However, little is known about whether some subgroups of patients with depression are significantly more prone to high utilization than others. Depression is a heterogeneous disorder involving disruptions in mood, appetite, sleep, motor activity, and cognition, which vary from one individual to the next (
11 ). Moreover, depression is commonly comorbid with other psychiatric illnesses (
12 ), general medical illnesses, and medically unexplained symptoms (
9 ) and is associated with a broad range of impairments (
12 ). In addition, a high level of use of general medical services is not specifically symptomatic of depression, but rather constitutes a "behavioral response" (
13 ) that may vary depending upon several factors, including the constellation of depressive symptoms and comorbid symptoms or illnesses. Identifying subgroups of persons who contribute significantly to high utilization among persons with depression could improve screening procedures designed to identify such patients in primary care settings, bring about more precise targeting of patients with depression for participation in enhanced treatment programs, and inform changes in treatment for specific subgroups.
Several considerations led us to examine whether patients with depression who have comorbid chronic pain constitute a subgroup with higher medical costs than patients with depression who do not have pain. First, depression and chronic pain frequently coexist (
14,
15 ) and may amplify one another (
16 ). Second, one impediment to diagnosing depression in primary care settings, where most patients are treated (
17 ), is the presentation of somatic complaints (
18 ), many of which involve pain (
19 ). Third, independent of depression, the costs of chronic pain are well documented (
20,
21,
22,
23 ) and have been characterized as "astronomical" (
24 ).
Previously, we reported that the presence of disabling chronic pain among primary care patients with major depression was associated with greater clinical burden, including significantly lower quality of life, increased somatic symptom severity, and high prevalence of comorbid panic disorder (
14 ). In the study reported here, we examined whether individuals with major depression and disabling chronic pain have medical costs that are higher than those of patients with depression who have either nondisabling chronic pain or no chronic pain. We hypothesized that after we adjusted for general medical illness, total medical costs among patients with major depressive disorder would be significantly higher for the subgroup with disabling chronic pain than for the group without pain or the group with chronic pain that was nondisabling. Finally, to further understand the relationships between major depressive disorder and medical costs, we separately compared the subgroups of participants with depression who had disabling chronic pain and those who did not have chronic pain with three groups of patients without depression: those with disabling chronic pain, those with nondisabling chronic pain, and those with no pain.
Methods
Sample
All study participants were members of Kaiser Permanente, a health maintenance organization (HMO) in northern California. The institutional review boards of both Stanford University Medical Center and Kaiser Foundation Research Institute approved the study. During a 12-week period in 2002, a total of 12,000 members were randomly selected within one week of a primary care visit to receive a mailing that included a cover letter, a consent form with an option to decline participation, and self-report questionnaires. In addition to being a Kaiser member and having recently visited an internal medicine or family practice clinic, participants also had to be between the ages of 21 and 75 and sufficiently literate in English to complete the self-report questionnaires. Additional details about exclusion criteria and participant recruitment can be found elsewhere (
14 ).
Of the individuals initially sampled, a total of 1,290 (11%) were ineligible because of literacy barriers (N=428) or because they could not be located as a result of incorrect contact information (N=862). Of the 10,710 potential participants, 3,808 (36%) refused to participate and 1,094 (10%) failed to respond. Thus 5,808 individuals (54%) participated. Compared with those who either were ineligible or did not respond (N=6,192), study participants were older (mean±SD age 53.3±13.6 versus 49.5±14.1, p< .001) and more likely to be female than male (58% versus 55%, p<.01).
