Evidence that prenatal infection plays a role in schizophrenia is increasing
(1). Previous investigations have reported associations between schizophrenia and second-trimester influenza
(2), rubella
(3), respiratory infection, polio, measles, and varicella-zoster
(4). If there is a relation between schizophrenia and multiple infectious agents that differ in their antigenicity, modes of transmission, and teratogenic potential, it is likely that they share some pathogenic mechanism. Cytokines, a family of soluble polypeptides, could play an important role in this mechanism
(5). These molecules are critically important to the immune response, acting as the systemic mediators of the host response to infection
(6). Cytokine elevations increase vulnerability to developmental brain damage and other reproductive outcomes
(7–
9). A second reason to examine prenatal cytokines is that many noninfectious exposures are associated with both cytokine abnormalities
(10) and schizophrenia
(11–
13).
In the present study, we related cytokine levels from stored prenatal serum specimens to schizophrenia in the offspring. We focused on four cytokines—interleukin-8 (IL-8), interleukin-1β (IL-1β), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α). This selection was based on the reliability of these cytokines as markers of the infectious/inflammatory response and on their associations with in utero infection and brain abnormalities
(7,
8,
14–16).
Among these four cytokines, we had a particular a priori interest in investigating IL-8, for two reasons. First, maternal serum levels of IL-8 are associated with histologic chorioamnionitis in infants born at term
(17). Second, unlike the other cytokines, a significant correlation between maternal and neonatal serum IL-8 levels has been demonstrated
(17).
Based on the second-trimester specificity of prenatal infection in previous studies of schizophrenia, we tested the hypothesis that maternal second-trimester cytokine levels would be higher among pregnancies resulting in offspring who developed schizophrenia than among pregnancies of matched comparison subjects. We used the birth cohort of the Prenatal Determinants of Schizophrenia study
(18). Serum samples were prospectively drawn during pregnancy in virtually all mothers of cohort members, permitting direct bioassay of these cytokines.
Method
The study protocol was approved by the institutional review boards of the New York State Psychiatric Institute and the Kaiser Foundation Division of Research.
Description of the Cohort
The Prenatal Determinants of Schizophrenia study has been fully described previously
(18) and will therefore be summarized briefly. The mothers of the cohort members in the Prenatal Determinants of Schizophrenia study were enrolled from 1959 to 1967 in the Child Health and Development Study
(19). The Child Health and Development Study recruited nearly all pregnant women receiving obstetric care from the Kaiser Foundation Health Plan in Alameda County, Calif. The membership of the Kaiser Foundation Health Plan was demographically similar to the population of that region
(20).
The Prenatal Determinants of Schizophrenia study cohort consisted of the subsample of 12,094 live births who were members of the Kaiser Foundation Health Plan from Jan. 1, 1981, through December 31, 1997. Kaiser registries provided a record of each subject’s membership and psychiatric treatment status over this 17-year interval. Hence, these dates correspond to the period of case ascertainment; we chose 1981 as the beginning of ascertainment because computerized records did not exist in the Kaiser Foundation Health Plan before that date. Subjects were eligible for the study if they were members of the Kaiser Foundation Health Plan at least until 1981. The youngest subjects with schizophrenia were ascertained at age 14 years, and the oldest at age 38. The demographic characteristics of the sample were similar for subjects who remained in the Kaiser Foundation Health Plan after age 10 and those who left the health plan before age 10
(18).
Collection of Maternal Sera
Maternal serum samples were collected in virtually all pregnancies, immediately frozen at –20°C, and archived at that temperature or below since the blood draws. The mothers of all cohort members provided consent for human investigation at the time of each blood draw. Because informed consent procedures differed during the period of the pregnancies (1959–1967) from those in use today, only verbal consent was required. At that time, the mothers were informed that the serum samples were to be stored for future use in a wide variety of studies, many of which had not been developed. Under current federal regulations, this category of research activity is exempt from the requirements relating to informed consent. Therefore, consent for use of the serum specimens was not obtained from offspring.
