Puberty is a biologically driven developmental transition with complex secondary effects on social, emotional, and sexual development (
1). Interindividual variation in the timing of pubertal processes creates a period of contrast in which same-aged girls differ significantly with respect to highly salient physical attributes such as breast size, distribution of subcutaneous fat, hip-to-waist ratio, and body hair. Girls who mature earliest are at greater risk for a range of psychological, behavioral, and social problems in adolescence, including higher rates of conduct problems (
2–6), substance-related problems (
3,
4,
7,
8), and precocious sexuality (
5,
9,
10). Most of the evidence also suggests increased risk for adolescent depression, anxiety, and general emotional distress (
4,
11–14), but the evidence is mixed in relation to educational outcomes (
15–18). This period of increased risk persists across adolescence even after later-developing peers have physically matured (
4,
10,
11). It is uncertain, however, whether this period of risk persists into young adulthood, when almost all young women have been physically and sexually mature for some years.
Various hypotheses have been proposed concerning the longer-term outcomes of early puberty, but few studies have the necessary longitudinal data to test them. The persistence hypothesis postulates that negative outcomes of early puberty in adolescence (early sexual initiation, substance use, and delinquent behavior) are self-propagating and continue unabated into young adulthood. The evidence, however, better supports what we call the selective persistence hypothesis.
According to the selective persistence hypothesis, extricating oneself from a pattern of adolescent behavioral problems is a protracted process for early maturers. Failures in limited areas (social, educational) may persist even after recovery from behavior problems (early delinquency; precocious or risky sexuality) (
19–21). Early maturation may orient girls toward early motherhood, with limited educational and occupational prospects, and increase their risk for emotional and substance-related psychiatric outcomes. The most extensive analysis of the long-term impact of early maturation (
5) supported the selective persistence hypothesis: Early-maturing girls ceased to have behavior problems in adulthood, including criminal offenses and substance use, but they nevertheless had more children than their same-sex peers by age 25, and there was some evidence of lower educational and occupational attainment. An earlier cohort study (
22) showed similar effects on age at marriage and first conception. These studies did not formally assess psychiatric status, however. The selective persistence hypothesis also raises the possibility that long-term effects may be apparent only for early maturers with the most serious problems or those with long-lasting negative consequences (e.g., teen parenthood).
The
attenuation hypothesis posits that the effects of early maturation will be most pronounced immediately after the period of early development but that these effects will attenuate by young adulthood because early maturers recover from the adverse effects of early pubertal timing and/or on-time and late maturers catch up in their physical development and now display similar adult-typical behaviors, particularly status-related behaviors, such as alcohol use or involvement in sexual activities. This hypothesis was supported by the young adult follow-up of the Oregon Adolescent Depression Project (
23), which revealed no effect of early maturation on current young adult psychopathology or role attainment and only modest effects on the quality of social networks, but elevated lifetime rates of depression, anxiety, and disruptive behavior disorders, suggesting that early maturers had recovered. Similar attenuated effects in young adulthood were observed in a study using data from the National Longitudinal Study of Adolescent Health (
12), which looked at levels of depressed mood over time. Both studies, however, employed pubertal timing measures that were largely retrospective—assessed after most girls had already reached maturity—rather than direct measurement of pubertal milestones throughout the pubertal transition.
Reviewing the literature on early-maturing girls in 1990, Stattin and Magnusson (
5) noted a “scarcity of systematic studies addressing the issue of long-range impact” (p. 301). At present, almost 20 years later, only one additional study (the Oregon study mentioned above) has examined a range of outcomes in early-maturing girls in adulthood. Thus, conclusions about the long-term effects of pubertal timing are based largely on studies of subjects born over 50 years ago (
15,
24).
Our aim in this study is to assess the long-term effects of pubertal timing on outcomes related to crime, substance use, education and socioeconomic status, sexual behavior, and mental health in cohorts born after 1980.