Measures
Depression. Major depression was assessed with the Patient Health Questionnaire (PHQ) (
25 ), a self-administered version of the Primary Care Evaluation of Mental Disorders (PRIME-MD) (
26 ) that enables
DSM-IV diagnoses of major depressive disorder and other disorders. Its diagnostic validity among primary care patients is comparable to that of the PRIME-MD (
25 ). Because the questionnaire was mailed and not reviewed by a clinician, we used the eight-item version of the depression module (PHQ-8), which omits an item asking about suicidal ideation (
27 ). For each of the eight items, respondents were asked how often over the previous two weeks they had been bothered by various symptoms (not at all, several days, more than half the days, or nearly every day). Items were scored from 0, not at all, to 3, nearly every day. To meet criteria for a diagnosis of major depressive disorder, respondents had to endorse being bothered by five or more of eight symptoms for more than half the days (that is, a score of 10 or higher) for the previous two weeks, with at least one of the five items being depressed mood or anhedonia. Scores of 10 or higher on the PHQ-8 have a sensitivity greater than 99% and a 92% specificity for identifying patients with major depression compared with interviews with health professionals that use questions from the Structured Clinical Interview for DSM-IV and the PRIME-MD (
28 ).
Chronic pain. To determine whether chronic pain was present, participants were asked whether they were "currently troubled by pain or discomfort, either all the time or on and off." An additional item queried whether the pain had persisted for more than six months. To be considered to have chronic pain, participants had to endorse both of these items. This definition follows one developed by the International Association for the Study of Pain (
29 ) with two exceptions. First, consistent with the recommendations of Elliott and colleagues (
30 ), we included respondents with intermittent pain. Second, we used the more conservative six-month threshold, rather than thee months.
Pain-related disability. Pain-related disability was assessed with the Graded Chronic Pain Scale (GCPS) (
30,
31 ), a seven-item questionnaire that measures both pain intensity and interference with daily activities. The GCPS has a hierarchical structure allowing classification of respondents into one of four classes: grade 1 (low intensity, low interference), grade II (high intensity, low interference), grade III (moderate interference), and grade IV (severe interference). Those who met criteria for grades III and IV on the GCPS were defined as suffering from disabling pain.
General medical illness. A dichotomous variable was used to indicate whether or not the patient had a diagnosis of any of four chronic diseases: coronary artery disease, congestive heart failure, diabetes, or cancer. Diagnoses were derived from disease registries that Kaiser Permanente supports for each of these conditions. Kaiser Permanente tracks these illnesses because they are prevalent, costly, and amenable to aggressive intervention (
32 ).
Costs for general medical and psychiatric services. Data on costs were obtained from Kaiser Permanente's Cost Management Information System (CMIS), which integrates the financial ledger with databases tracking utilization of clinic, hospital, and ancillary services. Step-down accounting methods are used to fully allocate building and administrative overhead costs, as well as all variable costs, to services delivered to patients by using relative value weights specific to the northern California region of Kaiser Permanente. For the small percentage of members who receive some services covered by Kaiser from non-Kaiser providers, we also included the cost to Kaiser of these "outside" services. We used the total fully loaded cost of delivering Kaiser services, regardless of whether the patient paid a copayment.
Statistical methods
After adjustment for medical illness, six groups were compared on total costs (with and without the inclusion of costs for psychiatric services) and on various components of the total, including outpatient medical, outpatient psychiatric, emergency department, medication, and hospital costs. The reference group was patients with major depressive disorder and comorbid disabling chronic pain, and the other five groups were those with major depressive disorder and comorbid nondisabling chronic pain, those with major depressive disorder only, those with disabling chronic pain only, those with nondisabling chronic pain only, and those with neither pain nor depression.
The primary statistical method was an analysis-of-variance model, which compared the six groups on annual patient-dollar costs per year (aggregating the costs of the year before and the year after the index visit). The total cost variable was nonnormally distributed, and a natural log transformation was successful in normalizing the distribution for parametric analysis. Variances were homogeneous across groups for log-corrected costs. Group was entered as a fixed factor with six levels, and age, gender, ethnic minority status, and serious medical illness (presence or absence of one of four chronic medical illnesses—coronary artery disease, congestive heart failure, diabetes, and cancer) were entered as covariates. After total costs were analyzed, the six diagnostic groups were compared on specific areas of cost that constituted the total, including costs for emergency services, medication, outpatient medical care, outpatient psychiatric care, and inpatient general medical and psychiatric care. An alpha of .05 was used for statistical significance. To examine whether the effects of pain and depression on total cost were synergistic, we employed a linear regression model that included continuous measures of the severity of chronic pain and the severity of depression as well as their multiplicative interaction. Age, gender, ethnicity, and serious medical illness were included as covariates.