Ascertainment and Diagnosis of Schizophrenia Spectrum Disorders
Schizophrenia spectrum disorders were defined as schizophrenia, schizoaffective disorder, delusional disorder, psychotic disorder not otherwise specified, and schizotypal personality disorder
(21). Case ascertainment occurred by means of computerized record linkage between Child Health and Development Study and Kaiser Foundation Health Plan identifiers. Inpatient, outpatient, and pharmacy registries were used. Subjects with schizophrenia or potential schizophrenia spectrum disorders were screened from registry diagnoses ICD 295–299 or medical records indicating antipsychotic medications, followed by psychiatrist review of all records. Among those who screened positive (N=183), 13 were deceased. We contacted 146 (86%) of the 170 remaining potential subjects with schizophrenia for diagnostic interviews.
Potential subjects with schizophrenia were administered the Diagnostic Interview for Genetic Studies
(22) by clinicians with at least a master’s degree in a mental health field who were trained to reliability. All interviewed subjects provided written informed consent for human investigation. Psychiatric diagnoses (DSM-IV) were made by consensus of three experienced research psychiatrists on the basis of the Diagnostic Interview for Genetic Studies information and medical records. Given that schizophrenia spectrum disorders are rare in subjects without a history of ICD 295–299 or treatment with antipsychotic medications, clinical review was not performed on cohort members who were not identified as potential subjects with schizophrenia. One hundred seven of the 146 contacted potential subjects with schizophrenia (73%) completed the Diagnostic Interview for Genetic Studies. Chart review by experienced psychiatric/psychological clinicians, with confirmation by a research psychiatrist, was used to diagnose the 76 potential subjects with schizophrenia who were not available for interview.
These procedures yielded 71 total subjects with schizophrenia and other schizophrenia spectrum disorders (44 received the Diagnostic Interview for Genetic Studies, 27 were diagnosed by chart review). The diagnoses were schizophrenia (N=43), schizoaffective disorder (N=17), delusional disorder (N=1), schizotypal personality disorder (N=5), and other schizophrenia spectrum psychosis (N=5) (this last category was assigned to subjects with either schizophrenia or schizoaffective disorder for whom insufficient information was available to definitively diagnose the specific condition).
Statistical Analysis
The analysis was based on a nested case-control design
(23) in which the comparison subjects for each case were selected to represent the population at risk when the case was ascertained. In the Prenatal Determinants of Schizophrenia study, subjects with schizophrenia were ascertained on the first date of medical attention for schizophrenia spectrum disorders, as recorded in the Kaiser Foundation Health Plan inpatient, outpatient, or pharmacy registries.
Subjects and Matching Procedure
Among the 71 subjects with schizophrenia spectrum disorders, 65 had at least one available prenatal serum sample. Of these, 59 had prenatal sera available from the second trimester or (generally early) third trimester. (In order to maximize the sample size, some subjects with sera from the third but not the second trimester were included. These samples are referred to as “second/third trimester.”) Further trimester-specific analyses were also conducted.
Eligible comparison subjects (N=10,768) were selected from offspring in the Prenatal Determinants of Schizophrenia cohort after excluding siblings of subjects with schizophrenia spectrum disorders, subjects with major affective disorders, and subjects without prenatal sera.
We initially selected up to eight comparison subjects per subject with schizophrenia spectrum disorder. Comparison subjects were matched to subjects with schizophrenia on membership in the Kaiser Foundation Health Plan at the time the case was ascertained in terms of date of birth (within 28 days), gender, and number and timing (within 28 days) of maternal blood samples taken during the index pregnancy
(18).
To conserve the sera, two matched comparison subjects with available sera from the second/third trimester (N=118) were selected at random from the pool of matched comparison subjects for each subject with schizophrenia spectrum disorder. To match closely for gestational timing, we further required that matched comparison sera be drawn within 6 weeks of the case sera, leading to the exclusion of one comparison subject for some matched sets. This selection process resulted in 105 matched comparison samples for the main analysis.
