In this first large survey of psychiatrists' attitudes toward shared decision making, more than half reported regularly using a participatory style of decision making in schizophrenia treatment. Psychiatrists surveyed did not use a one-size-fits-all approach but clearly tailored their participatory approaches toward patients and decision topics that they believed to be suitable for shared decision making.
Approval of shared decision making in schizophrenia treatment
The approval of shared decision making in our sample can be seen as surprisingly high considering the strong tradition of paternalistic decision making in medicine and psychiatry (
19 ), and it might reflect a change toward more participatory approaches in medical decision making. The generally high approval of shared decision making might also explain why psychiatrists' characteristics were not associated with whether they tended to approve of shared decision making, as has been shown in previous studies (
9 ).
However, psychiatrists clearly tailored their participatory approaches to patients and decisions they believed to be suitable for shared decision making. Thus in our sample the use of shared decision making was judged appropriate for patients who exhibited insight, were well informed, or explicitly demanded participation. Additionally, psychiatrists saw shared decision making as a promising approach for patients who have exhibited poor compliance or have reservations about their current antipsychotic treatment. It is possible that a participatory approach with these patients is seen as an attempt to convince patients to accept antipsychotic medication.
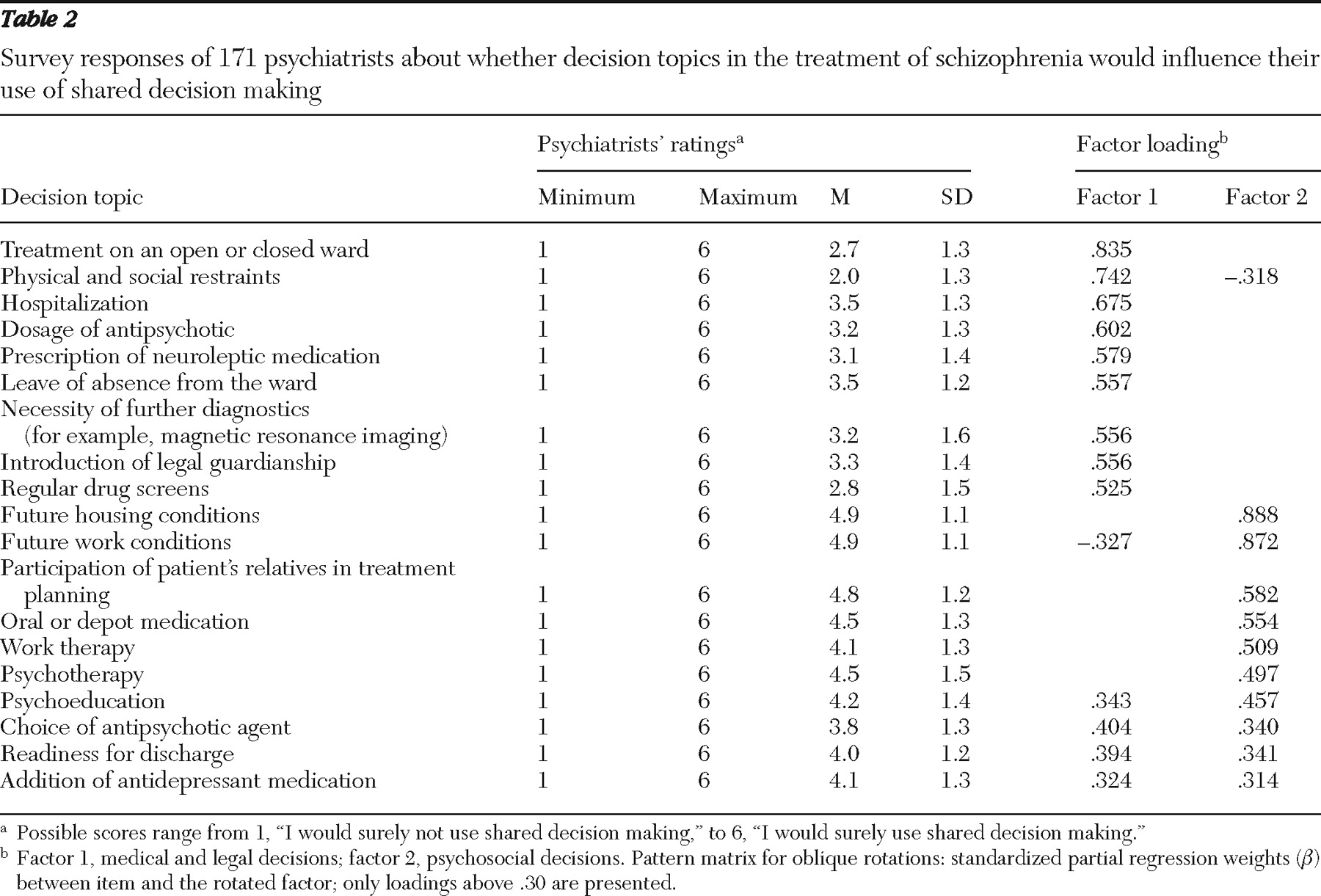
Beyond certain patient characteristics, there are also decision topics that lend themselves to using a more participatory way of reaching decisions. Thus for decisions about psychosocial treatment, patient participation seems not only possible but rather necessary. Patients facing these decisions often have recovered from acute episodes, and these decisions inevitably require the positive commitment of the patient.