Results
Demographic characteristics
In brief, the 5,808 participants ranged in age from 18 to 75 years. The mean±SD age of the sample was 53.3±13.6. Fifty-eight percent (N= 3,345) were women, and 66% (N= 3,856) were married or cohabiting. A total of 3,775 participants (65%) were Caucasian, 685 (12%) were Hispanic, 569 (10%) were African American, 528 (9%) were Asian, 94 (2%) were Native American, 47 (1%) were East Indian, and 110 (2%) were of other races or ethnicities. A more detailed description of the sample has been previously reported (
14 ).
Subgroup costs
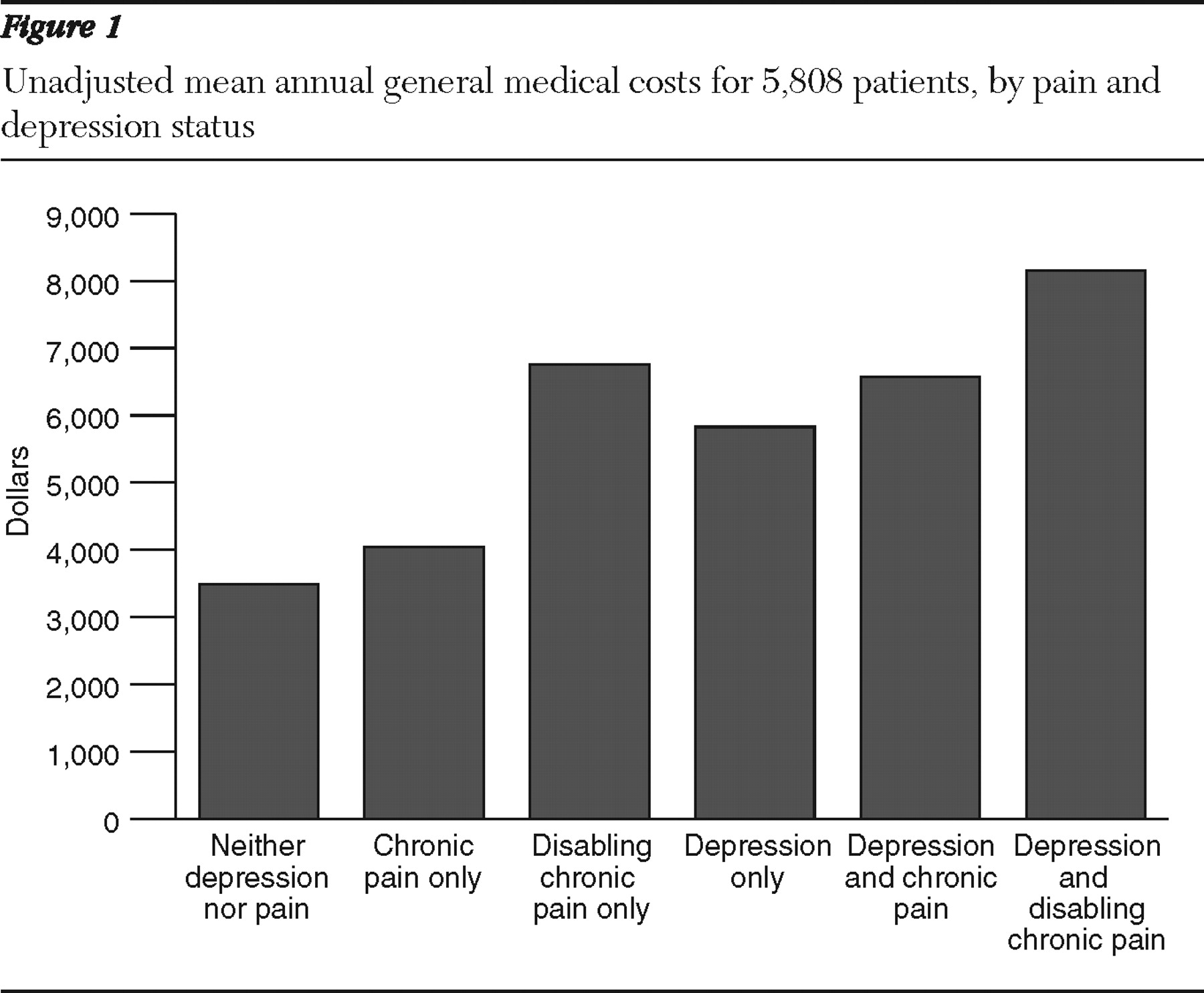
Figure 1 shows the unadjusted total cost for general medical care for the six groups. Patients with major depression and disabling chronic pain (the reference group) had the highest costs, and their costs were notably higher than those of the other two groups with major depressive disorder—those with chronic pain and those with major depressive disorder only. Costs for patients with major depressive disorder alone were lower than those for the nondepressed group with disabling chronic pain but higher than those for the other two nondepressed groups—those with chronic pain and those with neither depression nor pain.