Laboratory Assay
All procedures were conducted blind to diagnosis of the offspring and were carried out under Level II biohazard containment conditions. Each serum specimen was thawed and made 2 mM with respect to phenylmethylsulfonyl fluoride, a protease inhibitor, to prevent degradation of cytokines by serum proteases. Measurement of IL-8, IL-β, IL-6, and TNF-α in serum was by sandwich enzyme-linked immunosorbent assay. Matched antibody pairs (OptEIA sets) were obtained from BD Pharmingen (San Diego). F(ab) 2 fragments of both capture and detection antibodies were used to avoid interference by rheumatoid factor or heterophilic antibodies in the test sera. The relevant capture antibody was bound to the wells of treated microplates (Costar Easywash, Cambridge, Mass.) by adsorption at 4°C overnight. All subsequent procedures were carried out at room temperature.
After the plates had been washed extensively, a dilution series of a known concentration of the relevant cytokine (standard) and appropriate dilutions of the serum samples were placed in wells and incubated for 2 hours. Each plate contained a standard series. The plates were again washed, biotinylated detection antibody was added to each well, and the plates were incubated for a further 2 hours. Following a third wash, streptavidin-horseradish peroxidase was incubated in each well for 30 minutes. After another wash, enzyme substrate (tetramethylbenzidine) was added for a further 30 minutes, and the reaction was stopped with acid. The absorbance of the colored product was measured at 450 nm on a Molecular Devices V Max automated microplate reader (Sunnyvale, Calif.), and the data were analyzed with in-house computer programs written for the SigmaPlot 2000 graphing program (SPSS, Chicago).
The concentration of each cytokine in the sample was obtained by interpolation from the standard curve that took into account the dilution of the sample. Results were expressed as pg cytokine/ml serum. The lower limits of sensitivity for the assays (pg/ml) were as follows: IL-1β: 4, IL-6: 5, IL-8: 3.1, and TNF-α: 8.
Analytic Strategy
Matching by the nested case-control design ensured that each subject with schizophrenia spectrum disorder and the corresponding comparison subjects were followed for equal lengths of time from birth until first treatment for schizophrenia spectrum disorder. We fitted a univariate conditional logistic regression model
(24) to estimate the unadjusted association between schizophrenia spectrum disorders and each cytokine. For the main analyses, the regression coefficients, their standard errors, likelihood ratio chi-square test, and p values are reported. Statistical significance was judged at alpha=0.05.
We then assessed the potential effects of confounding on the results. We considered the following covariates as potential confounders: maternal age (<35 [reference] or ≥35); maternal ethnicity (white [reference], black, or other); socioeconomic status, defined as maternal education (less than high school, high school [reference], some college, or college degree); maternal smoking (during pregnancy or until aware of current pregnancy versus never smoked before pregnancy [reference]); and gestational age of the sample (to confirm adequate adjustment by our matching criteria). The adjusted association between schizophrenia spectrum disorders and the cytokines was assessed by using conditional logistic regression models.
