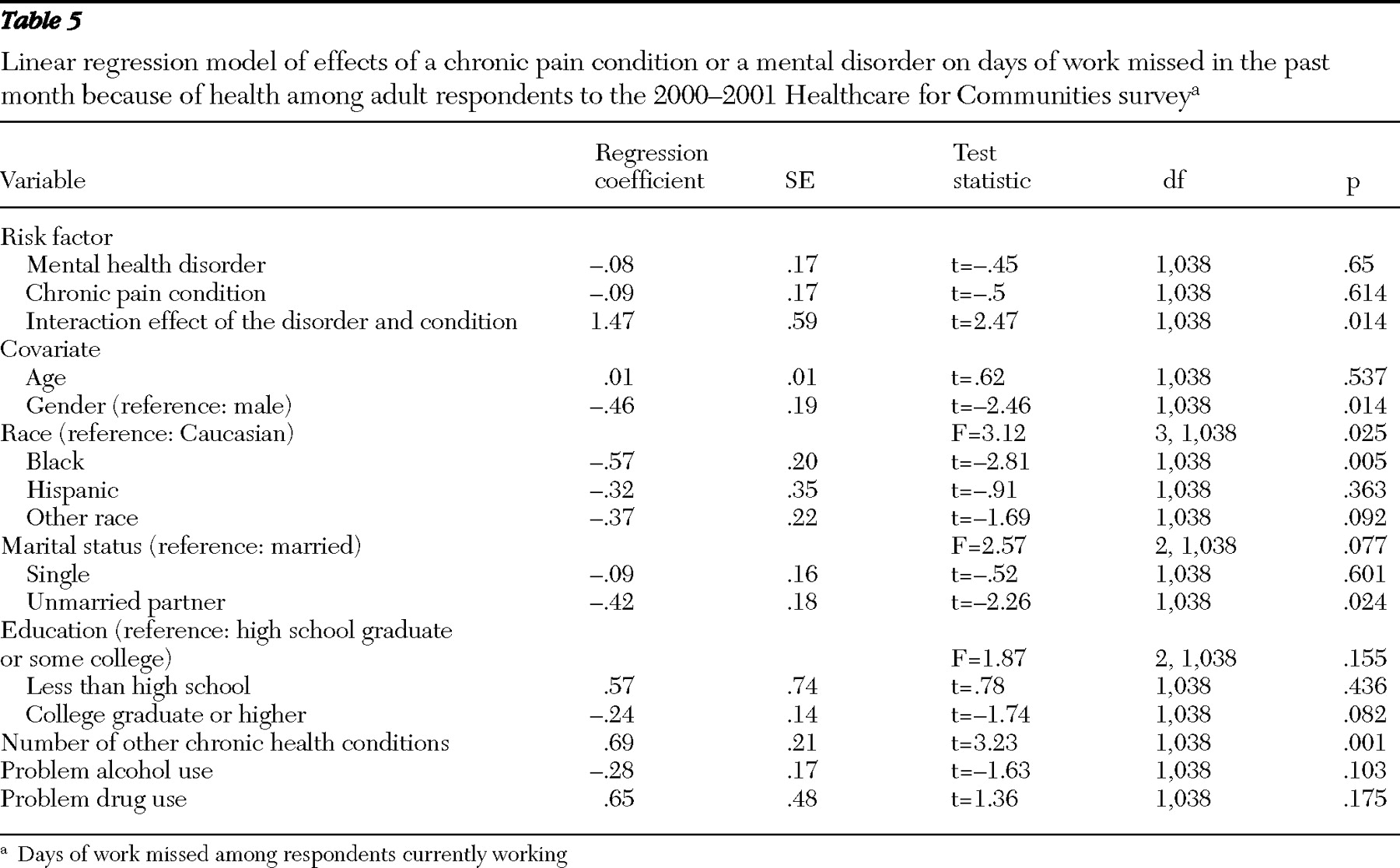
Tables 4 and
5 present the results of multivariate regression analyses examining risk factors for four outcomes. Logistic regression was used for three outcomes—no work in the past 12 months, ability to work limited by health, and any work missed—and linear regression was used for the fourth outcome—days of work missed in the past 30 days because of health.
The presence of a mental disorder and the presence of a chronic pain condition were each independently associated with limitations in the ability to work because of health. Likewise, among respondents who were currently working, the presence of either a mental disorder or a chronic pain condition was independently associated with work missed in the past 30 days because of health (
Table 4 ). For these outcomes, however, the interaction between presence of a mental disorder and presence of a chronic pain condition was not significant.
