Human immunodeficiency virus (HIV) testing is a cornerstone in efforts to detect, treat, and prevent HIV infection. With the advent of more effective therapies in recent years, early diagnosis is important in optimizing a treatment plan and forestalling the progression of AIDS and death
(1). In addition, earlier awareness of one’s seropositivity may lead to decreased future transmission of the virus, given the long asymptomatic period during which an HIV-infected individual could unknowingly be spreading the virus to others. Even for those whose test results are negative, pre- and posttest counseling sessions provide valuable opportunities for HIV education and risk-reduction counseling. Of course, HIV testing alone is not enough; individuals must also return for their test results. Indeed, of the nearly 2.3 million publicly funded HIV tests that were performed in the United States in 1998, 48% of those tested had no posttest counseling, and some of the highest failure rates were among those most at risk for infection
(2).
Compared with the general population, persons who are homeless and chronically mentally ill are at higher risk for HIV infection, reflecting their higher rates of drug use and sexual risk behaviors
(3–
6). Moreover, numerous studies have demonstrated HIV seroprevalence rates of ≥1% in homeless samples across the country
(3,
7–9). Thus, according to Centers for Disease Control and Prevention (CDC) guidelines
(1), homeless persons represent a population for whom HIV testing should be routinely recommended. Despite the importance of HIV testing, however, few studies
(9–
13) have examined factors associated with testing and return for test results in this vulnerable, high-risk population. The current literature in this area is somewhat limited in at least two respects. First, prior research has focused on identifying correlates of past HIV testing behaviors by using cross-sectional data, potentially limiting the interpretation of some associations. Second, previous studies have focused on groups of homeless persons living in specific locales and, therefore, are of limited generalizability.
In the present study, we used prospective data from a large, multisite homeless outreach demonstration project to determine the rates and predictors of HIV testing and receipt of test results among clients in the 3-month period after program entry. By identifying predisposing, enabling, and need factors associated with HIV testing and return for results, the findings of this study are expected to enhance the development and targeting of strategies to increase awareness of HIV serostatus among seriously mentally ill homeless persons.