Results
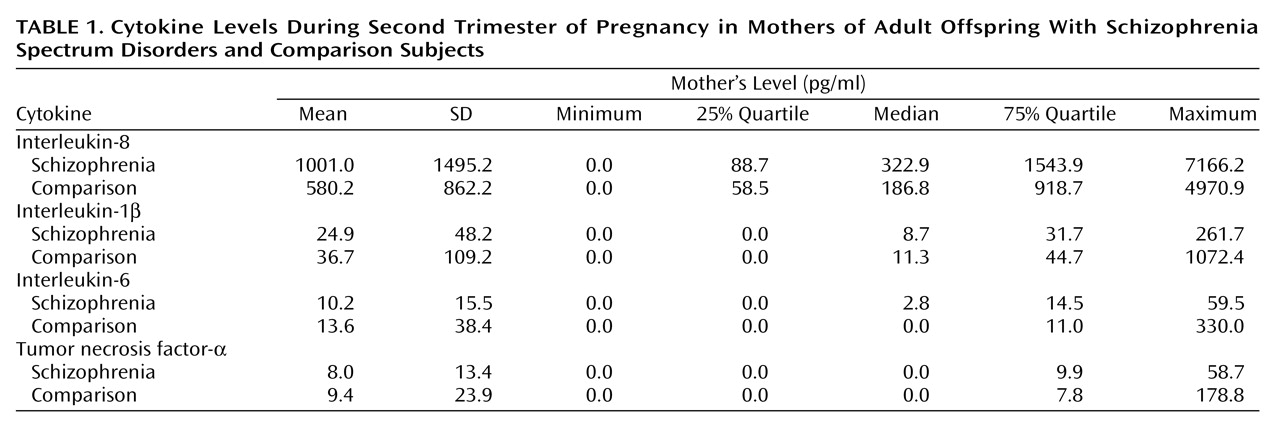
Both the mean and median levels of maternal second/third-trimester IL-8 were nearly twice as high in the mothers of offspring who developed schizophrenia spectrum disorders than the mothers of matched comparison subjects (
Table 1). The 25th and 75th quartile IL-8 levels of mothers of offspring with schizophrenia spectrum disorders were also higher than those of mothers of comparison subjects (
Table 1), indicating that the distribution of IL-8 levels was shifted upward throughout the range of levels of this cytokine. There were no appreciable differences in the means or distributions of second-trimester IL-1β, IL-6, or TNF-α between mothers of offspring with schizophrenia spectrum disorders and mothers of comparison subjects.
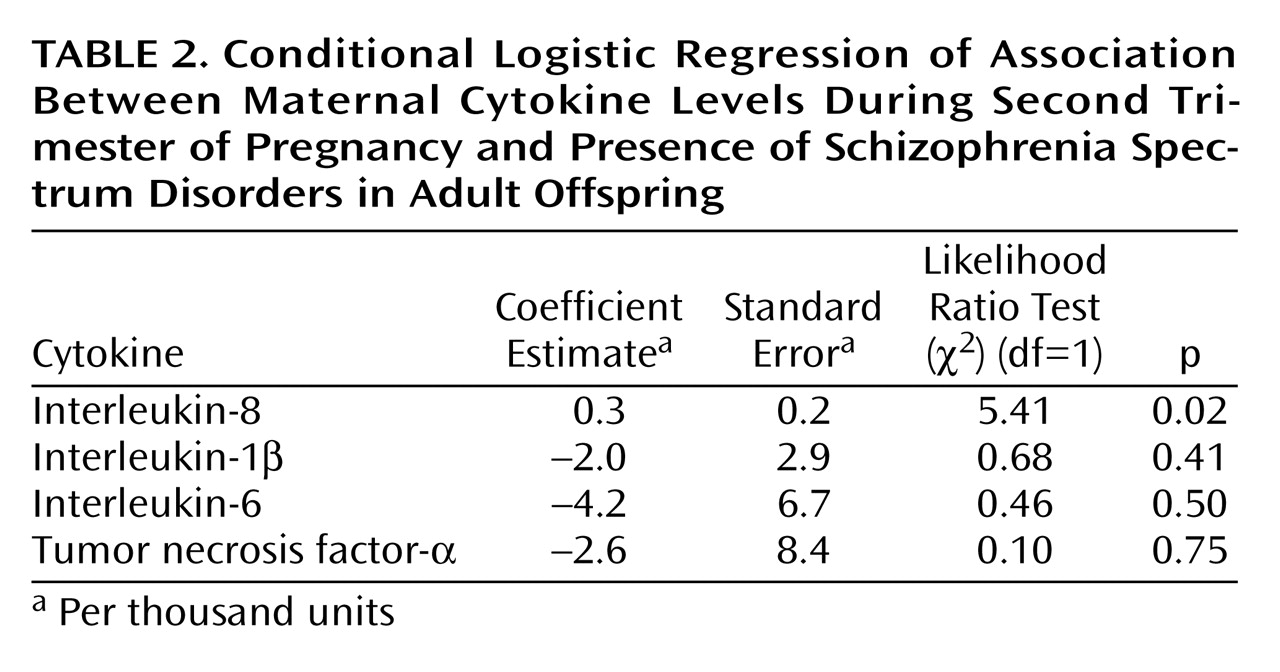
Among the cytokines tested, maternal second/third-trimester IL-8 was significantly associated with risk of schizophrenia spectrum disorders in the offspring (likelihood ratio test χ
2=5.41, df=1, p=0.02) (
Table 2). There were no statistically significant differences between subjects with schizophrenia spectrum disorders and matched comparison subjects with regard to maternal second-trimester IL-1β, IL-6, or TNF-α (
Table 2).
