Suicide is one of the leading causes of death worldwide (
1), but several barriers have slowed progress in understanding, predicting, and preventing suicidal behavior. First, attempts to predict suicide have relied almost exclusively on self-reporting of suicidal thoughts and intentions. This is problematic because self-reported data are subject to well-known reporting biases, and especially problematic in the case of suicide given that many people are motivated to deny suicidal thoughts in order to avoid hospitalization (
2). Second, there is a limited understanding of what factors actually predict suicidal behavior. To be sure, many risk factors have been identified, including the presence of psychiatric disorders, younger age, and a history of prior suicidal behavior (
3). However, these factors predict only a small amount of the variance in suicidal behavior and without a high degree of accuracy. Third, there is currently no accepted model for understanding how risk factors work together to cause suicidal behavior. This is not only a problem for researchers, but for clinicians, as there is currently no algorithm that clinicians can use to combine information about the multiple risk factors they might assess when trying to determine whether a patient is likely to make a suicide attempt in the near future. Thus, clinicians are left to use their intuition as a guide, which unfortunately is no better than chance at predicting suicidal behaviors (
4). Fourth, because suicide is a low base-rate behavior, very large samples are needed to test the complex models that have been proposed to predict suicide. Indeed, virtually all theories of suicide suggest that it is a multidetermined outcome in which many different factors work together to cause suicide attempts. However, the vast majority of prior research on this topic has tested simple bivariate models (
5).
What is needed are longitudinal data from large samples that can be used to develop and test new models of suicide risk. Such data are routinely collected in health information systems. However, this resource has been surprisingly underexplored by suicide researchers and represents a promising new direction for future scientific and clinical efforts. The growing adoption of electronic health records (EHRs) has created a powerful resource for epidemiologic and risk prediction studies (
6–
12). We previously showed that data commonly available in EHRs can accurately predict future domestic abuse diagnoses an average of 2 years in advance (
13). Using this information to support early detection of individuals at high risk for suicide and self-inflicted injury could help prevent significant morbidity and mortality and ensure that at-risk patients receive the professional care they need. Although some attempts to predict suicidal behavior using electronic health information have been reported, prior studies have had important limitations, including relatively small sample size (
14,
15), evaluation of a modest number of potential predictors (
14,
16), or limited data on prediction model performance (
16).
Here we report the development and validation of a risk prediction model using readily available EHR data to predict suicide attempts or death by suicide in a large health care system. As the data are already collected and readily available in the clinical setting, this study facilitates the goal of constructing a widely adoptable clinical decision support approach.
Method
The primary data source for this study was the Partners Healthcare Research Patient Data Registry (
17). The Partners Healthcare Research Patient Data Registry is a data warehouse of EHR data covering 4.6 million patients from two large academic medical centers in Boston (Massachusetts General Hospital and Brigham and Women’s Hospital), as well as community and specialty hospitals in the Boston area. To assemble the cohort for this study, the Partners Healthcare Research Patient Data Registry was queried for all inpatient and outpatient visits occurring between 1998 and 2012 (inclusive) at Massachusetts General Hospital and Brigham and Women’s Hospital. Development of the predictive model was conducted in the stages described below.
Case Definition and Validation
There were 1,728,549 patients who met the inclusion criteria of three or more visits, 30 days or more between the first and last visits, and the existence of records after age 10 and before age 90. For each patient, we obtained all the demographic, diagnostic, procedure, laboratory, and medication data recorded at each visit. We excluded 3,658 patients (0.21%) due to lack of historical data (as their first recorded encounter was for suicidal behavior) and 106 individuals for whom gender was not recorded. On average, each patient was followed for a period of 5.27 years, and the analysis included a total of 8,980,954 person-years.
Suicidal behavior was defined according to ICD-9 diagnostic codes and death certificates from the Commonwealth of Massachusetts. ICD-9 codes of E95* (injuries of intentional intent) are the most explicit diagnostic code for suicide attempts. To validate our case definition, we randomly selected 100 patients with an E95* code and reviewed all clinical notes within 1 week of the ICD-9 diagnosis. Three senior clinicians with expertise in the epidemiology and treatment of suicidal behavior (J.W.S., R.H.P., M.K.N.) manually reviewed narrative notes. Each note was designated as one of six categories using consensus agreement by all three clinicians (see Appendix 1 in the data supplement accompanying the online version of this article), and the positive predictive value of each code was calculated as the proportion of notes classified as either 1) self-harm, suicidal, or 2) self-harm, intentional, nonsuicidal.