Results
Study Participants
In total, 7,229 individuals were enrolled in the ACCESS program and completed a baseline interview. Nonmutually exclusive psychiatric diagnoses, based on a clinician’s assessment at the time of referral, included major depression (48.7%), schizophrenia (36.2%), other psychoses (31.4%), personality disorder (22.0%), bipolar disorder (20.3%), and anxiety disorder (18.0%). Rates of substance abuse were also high (42.8% with alcohol abuse and 38.4% with drug abuse).
For the purposes of this study, we excluded 237 individuals (3.3%) who reported being HIV-positive at baseline. Of the remaining 6,992 persons, 1,035 (14.8%) were excluded because they did not have a 3-month follow-up interview; an additional 67 (1.0%), although interviewed, were excluded because of missing outcome data. Thus, the final number of participants was 5,890. Compared with clients who were lost to follow-up, those who completed a follow-up interview were significantly more likely to be female (χ
2=8.79, df=1, p=0.003) and nonwhite (χ
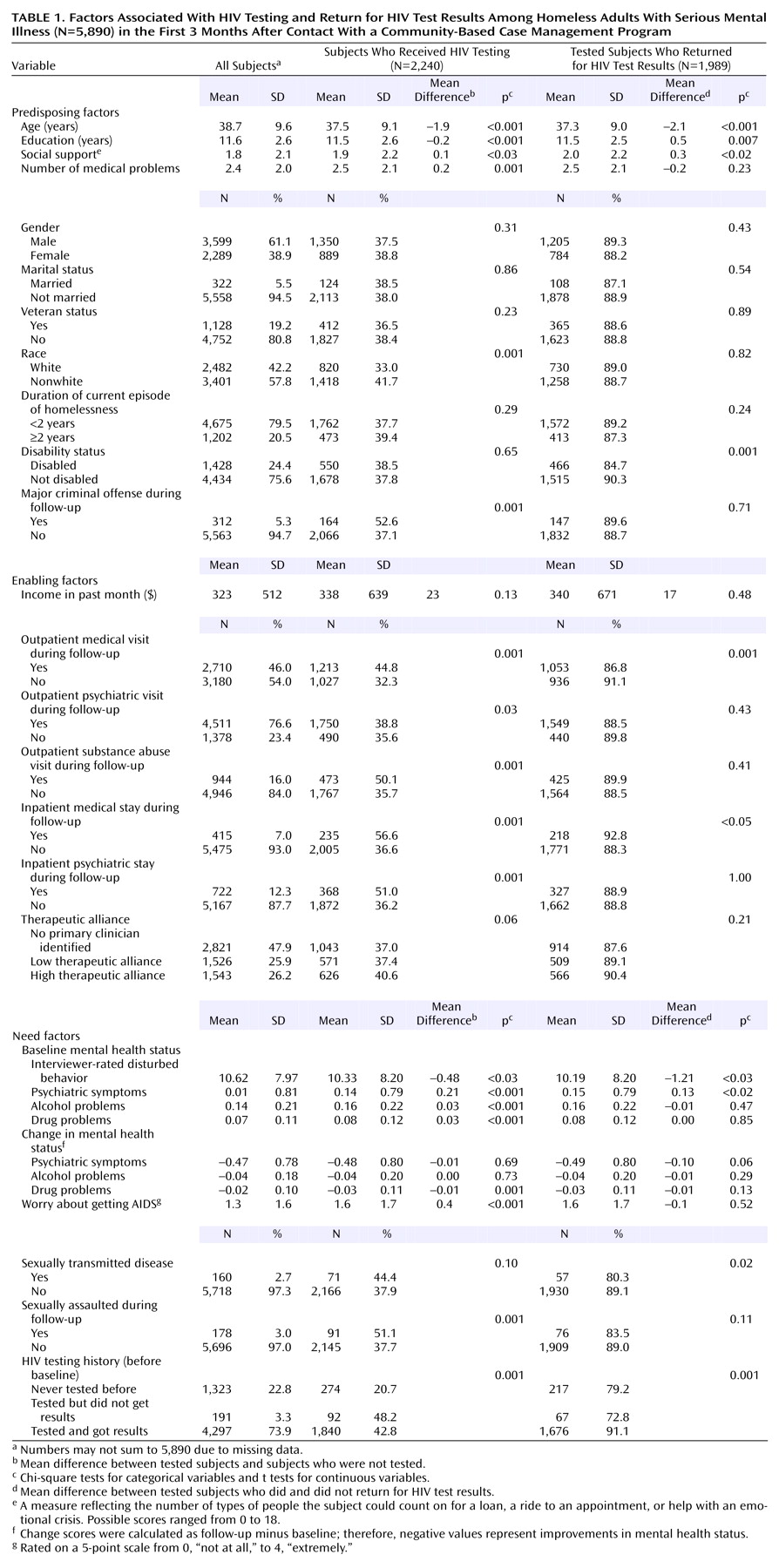
2=12.50, df=1, p=0.001) and to have greater social support (t=4.69, df=6983, p<0.001), medical problems (t=2.46, df=6990, p<0.02), and psychiatric symptoms (t=2.47, df=6765, p<0.02) (data not shown). The characteristics of the study participants are summarized in
Table 1.
Rates of HIV Testing and Return for Test Results During Follow-Up
Of the 5,890 clients included in this study, 2,240, or 38.0%, reported being tested for HIV during the 3-month follow-up period. Among those tested, 88.8% (1,989/2,240) reported receiving their test results. Across sites, the rate of testing ranged from 26.6% to 48.1% and the rate of receipt of test results ranged from 69.4% to 99.3%.
Predictors of HIV Testing
Bivariate associations between all potential predictors and HIV testing are presented in
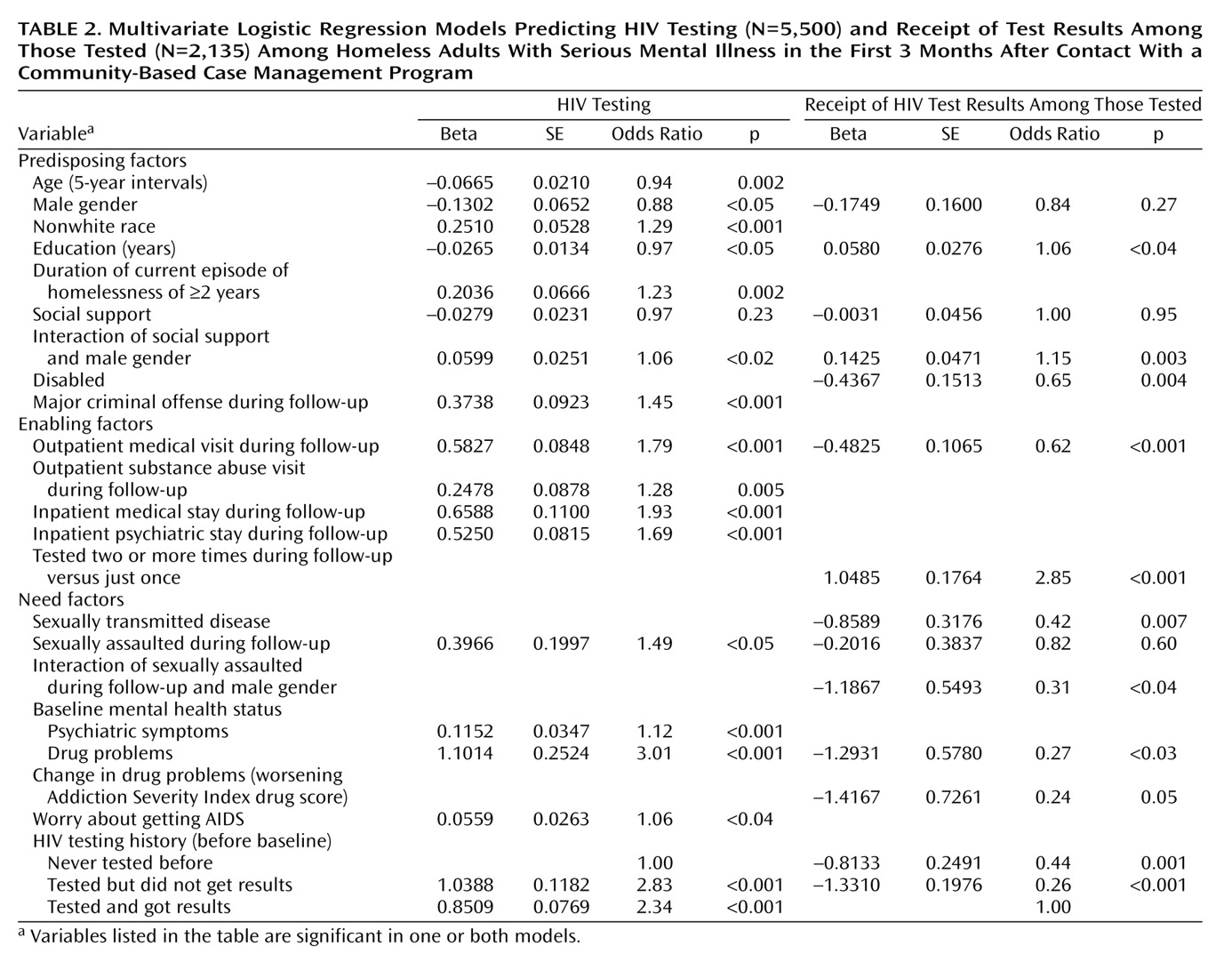
Table 1, and the final logistic regression model is presented in
Table 2. As
Table 2 shows, the likelihood of being tested for HIV after program entry decreased as both age and educational level increased.
Positive predictors of testing included the following HIV risk-related variables: nonwhite race, longer-term homelessness, being sexually assaulted during follow-up, more severe psychiatric symptoms and drug problems, and self-perceived risk or level of worry about getting AIDS. Among the strongest predictors of HIV testing was clients’ prior testing history; that is, clients who had been tested before, regardless of whether they ever got the results, were significantly more likely to be tested during follow-up than those who had never been tested before. Health services utilization and having been arrested and charged with a major crime during follow-up were also strongly associated with receipt of HIV testing.