For further confirmation, we conducted three additional analyses. First, we restricted the main analysis to serum samples from the second trimester only (i.e., all third-trimester samples were excluded). There was no change in the effect of maternal IL-8 level on schizophrenia risk (likelihood ratio test χ2=4.34, df=1, p=0.04). No effects were observed for IL-1β, IL-6, and TNF-α (results available on request). Second, we excluded subjects with schizophrenia spectrum disorder diagnoses other than schizophrenia. Similar to our findings for schizophrenia spectrum disorders, we found significantly higher levels of IL-8 among individuals diagnosed with schizophrenia (likelihood ratio test χ2=4.12, df=1, p=0.04), and no significant associations between IL-1β, IL-6, and TNF-α and schizophrenia. Third, in a separate analysis of third-trimester IL-8 and risk of schizophrenia spectrum disorders, we found no evidence of a relation with risk of schizophrenia spectrum disorders (likelihood ratio test χ2=0.10, df=1, p=0.75), although the power to detect an association was low given the small number of matched sets (N=8) in this analysis.
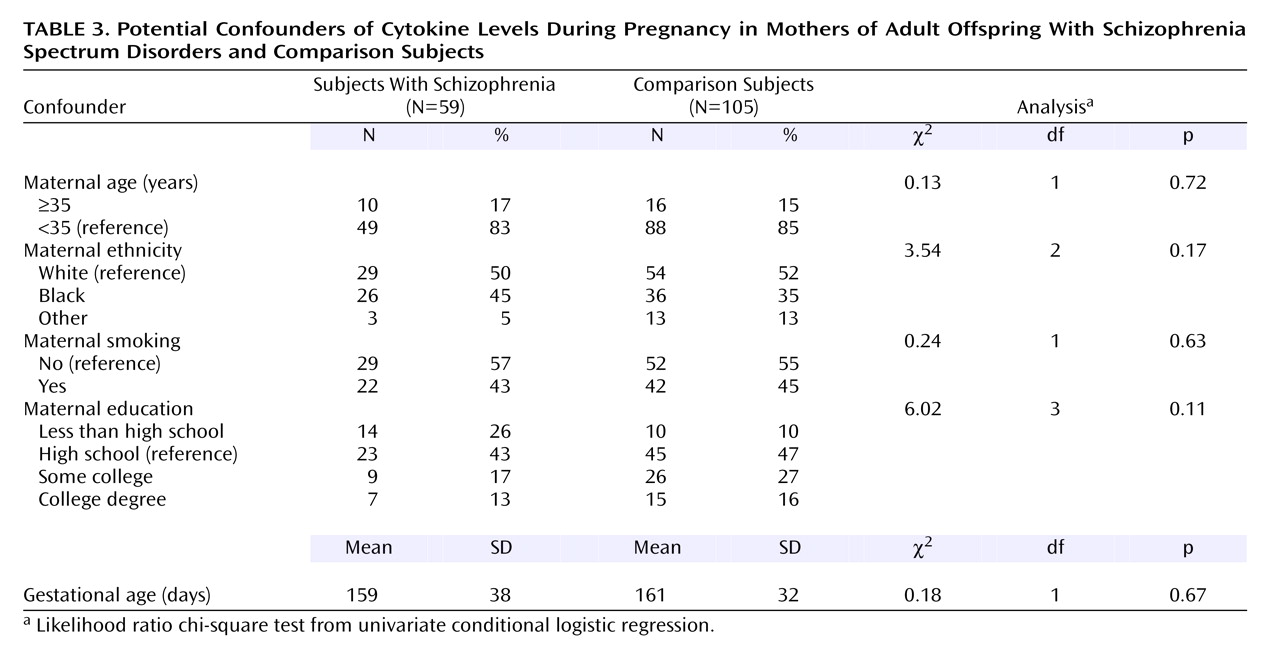
Subjects with schizophrenia spectrum disorders and comparison subjects did not differ with regard to the following maternal covariates: age, race, smoking, and gestational age of the serum samples (
Table 3). The rate of low maternal education (less than high school) was somewhat greater in subjects with schizophrenia spectrum disorders. It should also be noted that the subjects with schizophrenia and comparison subjects were matched on several key variables (see Subjects and Matching Procedure in the Method section).