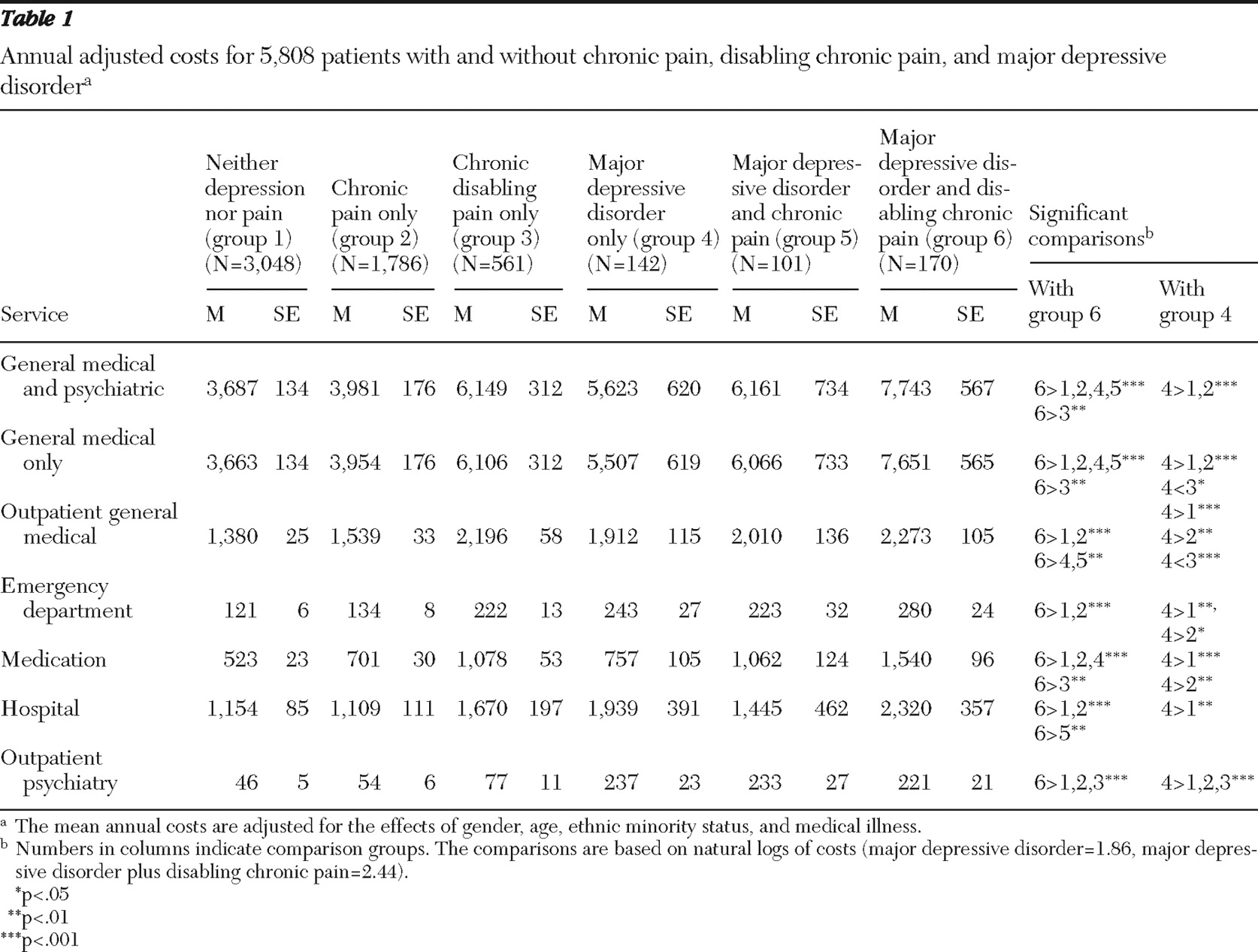
Statistically significant differences were observed between groups in adjusted total cost (
Table 1 ), in which the analysis adjusted for the effects of age, gender, racial or ethnic minority status, and medical illness (F=71, df=9 and 5,807, p<.001). Simple comparisons indicated that the reference group accrued significantly higher total costs than all five other groups (p<.001 for all comparisons, except for the comparison with the group with disabling chronic pain only, p<.01). These differences in costs remained consistent when the analyses excluded psychiatric outpatient costs (F=72, df=9 and 5,807, p<.001). In these analyses the simple comparisons also indicated that the reference group accrued significantly higher total costs than all five other groups (p<.001 for all comparisons, except for the comparison with the group with disabling chronic pain only, p<.01). Additional statistically significant differences are noted in
Table 1 .
Comparison of mean adjusted outpatient costs for general medical care, using analyses of covariance (ANCOVA), indicated a statistically significant main effect for group (F=69, df=9 and 5,807, p<.001). The reference group had significantly higher costs for outpatient medical care than all other groups with the exception of the group with disabling chronic pain only, for which the comparison indicated no significant difference. These outpatient costs for the group with major depressive disorder only were significantly lower than for the group with disabling chronic pain only (p<.001), but significantly higher than costs for the other two nondepressed groups (p<.01 for the comparison with the group with chronic pain, and p<.001 for the group with neither depression nor pain).
For adjusted emergency services costs, the omnibus ANCOVA model indicated a statistically significant main effect for group (F=20, df=9 and 5,807, p<.001). Emergency room costs were significantly higher for the reference group compared with the group with chronic pain only and the group with neither depression nor pain (p<.001 for both). However, costs for the reference group were not significantly different