Previous reports have indicated that ICD-9 codes matching E950* may have low sensitivity to detect suicidal behavior due to coding practices, reimbursement patterns, and the uncertainty of intent (
18). To maximize sensitivity of the case definition, we identified an additional set of 15 ICD-9 injury code categories and E98* (injury of questionable intent) as potential indicators of suicide attempts in the EHR (see Table S1 in the
online data supplement). The codes were selected based on prior literature, as well as a review of code descriptions.
For each ICD-9 category, the clinicians reviewed a small sample of patients using the chart review method above. If the prevalence of true cases was >20%, a larger sample of 50 randomly selected patients was subsequently reviewed. Code categories with a positive predictive value >0.70 were selected for our final case definition. These included E95* (positive predictive value: 0.82), 965.* (poisoning by analgesics, antipyretics, and antirheumatics; positive predictive value: 0.80), 967.* (poisoning by sedatives and hypnotics; positive predictive value; 0.84), 969.* (poisoning by psychotropic agents; positive predictive value: 0.80), and 881.* (open wound of elbow, forearm, and wrist; positive predictive value: 0.70). Detailed chart review results, including codes not included in the definition, are available in Table S1 in the online data supplement.
In total, over 2,700 notes for 520 individuals were reviewed to establish codes that best identified suicide attempt cases. These were supplemented by obtaining death certificates from the Commonwealth of Massachusetts, to capture completed suicides not recorded in the EHR. We also included a total of 852 death certificates between 1997 and 2010 with a “manner of death” of suicide (ICD-9: E95* or ICD-10 X60-X84, Y87.0) as cases.
Model Development
To explicitly account for differences by gender, we developed separate and independent models for men and women. We divided our cohort into two subcohorts of 718,793 men and 1,005,992 women. Each subcohort was randomly divided into training and testing (validation) sets of equal sizes. Based on the training sets, we developed naive Bayesian classifier models (
19) to estimate a patient’s risk for suicidal behavior. Naive Bayesian classifiers are a subclass of Bayesian networks with strong conditional independence of all input features, which greatly reduces model complexity and makes model development highly scalable for handling many independent variables. Naive Bayesian classifier models have been shown to be well-suited for clinical decision support and classification tasks (
13) and have the additional benefit of being easy to interpret. Models were developed using R version 3.1.1 with packages e1071, pROC, and ggplot2. Detailed description of model development is provided in Appendix 2 in the
data supplement.
The models included data on demographic characteristics, diagnostic codes, laboratory results (normal/low/high), and prescribed medications (true/false values). Data were collected up to but not including the first suicidal event for the case subjects and for all observed time periods for the control subjects. For each independent input variable in the training data set (e.g., diagnoses, medications, etc.), we assigned a partial risk score based on the ratio of its prevalence among case subjects compared with control subjects. The score was calculated on a logarithmic scale such that negative scores were “protective” (not associated with suicidal behavior), and positive scores were “adverse” (with higher prevalence among cases). In preparation for model validation, thresholds were selected to achieve benchmark specificities of 90% and 95% in the training sets.
Model Validation
We validated the models on the testing set of each gender subcohort, using a simulated prospective approach. For each patient, we calculated an overall risk score at each time point based on the data available for that patient until that time. For each item in the patient’s record, we assigned the appropriate partial risk score based on the model trained above. We then calculated the patient’s overall cumulative risk score by combining these partial risk scores for each subject. The patient’s score was interpreted using the thresholds selected during the training phase to achieve 90% and 95% specificities, respectively, and the sensitivity and timeliness of prediction at these levels of specificity were measured.
The Value of a Comprehensive Data-Driven Approach
To evaluate the usefulness of our comprehensive data-driven approach, we compared our results to the results obtained when looking at three widely accepted risk factors for suicide: 1) depression, 2) substance abuse, and 3) patients having any mental health condition (
20). We defined these risk factors using the Clinical Classification Software (
21) created and validated by the Healthcare Cost and Utilization Project. The Clinical Classification Software codes used were 657 for depression, 661 for substance abuse, and 650–663, 670 for all mental health conditions. Using the same training and validation sets described above, we tested the predictiveness of depression, substance abuse, depression and substance abuse, and any mental health condition (including depression and substance abuse) for suicidal behavior.