Nonetheless, for further assurance, we adjusted for maternal ethnicity, education, smoking, and gestational age in an additional analysis of maternal IL-8 and schizophrenia spectrum disorders. The results remained statistically significant after adjustment for these covariates (likelihood ratio test χ2=3.94, df=3, p=0.05).
Discussion
We have demonstrated a significant association between mean second-trimester serum levels of IL-8 in mothers of offspring who developed schizophrenia spectrum disorders compared with mothers of matched comparison subjects who did not develop schizophrenia. IL-8 is an 8 kDa protein and a member of a family of soluble molecules called chemokines, which are a subclass of the cytokine superfamily
(25). This chemokine plays a critical role in the immune response, including adherence of neutrophils to endothelial cells
(26), leading to their migration into tissues, and the discharge of lysosomal enzymes from neutrophils, resulting in oxygen free radicals
(27). IL-8 also has indirect chemotactic activity on T lymphocytes
(28).
IL-8 enhances the growth-inhibitory activity of neutrophils to pathogens
(29). Bacterial
(30) and viral
(31–
33) infections stimulate the production of IL-8. With regard to infections during pregnancy, higher maternal IL-8 levels have been associated with chorioamnionitis
(17). Studies suggest that maternal infection is a potential risk factor for schizophrenia
(2–
4). In previous work by our group on this same birth cohort
(34,
35), we demonstrated that maternal exposure to respiratory infection during the second trimester and to influenza during the early-to-mid-gestational period were associated, respectively, with twofold and threefold higher risks of schizophrenia spectrum disorders. Hence, IL-8 may represent a marker of a maternal infection that increases vulnerability to schizophrenia.
Alternatively, elevated maternal IL-8 may be a marker of a noninfectious inflammatory process that contributes to schizophrenia risk. Elevated levels of IL-8 and other cytokines have also been demonstrated in several noninfectious conditions, including preeclampsia
(11,
36), preterm birth
(37), and elevated body mass index
(13), each of which has been associated with schizophrenia and can adversely affect fetal development
(10,
38).
The magnitude of the elevation in maternal serum IL-8 levels in schizophrenia spectrum disorders was nearly twofold. Cytokine elevations of a similar magnitude in maternal sera have been observed for the noninfectious conditions cited as well as for other maternal conditions, including chorioamnionitis
(17,
39) and missed abortion
(40).
In addition to its relevance to pathological states, IL-8 plays an important role in the physiology of pregnancy and delivery. During pregnancy, IL-8 appears to be involved in blastocyst implantation and placental development
(41). This may occur by IL-8-induced inhibition of platelet-activating-factor acetylhydrolase, resulting in increased platelet activating factor, which is known to facilitate implantation and placental growth. Choriodecidual cells from early pregnancy tissues in vitro produce large quantities of IL-8; interferon-gamma, which increases following pregnancy, appears to up-regulate the production of IL-8 in endometrial stromal cells. IL-8 is also important in the process of cervical ripening at birth
(42) and in the onset of labor
(43). Higher levels of IL-8 that occur at term are believed to soften the cervix through neutrophil activation and subsequent production of collagenases.