In contrast, a significant interaction effect was found between presence of a mental disorder and presence of a chronic pain condition on the outcome of no work in the past 12 months (
Table 4 ) and of number of days of work missed in the past month because of health (
Table 5 ). These findings suggest effect modification and specifically suggest that mental disorders have a greater effect on how much a person is able to work when a chronic pain condition is also present. In stratified analyses (data not shown), this effect persisted for women but not for men.
In sensitivity analyses, we added pain interference as an additional covariate, but this did not change the results substantially, which suggests that the effects were not limited to persons with more severe pain.
Discussion
Our study of the association of chronic pain and mental disorders with employment in the general population has shown that each was independently associated with a doubling of the likelihood of reported work limitations because of health. Furthermore, when both conditions were present among women, there was a synergistic effect on the odds of having no paid employment in the previous year and on the number of work days missed in the previous month because of health. Results are consistent with findings from a recent analysis of respondents ages 55 to 65 years in the Health and Retirement Study (
27 ) and expand on the findings in that study to confirm the association between comorbid pain and any mental disorder and poor employment outcomes among persons ages 18 to 64.
In our study absence from the workforce was seen primarily among respondents with a mental disorder and comorbid chronic pain. An interaction effect between having a mental disorder and having chronic pain was significantly associated with no work for pay in the previous year and number of work days missed in the previous month because of health but not with limitations on work because of health. In our data approximately half of those who reported that their ability to work was limited by health problems also reported one or more of the other forms of work disability assessed, suggesting that a positive answer to the question about work limitations captured a broad range of severity in terms of work functioning. In addition, reports of work limitations indicate that disability is present but not how much. Having either a chronic pain condition or a mental disorder alone may be sufficient to cross a certain threshold level of impairment, but the degree of impairment worsens when both are present. The gender effects observed may reflect increased rates of depression, anxiety, and somatic symptoms among women (
26,
37 ) or differences in the total workload—paid and unpaid (for example, housework)—compared with men (
38 ).
Strengths of this study are its population-based design and the collection of data on both DSM-III-R mental disorders and chronic medical conditions. Limitations include the self-report nature of information about medical and chronic pain conditions, limited data on substance use disorders, and the cross-sectional nature of the information obtained. The outcome of no work in the past 12 months is less specific to health and may have been influenced by other unmeasured variables. In addition, our data did not assess other aspects of work disability, such as productivity, that may be affected by chronic pain or a mental disorder.
Although the associations found between mental health, chronic pain, and employment outcomes are robust, the data are cross-sectional and thus no conclusions can be drawn about the direction of the association. In addition, data did not include information on the duration of pain or symptoms of a mental disorder. Prospective studies have demonstrated an association between depressive symptoms and subsequent unemployment (
15 ) and loss of employment and subsequent depression (
13,
39,
40 ). Depression has also been shown in previous studies to both precede and follow the development of chronic back pain (
41,
42,
43,
44 ). A World Health Organization study found that either baseline depression or anxiety and moderate-to-severe occupational disability predicted the onset of persistent pain disorders 12 months later (
45 ). A prospective analysis of data from the Health and Retirement Survey found an association between depression plus severe pain and subsequent loss of employment compared with depression alone (
28 ). In our study, the fact that the effects of having a chronic pain condition and a mental disorder were synergistic on the odds of no work and on the number of days missed when respondents were working suggests that pain and mental illness may be mutually reinforcing factors leading to impairment in functioning and decreased ability to meet the demands of the workplace.
In this study, 68% of those with a mental disorder also had a chronic pain condition and 30% of those with a chronic pain condition also had a mental disorder. Previous studies have documented improvement in employment outcomes with enhanced treatment of depression (
46,
47,
48,
49 ). Given the high degree of comorbidity between chronic pain and mental disorders and the increased disability in the presence of both conditions, future studies should examine the single and joint effects of treatment for each of these disorders on employment outcomes.
Conclusions
Results of this study suggest that having a mental disorder is more strongly associated with certain work disability outcomes when the disorder is accompanied by chronic pain, especially among women. Future studies should examine the temporality of this association and the effects of treatment for each of these disorders on employment outcomes.
Acknowledgments and disclosures
Dr. Braden is supported by a Ruth L. Kirschstein National Research Service Award Institutional Research Training Grant (T32) from the National Institutes of Health. The authors thank Kenneth B. Wells, M.D., M.P.H., for access to the HCC data and Ming-Yu Fan, Ph.D., for statistical help.
The authors report no competing interests.