Finally, we found a significant interaction between social support and gender. At lower levels of social support, men were less likely than women to be tested for HIV. As the level of social support increased, however, so did the likelihood of being tested, but only among men; the same was not true for women.
Predictors of Receipt of HIV Test Results
Bivariate and multivariate associations between predictor variables and the likelihood of getting one’s HIV test results are presented in
Table 1 and
Table 2, respectively. As
Table 2 shows, receipt of results among those tested was positively associated with level of education and negatively associated with being disabled, outpatient medical service utilization, having a sexually transmitted disease other than HIV, and both drug problems at baseline and worsening drug problems over the course of follow-up.
Frequency of HIV testing during follow-up and prior testing history were also predictive of getting the results. Twenty-one percent (473/2,240) of those tested for HIV during follow-up were tested more than one time, and the odds of getting their results were nearly threefold greater in this group, compared with clients who were tested just once. As for HIV testing history, both first-time test recipients and those who had a history of being tested but not getting the results were significantly less likely to get their HIV results during follow-up than were clients who had a track record of returning for test results.
Moreover, we found two significant gender interaction terms. First, like the odds for HIV testing, the odds of returning for test results were increased by social support among men but not among women. Second, having been sexually assaulted decreased the likelihood that men would return for their HIV test results; the same was not true for women, however.
Discussion
Using prospective data from the ACCESS demonstration, we found that, despite CDC guidelines that high-risk, high-prevalence populations be routinely recommended HIV testing
(1), less than 40% of ACCESS clients reported being tested for HIV in the 3 months after program entry. Of those tested, however, 88.8% reported receiving their test results. Using the framework of Gelberg et al.
(17), we identified predictors of HIV testing and receipt of results from predisposing, enabling, and need domains in an effort to identify potential target populations for interventions aimed at increasing HIV serostatus awareness.