Results
Model Composition
Of the total 1,728,549 patients, we identified 20,246 (1.2%) cases with suicidal behavior. All other patients were labeled as controls. As previously described, we excluded 3,764 subjects from our analysis due to missing data, resulting in a final set of 16,588 case subjects and 1,708,197 control subjects. Of the 852 death certificates with suicide as a cause of death, only 49 did not have one of the ICD-9 codes that comprise the case definition, indicating high sensitivity of our EHR case definition.
The demographic characteristics of all patients recorded within the Partners Healthcare Research Patient Data Registry data warehouse (including the excluded cases) are presented in
Table 1. The relative score associated with each demographic factor by gender is summarized in
Table 2. Overall, suicidal behavior was more common among men than women (odds ratio=1.75, 95% confidence interval [CI]=1.68–1.82). For both men and women, “separated” marital status was associated with more than a fourfold risk of suicidal behavior compared with married patients (p<0.001). Higher risk of suicidal behavior was observed in African American (odds ratio=1.31, 95% CI=1.22–1.41) and Hispanic (odds ratio=1.68, 95% CI=1.58–1.79) patients compared with Caucasian patients. With regard to age, higher prevalence of suicidal behavior was found in women under the age of 25 (odds ratio=1.5, 95% CI=1.37–1.64 compared with other age groups) and in men aged 25–45 (odds ratio=1.83, 95% CI=1.73–1.93 compared with other age groups).
Details regarding the risk scores associated with individual codes are presented in Table S2 in the
online data supplement. (It is noteworthy that while Table S2 in the
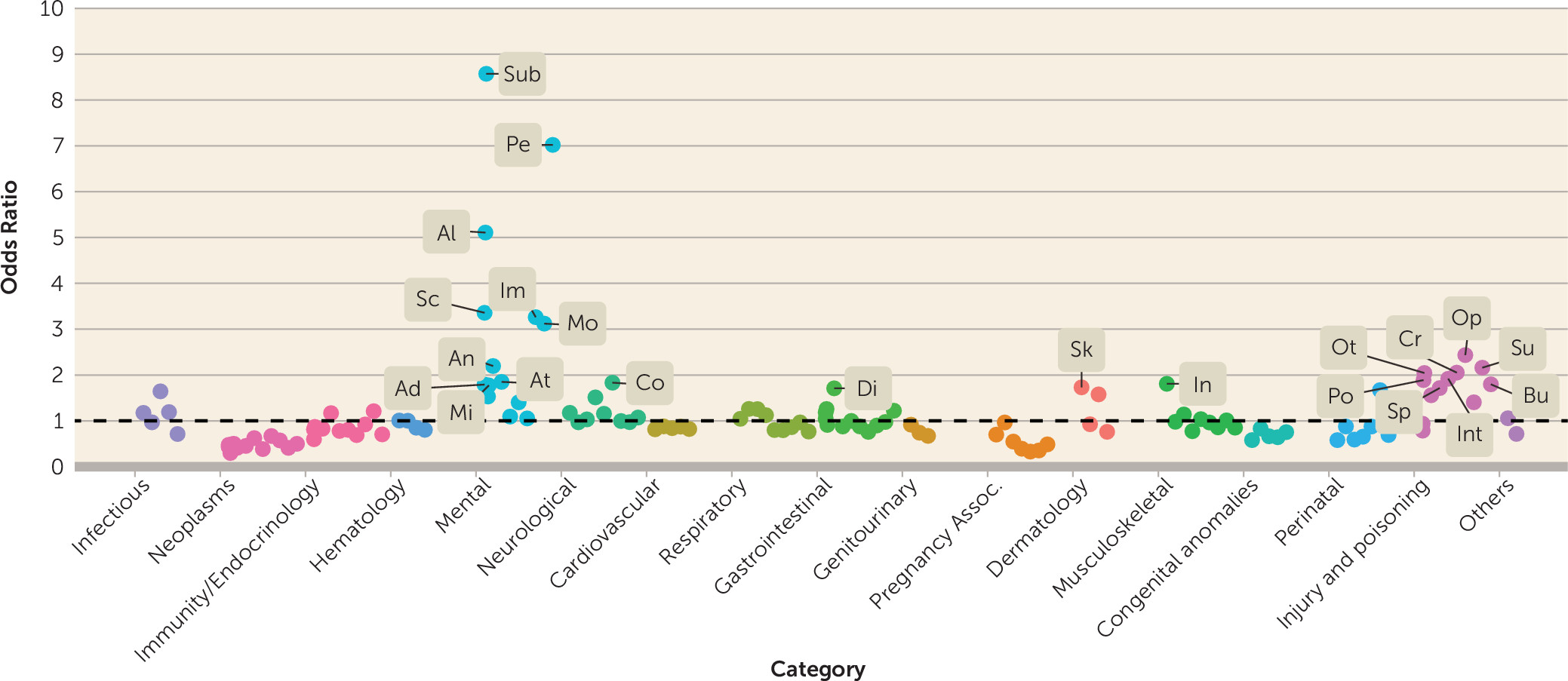