Method
Participants
The Great Smoky Mountains Study is a longitudinal study of the development of psychiatric disorders in rural and urban youths (
14–19). A representative sample of three cohorts of children, ages 9, 11, and 13 at intake, was recruited from 11 counties in western North Carolina using a household equal probability accelerated cohort design (
20). The externalizing problems subscale of the Child Behavior Checklist (
25) was administered to a parent of the first-stage sample (N=3,896). All children whose scores were in the top 25%, plus a 1-in-10 random sample of the rest, were recruited for detailed interviews. Ninety-five percent of families contacted completed the telephone screen. About 8% of the area residents and the sample are African American, and fewer than 1% are Hispanic; American Indians make up only about 3% of the study area but were oversampled to constitute 25% of the sample. All participants were given a weight inversely proportional to their probability of selection, so that the results are representative of the population from which the sample was drawn. Of all youths recruited, 80% (N=1,420) agreed to participate. The sample was 49% female (N=630).
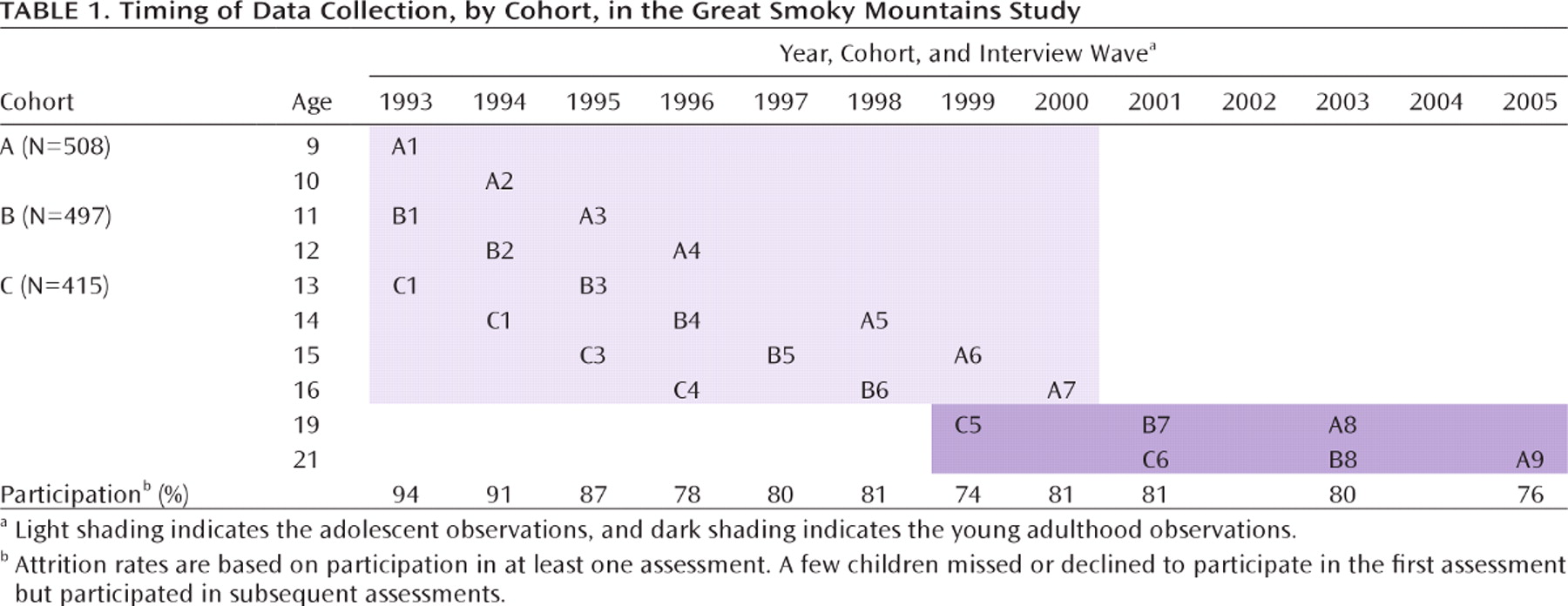
Table 1 presents the study design and participation rates at each wave. In this article, we present data on 4,021 parent-daughter pairs of interviews carried out across an age range of 9 through 21.