Despite this positive commitment to shared decision making, the survey suggested that there are quite a few obstacles to practicing shared decision making. In the case of impaired decisional capacity, psychiatrists had doubts about whether they can accept patients as competent partners in medical decisions. And for medical and legal decisions, psychiatrists had doubts about whether it is appropriate to share decisions about issues such as hospitalization, antipsychotic medication, or legal guardianship. These decisions may in many cases affect patients in acute episodes (for example, whether the patient would be treated in an open or closed ward), who at the time of the decision might have reduced decisional capacity. Furthermore, some of these decisions (for example, use of restraints) have to be made only after discussion and shared decision making have failed. Finally, decisions such as whether or not to treat with antipsychotics may, in the psychiatrists' view, have such an impact on the patient's life and the further course of illness that they fear negative consequences for the patient if they put these decisions up for discussion. Decisions concerning medical and legal issues were apparently seen mainly as the domain of an expert physician and not as a domain where both the patient and the physician decide together.
Only three medical decisions (choice of antipsychotic agent, readiness for discharge, and use of antidepressants as adjuncts) loaded on both factors, probably because they are both expert and psychosocial decisions. Thus choosing among different antipsychotics involves expert knowledge (the physicians' domain) as well as the knowledge of the person who must live with the drug and its side effects for several years.
Taking all results into account, psychiatrists reported the general desire to engage in shared decision making with most of their patients. However, they clearly looked at the individual patient and decision topic before deciding whether to share decisions. In this context, we believe that two issues deserve further discussion: the exclusion of patients with impaired decisional capacity from shared decision making and the lack of shared decision making in medical decisions.
Because shared decision making requires that patients are able to act as competent decision makers (
2 ), it is appropriate that psychiatrists do not use shared decision making with everyone but first consider the patient's decisional capacity. Here our results support the findings of a qualitative study of psychiatrists in England, in which psychiatrists showed a strong preference for a cooperative therapeutic alliance with patients with schizophrenia, but they also considered patient competence as a critical obstacle to participatory approaches (
13 ).
With regard to patients' decisional capacity, research on this issue in fact has shown that patients with schizophrenia often show poorer decisional capacity than persons without any physical or mental conditions (comparison group) (
14 ). This poor performance of patients with schizophrenia, however, did not reflect an enduring inability. The performance of most patients with schizophrenia was equal to that of persons in the comparison group when they received an additional (educational) intervention that allowed them to review and reflect on the information necessary to consent to treatment (
14 ).
In addition, a trial of the feasibility of shared decision making with acutely ill patients with schizophrenia revealed that although psychiatrists were often in doubt about their patients' decisional capacity (
20 ), shared decision making was highly appreciated by both patients and psychiatrists and showed the potential to improve long-term outcomes (
20,
21 ).
Thus the obstacles to shared decision making reported in our survey might not be unchangeable (which stigmatizes patients), but our findings should prompt additional interventions that help patients become more capable of sharing decisions. Here, the use of psychoeducation, decision aids (
22 ), and communication skills programs (
23 ) and individual preparation of patients for decisions (
24 ) might allow reasonable engagement of many patients in medical decisions, when they otherwise would have been judged as not being able to share in decision making.
With regard to the lack of shared decision making relating to medical decisions (for example, hospitalization and drug dosage), psychiatrists should keep in mind the potential negative consequences of not engaging patients in these decisions. Most of the disagreement between psychiatrists and patients occurs in these decisions. Many patients indicate that they would make these decisions differently when deciding alone (
15 ). In addition, negative experiences (for example, not being given the option to make decisions) in acute episodes often predict patients' attitudes toward treatment for a long time afterward (
25 ). Thus decisions made without patient participation (in a paternalistic manner) are at high risk of being reversed once the acute episode is over, which may have a negative influence on the long-term course of the illness.
Limitations
It is a limitation of our approach that we relied on psychiatrists' self-reports, because self-report about the use of shared decision making may reflect preferences rather than actual behavior, which is often determined by barriers such as time constraints rather than by any preferences for a participatory decision style (
7 ). Hence self-reports often indicate higher rates of shared decision making (
4 ) than observational studies show (
26 ). Accordingly, the approval for shared decision making in schizophrenia treatment might be lower in clinical practice, and social desirability might have prevented some doctors from expressing even more explicit reservations about shared decision making.
In addition, in clinical practice psychiatrists do not respond to isolated characteristics when deciding about shared decision making, as they did in our survey, but rather they are confronted with a more complex situation (for example, a patient with reduced decision capacity facing a psychosocial decision).