data supplement highlights only the top 100 codes associated with suicidal behavior, the naive Bayesian classifier model actually captures risks associated with all available codes.) Opioid abuse was 16 times more common among case subjects than control subjects (95% CI=14.9–22.8), and personality and bipolar disorders were 7–10 times more common among case subjects (p<0.001). Of note, however, a variety of other clinical features beyond mental health diagnoses appeared among the top 100 predictors, including infections such as hepatitis C carrier (odds ratio=6.1, 95% CI=4.5–8.1), alveolitis of the jaw (odds ratio=5.8, 95% CI=3.7–9.4), osteomyelitis (odds ratio=4.85, 95% CI=2.9–8.0), cellulitis (odds ratio=4.6, 95% CI=3.9–5.4), and numerous codes related to wounds and injuries including contusion of the back (odds ratio=4.7, 95% CI=3.1–7.2) (see Table S2 in the
data supplement for additional details). A summary view of the effect sizes (odds ratios) of diagnostic codes grouped into 135 categories is presented in
Figure 1, as defined by the Clinical Classification Software codes mentioned previously. As expected, suicidal behavior is strongly associated with substance abuse and psychiatric conditions in both men and women (see Table S2A in the
data supplement). The lists of top medications and laboratory tests (Table S2B and C in the
data supplement) also highlight the elevated suicide risk associated with drug abuse and mental illness. The top laboratory results associated with suicidal behavior were related to standard toxicology screenings, and the top medications associated with suicidal behavior were mostly psychiatric drugs.
Model Performance
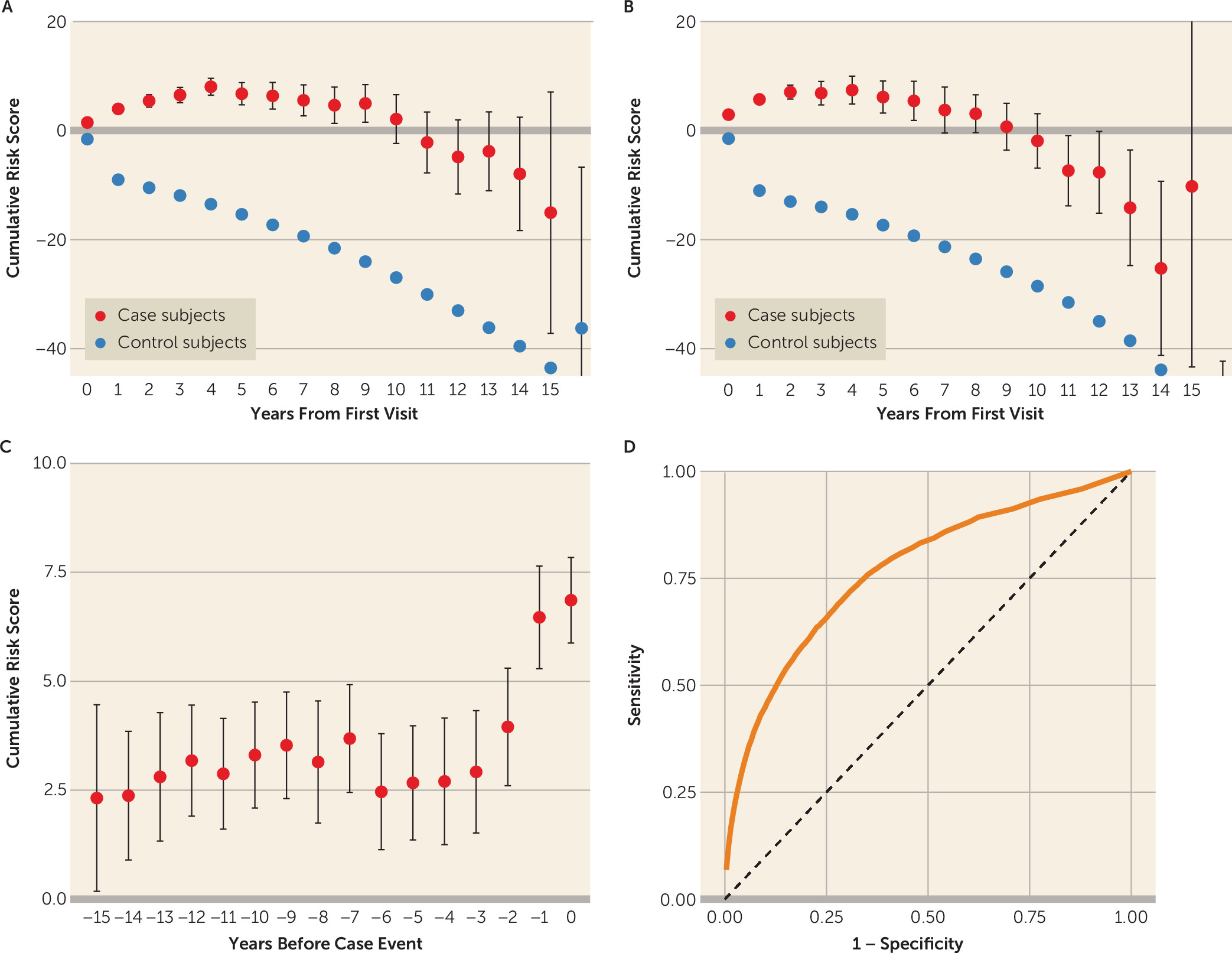
Relying solely on coded information commonly available in the EHR, the model successfully predicted suicidal behavior with an overall area under the receiver operating characteristic curve of 0.77 (