Procedures
The parent and participant were interviewed by trained interviewers separately (as close as possible to the participant's birthday) until participants were 16; at ages 19 and 21, participants were interviewed, but not their parents. Before the interviews began, the parent and child signed informed consent forms approved by the Duke University Medical Center Institutional Review Board. Each parent and child was paid for their participation.
Pubertal Timing
At each assessment up to age 16, self-ratings of current pubertal morphologic status based on the standard Tanner staging system (
26) (5-point scale from I [prepubertal] to V [adult]) and age at menarche were assessed. Self-ratings of Tanner stage correlate well with direct observation of pubertal status (
27,
28). For the two younger cohorts, early pubertal timing was defined as achieving Tanner stage IV (increased breast size and elevation) by age 12 (18.2% of girls). These physical changes are highly salient to the girls themselves, their family, and their peers. The oldest cohort, however, was first interviewed at age 13. Thus, girls in this group who had already achieved Tanner stage IV or V could not be unambiguously assigned to a pubertal timing group using the Tanner staging method. Instead, these girls were classified as early maturers if they reported an onset of menarche before age 11. The proportion of early maturers identified this way was similar to the proportion identified using Tanner staging. Together, 19.0% of girls (unweighted N=115) were categorized as early maturers.
Adolescent and Young Adult Outcomes
Outcome status was derived by aggregating observations across two periods: adolescence (ages 13 to 16) and young adulthood (ages 19 and 21). All adolescent data except juvenile justice status were collected through parent and child interviews with the Child and Adolescent Psychiatric Assessment (
26,
27). Parent and adolescent reports were combined using an either/ or rule for adolescent outcomes unless otherwise specified. In young adulthood, all outcomes except officially recorded criminal offenses were assessed through participant interviews with the Young Adult Psychiatric Assessment (
28). The time frame for both interviews was the 3 months preceding the interview unless otherwise stated. Our goal was to assess a range of domains of functioning within each developmental period (e.g., crime, psychiatric functioning).
Crime.
The self-report and parent-report variables used were police contact (adolescence and young adulthood), criminal charges (adolescence only), and incarceration (young adulthood only). Offenses from the North Carolina Administrative Offices of the Courts official juvenile and adult records were categorized as minor, moderate, or severe/violent (see reference 29 for definitions). Because there were few girls with severe/violent offenses, these were grouped with moderate offenses.
Psychiatric functioning and substance use.
Scoring programs written in SAS, version 9 (SAS Institute, Inc., Cary, N.C., 2004), combined information about the date of onset, the duration, and the intensity of each symptom to create DSM-IV diagnoses. The 2-week test-retest reliability of Child and Adolescent Psychiatric Assessment diagnoses in children ages 10 to 18 is comparable to that of other highly structured interviews (kappa values for individual disorders range from 0.56 to 1.0) (
27). Validity is well established using multiple indices of construct validity (
26). All adolescent and young adult disorders with a 3-month prevalence greater than 1% were included. Three-month prevalence rates for ages 9 to 16 have been published elsewhere (
30).
School/peers (adolescents only).
“Truancy” was coded if the child failed to reach school or left school at least twice without the permission of the school authorities for reasons not associated with either separation anxiety or fear of school. “Association with older peers” was coded if the majority of the participant's friends were two or more years older than the participant. “Difficulty making friends” was coded when the child reported difficulty forming or maintaining friendships. “No best friend” was coded when the child reported having no peer confidant. “Bullying peers” was coded according to the DSM-IV conduct disorder symptom.
Home (adolescents only).
“High confiict with parents” was coded if the number of reported parent-child arguments was in the top 25%. “Poor sibling relations” was coded if the participant reported high levels of confiictual interactions with any sibling. “Running away” and “curfew violations” were coded according to their DSM-IV descriptions for conduct disorder.
Sexual behavior.
Participants reported whether they had ever had sexual intercourse, and if so, the number of their sexual partners. “Multiple sexual partners” was defined as having two or more sexual partners in adolescence or 10 or more partners by young adulthood. “Pregnancy” was coded as positive for those who reported any pregnancy, regardless of whether the fetus was carried to term. “Sexually transmitted disease” in young adulthood was coded if the participant reported testing positive for herpes, genital warts, chlamydia, or HIV. Young adults also reported whether any sexual encounter involved “going home with a stranger.”