from costs for the groups with major depressive disorder and chronic pain, major depressive disorder alone, and disabling pain alone. Comparisons also indicated no difference between the group with major depressive disorder alone and the group with disabling pain alone. Costs for the group with major depressive disorder alone were significantly higher than for the groups with chronic pain alone (p<.05) and with neither depression nor pain (p<.01).
For adjusted medication costs, the omnibus ANCOVA model also indicated a statistically significant main effect for group (F=54, df=9 and 5,807, p<.001). The reference group had significantly higher costs than the group with major depressive disorder alone (p<.001), the group with disabling pain alone (p<.01), the group with chronic pain alone (p<.001), and the group with neither depression nor pain (p<.001); however, costs were not significantly different from costs for the group with major depressive disorder and chronic pain. Using the group with major depressive disorder alone as the reference group, comparisons indicated no significant difference between the group with major depressive disorder alone and the group with disabling pain alone. Costs for the group with major depressive disorder alone were significantly higher than for the groups with chronic pain alone (p<.01) and with neither depression nor pain (p<.001).
For adjusted hospital costs, the omnibus ANCOVA model also indicated a statistically significant main effect for group (F=13, df=9 and 5,807, p<.001). The reference group had significantly higher costs than the group with major depressive disorder and chronic pain (p<.01) and the groups with chronic pain alone (p<.001) and with neither depression nor pain (p<.001). No significant difference was found in costs for the group with major depressive disorder alone and the group with disabling pain alone. Costs for patients with major depressive disorder alone were not significantly different than for two of the nondepressed groups—those with disabling pain alone and with chronic pain alone—but they were significantly higher than costs for the group with neither depression nor pain (p<.01).