Figure 2). The model performed similarly in female and male cohorts (area under the curve=0.77 [95% CI=0.77–0.78] compared with 0.76 [95% CI=0.75–0.77], respectively). Detailed results of the naive Bayesian classifier model by gender are summarized in
Table 3. With 90% specificity, the model detected 44% and 46% of the suicidal cases among men and women, respectively. Consistent with the low base rate of suicidal behavior in the full cohort, the positive predictive value was 5% and 3% compared with 1.55% and 0.9% baseline prevalence for men and women, respectively. Running the model by gender for specific age groups yielded even better prediction for narrower subpopulations, such as women ages 45–65 where, for 90% specificity, the model achieved 54% sensitivity (see Table S3 in the
data supplement).
One of the model’s key strengths is its ability to incorporate the full phenotypic breadth for the EHR in making a prediction—beyond what an individual clinician might typically use in a given encounter. To examine the advantages of this approach, we compared the model performance to that of simple models based only on commonly used risk factors. Allowing for a 10% false-positive rate, the full model achieved 45% sensitivity, while models that only used various combinations of widely accepted risk factors performed substantially worse: 29% for depression (area under the curve=0.62 [0.62–0.63]), 25% for substance abuse (area under the curve=0.58 [0.58–0.59]), 34% for depression and substance abuse (area under the curve=0.65 [0.64–0.65]), and 19% for any mental health condition (area under the curve=0.64 [0.63–0.64]). Thus, the relative increase in sensitivity was 32% to 137% compared with these simpler models.