Education and socioeconomic status (young adults only).
“School dropout” was coded if the participant had not graduated from high school by age 21. Up to age 16, “low occupational status” was coded using the maximum of the parents' or participant's occupational prestige as rated by the National Opinion Research Center General Social Survey ratings. Thereafter, the maximum of the participant's or participant's spouse's rating was used. “Poverty status” was coded on the basis of thresholds issued by the U.S. Census Bureau based on income and family size (
31). “Material hardship” was coded if the participant was unable to meet basic needs, had no health insurance, had financial problems, had residential instability, or had no insurance for mental health or substance abuse treatment.
Analyses
All associations were tested using weighted logistic regression models in a generalized estimating equations framework implemented by SAS PROC GENMOD. Robust variance (sandwich type) estimates were used to adjust the standard errors of the parameter estimates for the stratified design effects. Therefore, the parameters reported here are representative of the population from which the sample was drawn. Associations between early puberty status and each outcome were tested in adolescence (ages 13 to 16) and in young adulthood (ages 19 and 21).
Missing Data
Across all waves, an average of 82% of possible interviews was completed, ranging from 75% to 94% at individual waves (
Table 1). Three or four assessments (depending on the cohort) were possible in adolescence, and two assessments were possible in adulthood. If missing assessments was associated with pubertal timing, then our analyses might be biased. Pubertal timing, however, was not associated with missing assessments overall or in young adulthood only. The overall statistical trend suggested that early maturers missed fewer assessments than their peers.
Results
Pubertal Timing and Adolescent Outcomes
Early maturation was associated with at least one indicator in each of the six adolescent outcome domains (10 of 26 specific indicators; see
Table 2) and predicted having had any problems in substance use, school/peers, and psychiatric functioning domains (one or more elevated indicators). The strongest associations (odds ratios >3.0) were seen with substance use and conduct problems.
Pubertal Timing and Young Adult Outcomes
No significant associations were observed between early maturation and any of the five young adult domains (
Table 3), suggesting that attenuation of the negative effects of early maturation was the rule. Only three of the 21 specific outcome measures were significantly predicted by early puberty; these included higher rates of lifetime sexual partners, higher rates of young adult depression, and lower levels of illicit drug abuse. Depression was the only current young adult outcome for which early maturers were at increased risk. Depression in young adulthood might reasonably be related to psychiatric status in adolescence (
32). Testing associations with both disorders that were predicted by early puberty in adolescence—conduct disorder and depression—suggested that it was adolescent conduct disorder, not depression, that accounted for the higher rates of young adult depression. An interaction term between pubertal timing and adolescent conduct disorder significantly predicted young adult depression (odds ratio=221.8, 95% CI=9.7–5094, p=0.0007), such that 9% of early maturers with no history of adolescent conduct disorder displayed depression in young adulthood, compared with 81% of early maturers reporting a history of adolescent conduct disorder. After accounting for this interaction, the main effect of pubertal timing on young adulthood depression was no longer significant (odds ratio=1.9, 95% CI=0.5–7.4, p=0.38). Overall, there was little evidence of persistent, long-term effects of early pubertal timing, with the exception of a small group of girls at greater risk for depression in young adulthood.