Other Cytokines
Since pregnancies complicated by chorioamnionic infection in the newborn are associated with higher levels of maternal IL-1β, IL-6, and TNF-α
(8,
9,
14–16), we might have also expected associations with schizophrenia; yet none were observed. There are several potential explanations. First, most studies linking elevated maternal levels of IL-1β, IL-6, and TNF-α with intrauterine infection were based on measures of these cytokines in nonserologic specimens, such as amniotic fluid. One study
(17) did not show an elevation of these other maternal cytokines in term pregnancies complicated by chorioamnionitis.
Second, with regard to TNF-α, the median levels in our study were generally lower than those reported in pregnant comparison subjects from some previous serologic studies
(17,
39). This may have blunted differences between subjects with schizophrenia and comparison subjects. With regard to IL-6, the median levels were comparable to or higher than those observed in previous studies
(39), although some studies
(44) demonstrated higher median levels than we observed in our study. For IL-1β, the median levels in our study were either comparable to
(17,
44) or greater than
(37) corresponding levels from previous studies.
A third potential explanation for the specificity of the IL-8 finding is the fact that it belongs to the more specific class of cytokines termed “chemokines.” Possibly, the unique properties of IL-8, such as potent neutrophil attraction and activation, may lead to developmental brain anomalies involved in the pathogenesis of schizophrenia.
A study based on the Collaborative Perinatal Project
(12) also found a trend for higher levels of maternal IL-8 in pregnancies of subjects destined to develop psychoses
(12). The lack of a significant IL-8 effect may have resulted from low statistical power because of a small sample. That study is not completely comparable to the Prenatal Determinants of Schizophrenia study, however, because the case sample in that cohort was somewhat more heterogeneous and the serum samples were generally drawn at the time of delivery rather than in the second trimester. One positive finding of that study
(12) was an association between higher levels of maternal TNF-α and psychosis in offspring. This discrepant finding may have resulted from elevated TNF-α levels in nonschizophrenia psychotic disorders, but this appears unlikely because the number of such cases was relatively small compared with the entire sample.
Limitations
The sera in the present study had been frozen for more than 30 years. Possibly, storage for this lengthy period may have altered the cytokine levels. Several factors may militate against this possibility. First, careful visual inspection of our samples and consultation with the lead Child Health and Development Study investigators (personal communication) revealed no evidence of previous freeze-thawing. Second, the comparison subjects were matched to subjects with schizophrenia spectrum disorders on date of birth and gestational timing, and the samples were uniformly handled and stored, suggesting that storage time should not have biased the associations. Third, the levels of IL-8 and IL-1β in the present study were robust, and our IL-6 levels were comparable to or greater than levels found in several previous studies (see preceding discussion). Although serum levels of TNF-α were generally lower than those found in most previous studies, these investigations varied widely among each other with regard to the magnitude of TNF-α levels.
Second, the cytokine response is governed not only by environmental insults but also by genetic factors. The present study did not include sufficient data on family history to permit an analysis of genetic vulnerability and prenatal cytokines.
Conclusions
The present study supports the hypothesis that higher levels of second-trimester IL-8 are associated with a greater risk of schizophrenia. There are two possible explanations for this finding. First, in utero infection may have led to the elevation of IL-8 in mothers of subjects who developed schizophrenia spectrum disorders. Second, a noninfectious exposure associated with a pro-inflammatory cytokine response may have been responsible. Further work is essential to clarify the relationship between prenatal insults associated with elevated cytokines and schizophrenia; for example, the preservation of placental tissue would permit the investigation of the contribution of inflammatory processes such as chorioamnionitis to schizophrenia risk. Nonetheless, these findings suggest a promising avenue of exploration that may ultimately facilitate the prevention of schizophrenia and reveal its etiopathogenic mechanisms.