We also examined the average time that models were able to predict suicidal behavior in advance of an individual receiving a case-defining diagnosis. Setting specificity at 90%, the model predicted suicidal behavior an average of 4.0 years before the case-defining code was recorded in the EHR for the 45% of the cases identified by the model at this specificity level. Increasing the model specificity to 95% (i.e., only 5% false positives), our classifier predicted suicidal events an average of 3.5 years prior to the diagnosis for the 33% of the cases identified by the model at this specificity level.
The average cumulative risk scores over time for case subjects compared with control subjects are shown in
Figure 2A for women and in
Figure 2B for men. As time progresses, there is growing separation between the cumulative score for case subjects compared with control subjects, with a maximal difference after 15 years. A different view of the case subjects is shown in
Figure 2C, with risk scores by year leading up to the date of their suicidal event. As shown, there is a noticeable increase in the scores in the 3–4 years in advance of the index event.
Discussion
Using data commonly available in EHRs, our models were able to identify nearly half of all suicides and suicidal behaviors with 90% specificity, an average of 3–4 years in advance. The increasingly widespread adoption of EHRs provides unprecedented opportunities for practical application of precision medicine, including the possibility of risk prediction for major health outcomes. Suicide attempts and suicide deaths are major sources of morbidity and mortality, and prior research has demonstrated that clinicians are generally unable to predict these outcomes (
4,
22,
23).
Our empirical, data-driven modeling approach has a number of key strengths. First, we are able to examine both established and previously unsuspected risk factors by leveraging the full phenotypic breadth offered by the EHR. The most highly weighted variables found by the model were psychological conditions and substance abuse, corresponding to findings from prior epidemiologic studies (
1) and supporting the validity of our model. However, rather than limiting the risk profile to known or hypothesized risk variables, the naive Bayesian classifier model assigns risk weights to all of the coded variables in the health record: diagnoses relating to fractures, wounds, infections, and injuries, as well as certain chronic conditions such as hepatitis, were also associated with elevated suicide risk. Second, this modeling approach assigns separate risk scores not just to general categories of disease (e.g., prior psychiatric disease) but rather to each individual diagnostic, laboratory, and prescription code, allowing for greater insights into which specific codes are associated with higher risk. Third, the longitudinal nature of the EHR allows us to estimate the cumulative effect of risk factors over time and to identify risk profiles well in advance of the index event. Fourth, the model can be tailored to the specific setting and coding environment in which it is implemented: variables’ weights can be calibrated using retrospective data from the target site and the selected thresholds modified according to the costs associated with false positive and false negative predictions.
The idea of mining EHR data for suicide risk prediction has been explored in several previous studies. Baca-Garcia and colleagues (
14) used several data-mining strategies to reanalyze data from a study of clinician decision-making in the emergency department regarding 509 individuals who attempted suicide. Predictions were based on 139 features that were reduced to five in the best-performing model. The study was based on a smaller sample and number of features compared with the model described in our study. Ilgen and colleagues (
16) applied recursive partitioning to a sample of Veteran’s Affairs patients treated for depression in order to predict risk of suicide ascertained from the National Death Index. They identified 1,892 deaths by suicide using ICD-9 codes and specified a set of eight candidate predictors derived from treatment records, but model performance metrics were not reported. Using a different approach, Poulin and colleagues (
15) derived a machine-learning algorithm based on clinical notes in the Veteran’s Affairs medical record to distinguish three groups (N=70 in each group): those who received mental health treatment and did or did not die by suicide and a control group of those who neither used mental health services nor died by suicide. They achieved an overall classification accuracy of up to 67% (compared with up to 94% in our study). Tran and colleagues (
23) applied a penalized regression modeling approach to coded EHR data for 7,399 patients who underwent suicide risk assessment by clinicians and were followed for 180 days. Compared with clinician predictions based on an 18-point suicide assessment checklist, the EHR-based model was more successful in stratifying risk at 30–180 days. Compared with our results, this study focused only on subjects who underwent screening for suicide and predicted risk over a relatively short time frame. Finally, in a study of U.S. Army personnel, Kessler and colleagues (
24) applied machine-learning approaches to EHR and administrative data records to predict suicides in the year following a psychiatric hospitalization. In their best-fitting model, 53% of the suicides occurred after the 5% of hospitalizations with the highest predicted suicide risk, but their use of the rich administrative and personal data available in the comprehensive military database limits generalization to standard health care systems. Our model has advantages over these prior studies. First, it uses data readily and widely available in today’s EHR systems. Second, it includes a broader range of variables and a larger and more diverse sample than in prior studies. Third, the model incorporates time-varying data, allowing us to determine the timeliness of predictions.