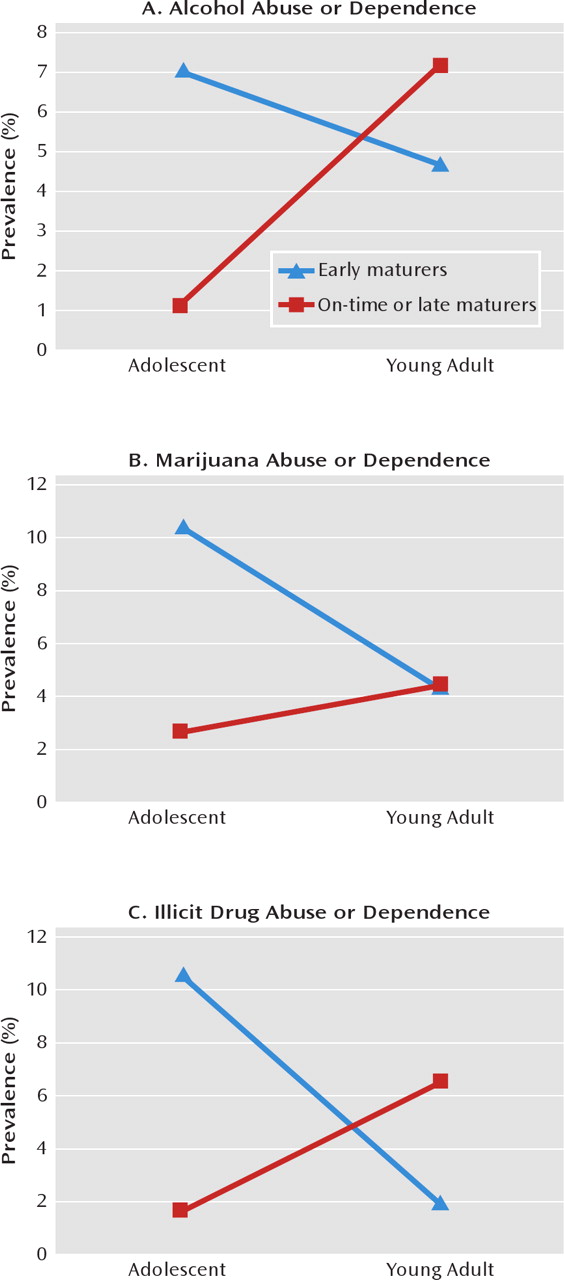
Attenuated effects might suggest either recovery by early maturers or “catch-up” by on-time and late maturers. Longitudinal analyses were conducted for indicators that were measured similarly across developmental periods (e.g., alcohol abuse or dependence, marijuana abuse or dependence, illicit drug abuse or dependence) to test whether they decreased from adolescence to young adulthood for early maturers (recovery) or increased across developmental periods for on-time and late maturers (catch-up).
Figure 1 shows that early maturers recovered (i.e., indicators decreased over time) in terms of their illicit drug abuse or dependence, whereas their on-time and late maturing peers caught up (i.e., indicators increased over time) in their alcohol abuse or dependence. Neither the recovery nor the catch-up hypothesis was fully supported for marijuana abuse and dependence.
Long-Term Persistence in Selected Groups
Despite the overall appearance of attenuation of the adolescent effects of early maturity in young adulthood, it is possible that adverse outcomes persisted for a subset of early maturers, such as those with the highest overall levels of adolescent problems. To test this hypothesis, we compared early maturers who had elevated levels of negative outcomes in adolescence (the upper 25% on a cumulative negative outcome scale, which corresponded to exhibiting five or more negative adolescent outcomes) with on-time maturers who had similar levels of adolescent negative outcomes to determine whether early maturation predicts a more persistent course of disturbance. These groups were compared on the total number of negative adult outcomes as well as on scales for total outcomes related to crime, substance use, socioeconomic status, sexual behavior, and mental health. The most troubled adolescent early maturers did not differ from similarly troubled on-time maturers in any adult outcomes (
Table 4).
Finally, it is plausible that early maturers with particular types of adolescent problems are more likely to have persistent problems. In fact, this pattern was already observed for adolescent conduct disorder predicting young adult depression. To further test for this pattern, interaction terms between significant adolescent outcomes and pubertal timing were entered into models predicting each domain of young adult functioning as well as specific young adult psychiatric disorders. There was little evidence that early maturation moderated the effect of adolescent indicators on young adult outcomes. Significant interactions occurred at the rate expected by chance and were as likely to indicate decreased as increased risk for early maturers compared with on-time and late maturers. (Full results are available on request from the first author.)
Discussion
Girls who developed early compared to those who did not were at greater risk for negative status outcomes in adolescence, including running away, substance-related dangerous behavior, and sexual behavior, as well as outcomes that are considered abnormal at any age, such as depression, criminal charges, and illicit drug abuse. The strongest effects were seen for substance abuse, followed by conduct problems and finally more modest effects on emotional functioning. This pattern is similar to that observed in previous studies that looked at a range of adolescent outcomes (
4,
11).