For adjusted costs of outpatient psychiatric care, the omnibus ANCOVA model was statistically significant (F=37, df=9 and 5,807, p<.001). However, we found no significant differences between the three depressed groups. Costs for both the reference group and the group with major depressive disorder alone were significantly higher than costs for all three nondepressed groups (p<.001 for all).
Results of the linear regression that used the continuous measures of pain and depression indicated statistically significant effects on total cost for pain (p=.001) and depression (p=.038) after the analysis controlled for contributions of serious medical illness and demographic variables (gender, age, and race-ethnicity). Partial correlations from these models indicated that the largest contribution to total cost was general medical illness (partial r=.35). The contributions of depression severity and pain severity to the variance in cost were comparable (partial r=.06 and .07, respectively). No statistically significant interaction was found between continuous measures of pain and depression severity.
Discussion
We found that patients who had major depression and comorbid disabling chronic pain had higher total medical costs than the other groups of depressed patients in this study. Findings were similar when costs for psychiatric care were not included in the total. Total costs for this group were significantly higher than costs for patients with major depressive disorder and nondisabling chronic pain and for patients with major depressive disorder alone. Averaged over a two-year period, after adjustment for medical illness, total annual costs for patients with both major depressive disorder and disabling chronic pain were more than 25% higher than for patients with major depressive disorder and chronic nondisabling pain ($7,743 and $6,161, respectively) and more than 37% higher than for patients with major depressive disorder with no chronic pain ($7,734 and $5,623, respectively).
Not surprisingly, total costs for participants with both major depressive disorder and disabling chronic pain (the reference group) were also significantly higher than costs for each of the nondepressed groups. Compared with the subgroup with the lowest costs—the group with neither depression nor pain—costs for the reference group were more than 100% higher ($7,743 and $3,687, respectively). These results did not measurably change when we subtracted the costs of psychiatric treatment.
On the other hand, comparison of the group with major depressive disorder alone and the three nondepressed groups showed a more inconsistent pattern. For patients with major depressive disorder alone, total costs were significantly higher than for nondepressed participants with nondisabling chronic pain and nondepressed participants with no pain. However, total costs for the group with major depressive disorder alone were lower than those for the group with no depression but with disabling chronic pain; this difference was significant (p<.05) when outpatient psychiatric costs were removed from the total costs.
In examining components of total cost, we found that the reference group had significantly higher costs than the group with major depressive disorder alone on indices associated with routine use of services, rather than with nonroutine use. Outpatient costs for general medical care for the reference group were significantly higher than those for the group with major depressive disorder alone and for all other groups with the exception of the group with disabling chronic pain alone. Medication costs for the reference group were also significantly higher than those for the group with major depressive disorder alone and those for all other groups, except for the group with major depressive disorder and chronic pain. On the other hand, hospital costs did not differ significantly between the reference group and the group with major depressive disorder alone. Although the reference group had the highest emergency room costs, the differences were significant only for comparisons with the two lowest-cost groups—those with chronic pain and those with neither depression nor pain; the same pattern was observed when the group with major depressive disorder alone was compared with the two lowest-cost groups.
Analyses of continuous measures of pain and depressive symptoms also indicated that high severity levels of both conditions were associated with significantly increased costs. However, the interaction between cost and graded severity of chronic pain and of depression was not significant, suggesting that the relationship of depression severity and pain severity with annual total costs is not multiplicative (synergistic). This finding is not consistent with results reported for primary care patients in an urban practice (
33 ), in which the interaction between major depressive disorder and pain-related impairment was found to be significantly associated with health care charges. The multiplicative relationship between pain and depression in that study occurred specifically among patients with severity levels indicative of major depressive disorder and at least moderate pain. Only pain that is moderate to severe, impairs function, or is refractory to treatment has been found to be associated with more severe depressive symptoms and worse depression outcomes (
34 ). This may be true for costs as well. Our results suggest that the higher cost observed among patients with depressive symptoms and disabling chronic pain resulted from the additive costs of having both conditions. However, given the inconsistency between our regression models and those reported by Gameroff and Olfson (
33 ), the nature of the interaction of cost with pain and depression—additive versus multiplicative—warrants further investigation.