Our results should be interpreted in the context of several limitations. We used 15 years of data from an urban-regional data set including hospital admissions, observation stays, and encounters in emergency and outpatient settings. This data set excluded any patient visits outside this geographical area, time period, or network of hospitals, thus potentially losing some patients to follow up. As a result, certain codes that may have assisted in identifying high-risk patients may not be recorded in the data set. Furthermore, some of the excluded visits could have been for suicidal behavior that was not recorded in this data set, meaning that these individuals may have been incorrectly classified as control subjects or correctly classified as case subjects but given incorrect onset times. That said, our goal was to determine whether data commonly available in today’s real-world EHRs can be used to effectively predict suicidal behavior in a sensitive, specific, and timely manner. Our case definition includes codes that we validated to be highly specific for suicidal behavior. Nevertheless, variability in coding practices could limit the generalizability of our model in some settings. For example, some studies have supported the sensitivity, specificity, and predictive value of E-codes and other suicide-related codes (
25,
26), while others have not (
27–
29).
Alternative approaches (e.g., neural networks, support vector machines, and other machine-learning approaches) might yield comparable (or possibly greater) predictive accuracy but are typically “black box” models that are difficult to interpret. Rather than using complex model selection or data reduction procedures to identify a subset of predictive variables, we demonstrate that the straightforward approach of using all the clinical data available for a patient does very well. In addition, to maximize the generalizability of our tool to other health care systems, we deliberately use codified data that are readily available in EHRs rather than relying on complex text-mining approaches (e.g., natural language processing) that can be more difficult to implement and more sensitive to local documentation practices.
Several aspects of our risk-prediction approach could be enhanced in future research. For example, currently the model yields low to moderate positive predictive value (5%−7% at 95% specificity), although this is to be expected in a condition with a very low baseline probability (1.2%) and represents a 4.5- to 6.5-fold enrichment of suicide risk prediction compared with the base rate. Applying our approach to patient subsamples with high prevalence of suicide risk (e.g., patients in psychiatric care) could enrich the base rate and improve the model’s positive predictive value. Additionally, our model currently captures the risk associated with each feature (e.g., diagnoses) separately. More complex models incorporating combinations or interactions of features may improve diagnostic accuracy. With appropriate integration into the clinical workflow, this model can assist already overloaded clinicians to identify high-risk patients who require further in-depth screening. Although a statistical model is never a substitute for clinical evaluation, an early warning system based on our approach may provide a mechanism for identifying patients who are at elevated statistical risk of future suicidal behavior and therefore require screening. This is especially important, since screening rates in clinical settings remain far below desired levels (
30).
After further refinement, we envision our models being used as a dashboard element in the EHR at the point of care. In ongoing work, we are designing a user-friendly visualization suitable for incorporation into the EHR interface. For each patient, the system could present the clinician with a high-level summary of short-term, medium-term, and long-term suicide risks, alongside a visualization of the patient's longitudinal history and a list of the most prominent risk factors for that given individual. It will also provide carefully worded messages for clinicians, explaining what the risk alert means and what information it is based on. These messages will be crafted in consultation with clinicians in order to avoid misunderstandings and ensure seamless integration into the clinical workflow. It is important to reiterate that our approach is designed as a screening tool for decision support rather than a specific quantitative prediction of suicide risk. Given the imperfect predictive value of any automated model, it would be inappropriate (and medicolegally imprudent) to base clinical decisions (such as hospitalization) solely on model readouts. Rather, we envision an alert system by which patients exceeding thresholds of predicted risk could be flagged as at relatively higher risk to encourage clinicians to conduct more targeted assessments of suicide risk.
In conclusion, these findings suggest that the vast quantities of longitudinal data accumulating in electronic health information systems present a largely untapped opportunity for improving medical screening and diagnosis. Beyond the direct implications for prediction of suicide risk, this general approach has far-reaching implications for the automated screening of a wide range of clinical conditions for which longitudinal historical information may be beneficial for estimating clinical risk.