Previous cross-sectional studies have shown that persons who are at greatest risk for HIV infection due to sociodemographic, sexual, and clinical risk factors are usually the most likely to have been tested
(27,
28). Consistent with these findings, we found that significant, independent predictors of HIV testing during follow-up included younger age, less education, nonwhite race, longer-term homelessness, being sexually assaulted during follow-up, higher levels of psychiatric symptoms and drug problems, and greater worry about getting AIDS.
None of these HIV risk-related variables, however, also predicted following through with getting the results among those tested. On the contrary, drug problems (both higher levels at baseline and worsening problems over the follow-up period), as well as being disabled, appeared to be impediments to returning for results. Moreover, whereas being a victim of sexual assault increased the odds of getting tested for HIV, perhaps due to greater contact with emergency health services, sexual victimization was associated with decreased odds of returning for results, particularly among men. Having a sexually transmitted disease other than HIV also was associated with failure to get HIV test results. These latter findings are consistent with studies suggesting that denial and fear may serve as barriers to learning one’s HIV status
(28,
29). Taken together, they point to the need for targeted interventions on the part of HIV counselors and mental health providers to increase rates of return for test results among at-risk individuals who, for whatever reason, may be unable or unwilling to get their results. Efforts to develop better coping skills, for example, have been shown to reduce HIV risk behaviors in impoverished populations
(30) and may be effective in increasing rates of HIV testing and return for results
(10,
11).
Consistent with previous research demonstrating an association between access to care and receipt of HIV testing
(31), we found that clients who were linked with outpatient medical and substance abuse services were significantly more likely to be tested than were those who did not receive such services. In addition, we found that inpatient stays and having been arrested and charged with a major crime increased the likelihood of HIV testing. While these latter findings are consistent with studies documenting relatively high rates of “voluntary” testing in hospitals
(32) and prisons
(33), it is important to note that higher acceptance rates are more likely when informed consent is vague and HIV testing is presented as “routine” rather than as optional
(28). Believing that HIV testing is mandatory and bundled with other services, institutionalized persons may be more likely than their noninstitutionalized counterparts to accept testing.
An important predictor of HIV testing and receipt of results during follow-up was clients’ prior experience with HIV testing. Knowing whether clients have been tested previously and, if so, whether they received those earlier results will help clinicians to identify individuals who may benefit from additional and more careful follow-up. In addition, repeated HIV testing during follow-up increased the likelihood of actually getting the results and thus may prove to be a useful strategy in helping to increase HIV serostatus awareness among mentally ill homeless persons, who often live chaotic lives and for whom returning for test results may be a challenge.
This study had some limitations. First, although the baseline participation rate was high, follow-up interviews were missing for 15% of the baseline participants. Because those who were lost to follow-up may have been the least likely to receive needed services, we may have overestimated the rates of HIV testing and receipt of results in this group of clients.
Second, the ACCESS program was not focused on HIV/AIDS and related outcomes; therefore, detailed information was not available on high-risk sexual or substance abuse behaviors. Nevertheless, we were able to examine the effect of a broad array of individual-level predisposing, enabling, and need factors on HIV testing and receipt of results.
Third, the study relied on self-reported data. We were not able to validate responses using external sources, such as medical records. However, others have demonstrated a reasonably high level of validity for self-reported data about HIV testing and results
(34).
Finally, given the complex needs of clients and the competing demands on clinicians, it may be argued that the 3-month follow-up period was too short and that if one were to look over a longer period of time, a greater percentage with HIV testing would be found. As a secondary analysis, we looked at available 12-month follow-up data for the study participants and found that an additional 1,123 clients reported being tested for HIV sometime between the two follow-up interviews, resulting in a total percentage tested of 57.1% (3,363/5,890) in the year after program entry. Although the appropriate timing and frequency of testing have not been firmly established
(1), these data highlight that a substantial proportion of clients did not receive HIV testing even a year after initial contact with the program and that, among those who were tested, fully two-thirds were tested in the first 3 months after program entry.
In summary, we found a high rate of follow-through in returning for HIV test results among those tested, which likely reflects the fact that the study participants were enrolled in an intensive case management program. In this sense, our findings may overestimate the experience of vulnerable homeless persons contacted through other programs or points of service delivery. Despite the ACCESS program’s emphasis on case management and coordination of care, however, and despite public health guidelines, the majority of clients were in fact not tested for HIV in the 3-month period after program entry, and a substantial proportion were not tested even after 12 months. These findings highlight the need for greater efforts to increase testing and awareness of HIV serostatus among high-risk homeless persons in order to better care for HIV-positive individuals and potentially reduce future transmission of the virus. Activities aimed at educating both clients and mental health providers about HIV may be effective in increasing rates of HIV testing and counseling among homeless persons with serious mental illness.