Our sample appears to be comparable to those in other studies that have compared medical costs of patients with and without depression that did not examine subgroups. Specifically, the mean cost for patients with depression was $6,627 per year, compared with a cost of $4,040 for patients without depression. Studies comparing the costs for patients with and without depression have generally found that costs for the former group are 1.5–2 times higher (
13,
35 ).
Our criteria for the presence of chronic pain were consistent with those recommended by the International Association for the Study of Pain (
14,
29 ). We found that chronic pain was present in approximately 45% of the sample (2,618 of 5,808 participants). These findings are comparable to those of other studies that used similar criteria (
30 ). However, for patients who did not have significant disability, we found that chronic pain was not associated with meaningful differences in cost. Rather, the significant increments in cost were associated with depression and with chronic pain that was disabling. Thus identification of depressed patients in primary care settings who are likely to use the highest level of medical services will necessitate assessing disability as well as depression and chronic pain.
These findings are generally consistent with those of a small number of other studies that have examined general medical costs of individuals with both depression and chronic pain. Three studies have used self-report data to estimate costs in this subgroup. In a household survey of individuals aged 50 to 61 (
36 ), estimates of total general medical costs for those with depression and severe pain were higher than for those with depression and mild or moderate pain; the latter group's total costs were higher than for a group of individuals with depression alone. A similar stepwise pattern in these three groups was also reported among individuals aged 55 to 65 (
37 ). In a population-based study, Bao and colleagues (
38 ) reported that among individuals with major depression or dysthymia, those with comorbid pain reported a 20% greater number of physician visits than those without pain. Our findings of higher costs for patients with major depressive disorder and disabling pain than for patients with major depressive disorder and nondisabling pain or no pain are consistent with results reported by Gameroff and Olfson (
33 ). They reported that patients who had major depressive disorder and high pain interference had significantly higher total medical costs than patients who had major depressive disorder and low pain interference.
Several limitations should be considered when interpreting our findings. First, although our cost data include costs from both the year before and the year after the individual's enrollment in the study, our data on pain, depression, and disability are cross-sectional. Thus the duration and persistence of these clinical indices are unknown, as are the temporal relationships among them. Second, our assessment of depression was based on self-report rather than on a diagnostic interview. On the other hand, the prevalence of major depressive disorder among our participants was similar to that in a previous sample from the same HMO (
39 ) that was selected by use of a modified version of the Structured Clinical Interview for DSM-III-R (
40 ). Third, our assessment of pain and disability was also based on self-report measures. The extent to which patient reports of pain and functional limitations correspond to true impairment is variable. Fourth, our sample comprised HMO members who had recently visited their physician, 65% of whom were Caucasian, and two-thirds of whom were married or cohabiting. The extent to which our findings may generalize to insured or HMO patients in general, to individuals who are not seeking help, or to uninsured persons is unclear. On the other hand, our findings are similar to those reported by Gameroff and Olfson (
33 ) in a primary care sample of patients with low incomes who were primarily immigrants; in this sample of 1,028 persons 88% were Hispanic, most were insured through Medicaid, and only 21% were married or cohabiting.
Fifth, the response rate to our survey was 54%. Overall, survey respondents were older and more likely to be female (
14 ). We cannot rule out the possibility that respondents differed from nonrespondents on measures of clinical interest. Finally, although our adjustment for medical morbidity was based on physician diagnoses, as opposed to previous studies in this area that relied on self-report data (
33,
36,
37,
38 ), the list of general medical illnesses accounted for was far from exhaustive and did not include some of the most common, long-term, disabling-pain conditions found in clinical populations; therefore, it did not fully account for between-group variance in medical morbidity. Moreover, as Simon and Katzelnick (
13 ) noted, although self-report measures of general medical illness in depressed populations are subject to bias associated with depressed mood, physician-based methods tend to be less sensitive.