These negative effects were mostly time limited, however, with little evidence of continued problems into young adulthood. Attenuation of effects resulted from two concurrent processes: recovery by early maturers (e.g., early maturers decreased their illicit drug abuse or dependence over time) and catch-up by on-time and late maturers (e.g., on-time and late maturers increased drug abuse or dependence over time). Early puberty ceased to be a risk factor for young adulthood outcomes related to crime, substance use, education or employment, and most sexual behavior measures (number of lifetime sexual partners being an important exception). Except for girls with adolescent conduct disorder, there was little evidence for the existence of subgroups of early maturers—identified by either severity or type of adolescent problems—that continued to have trouble in young adulthood.
While previous studies suggest few long-term effects of early pubertal timing on behavioral outcomes, there is less agreement on outcomes that endanger the successful transition to independence, such as poor educational attainment and early motherhood (
5,
22,
23). Our results suggest that long-term effects on such outcomes are modest at best. Stattin and Magnusson (
15) found long-term effects only on postsecondary education levels and childbirth. In other areas of social support, personality, life values, and behavioral functioning (including delinquency, substance use, and smoking), few effects persisted. In our study, early developers displayed lower occupational status and more material hardship, but neither effect was statistically significant. Thus, even for outcomes related to transitioning to independence, the effects of early maturation are time limited, and most persisting effects are modest. One exception to this rule in the present study was depression.
In a previous study, we reported little effect of pubertal timing on depression in adolescence in this sample (
33). That analysis, however, included only the first four waves of the Great Smoky Mountains Study sample and two of three cohorts. The addition of 1,345 adolescent observations (all cohorts followed through to age 16) changed our conclusion. Early maturers who also displayed the highest levels of behavior problems in adolescence were at greatest risk for depression in young adulthood, a sequence of mental health problems previously found for both males and females (
34). Thus, the effect of pubertal timing on depression in young adulthood may be most easily detectable in those with a history of adolescent conduct disorder.
Early maturers were also much more likely than on-time and late maturers to report having had many sexual partners by young adulthood (a difference that was not significant in adolescence). A high number of lifetime sexual partners is linked with infection with human papillomavirus (
35), hepatitis C virus (
36), and HIV (
37) and thus is a significant public health concern.
Strengths and Limitations
The Great Smoky Mountains Study has several strengths besides its longitudinal prospective design. The key variable, early puberty, was assessed yearly and prospectively for most girls from middle childhood through adolescence; a population-based design minimized selection biases; and a wide range of functional domains in adolescence and young adulthood were assessed. The sample is not representative of the U.S. population, however; Native Americans are overrepresented and African Americans and Latinos are underrepresented. Also, the gold standard measure of pubertal development involves recurrent physical examinations by a medical professional. Such repeated intrusive assessment, however, would have been financially prohibitive and might have led to unacceptable sample attrition. Fortunately, there is adequate to good reliability between self- or parent-reported physical development and official medical records (
38). As evidenced by the findings in adolescence, our pubertal measure was sufficiently sensitive to detect significant effects.
Conclusions
Although the short-term ill effects of early puberty are well established, the question of whether early pubertal timing is sufficient to perturb normal functioning across subsequent developmental periods remains. The effects of most risk factors—even traumatic events—are generally time limited (
39). Early pubertal development in girls represents a possible exception to this general rule because of its effects on social networks, its occurrence at a sensitive period in terms of educational functioning, proposed links to early sexuality and pregnancy, and a gender-atypical elevation in conduct problems. Despite navigating a wide range of problems in adolescence, most early-maturing girls had levels of functioning similar to on-time or late-maturing girls by young adulthood. For a small group of early maturers, however, some troubles persisted nearly a decade after the start of the pubertal transition. This group could be identified by their conduct problems in adolescence and could possibly be provided with the assistance necessary to avert long-term distress. Clinicians and public health policy professionals would need only focus on a limited number of long-term outcomes for a limited number of early maturers.