Empirical studies of the incidence, patterns, and clinical characteristics of homicide-suicide in older persons have not been published (
1). There are several explanations for this, including the low frequency of homicide-suicides across all age groups and the lack of a standardized operational definition and surveillance system. Homicide-suicides involve a perpetrator, usually a male, who commits one or more homicides and shortly thereafter commits a violent suicide (
2,
3). Homicide-suicide normally occurs within a family context and may involve children, but most cases are characterized by a spousal or love relationship between the perpetrator and victim. Firearms are the lethal weapon in most instances. Although the time between the homicide and suicide is usually minutes or hours, in the few studies specifying intervals, the time ranged from 24 hours to 3 months.
The reported annual incidence has been constant, ranging from 0.2 to 0.3 per 100,000 in the United States and other countries, whereas rates of suicide and homicide separately vary substantially (
4–
11). Homicide-suicides, also reported in terms of percentage of total homicides, vary regionally in the United States, from 1% to 20%, but average about 5%. The percentage varies widely across other countries, ranging from 3% to 60%, and is related to homicide rates, i.e., the higher the homicide rate, the lower the percentage of homicide-suicide (
2,
5,
12).
Homicide-suicides have been classified as spousal/consortial, familial, and extrafamilial types, with different subclassifications defined by relationship and age of individuals involved and attributions of motivation from postmortem interviews. Precise operational criteria are lacking, although several investigators have proposed research strategies to formulate a standardized definition and taxonomic system (
2,
3,
11). Marzuk et al. (
3) proposed two subtypes of the most common form, spousal/consortial homicide-suicide: 1) the amorous-jealous subtype, referring to circumstances in which the perpetrator is a young man who kills a lover or wife, reportedly motivated by rage, jealousy, and paranoia at a time of pending or real separation; and 2) the declining health subtype, referring to situations in which the perpetrator is an older man caring for an impaired wife, and both may be in failing health. However, as the authors stressed, empirical evaluation of the typologies is needed.
There are no published studies reporting base rates or documentation of the characteristics of older homicide-suicide cases (
1,
9). Most studies have also not differentiated spousal/consortial homicide-suicides from other classifications except to report the proportions within categories (
11). The anecdotal literature has described homicide-suicides in older couples, interpreting them as dual suicide pacts, dyadic deaths, or homicide-suicide with altruistic motives attributed to the perpetrator (
9). This is the first empirical report of the incidence of homicide-suicides by age as well as the clinical characteristics of homicide victims and suicide perpetrators of spousal/consortial deaths.
METHOD
Case Ascertainment
We contacted four medical examiner offices covering seven entire Florida counties where the medical examiner agreed to help identify homicide-suicide cases and make death lists from 1988 to 1994 and case files available to us. These districts were chosen to identify the number of new homicide-suicide events each year over the 8-year period in two regions of Florida—west central and southeastern Florida—both comparable in the size of the total population and high concentrations of older persons. Three medical examiner districts were in west central Florida: District 6, Pasco and Pinellas counties; District 12, DeSoto, Manatee, and Sarasota counties; and District 13, Hillsborough County. District 11 covered Dade County in southeastern Florida.
All four medical examiner offices maintained separate yearly death listings for homicides, suicides, accidents, motor vehicles, and natural causes. Suicide and homicide lists were analyzed to identify homicide-suicide events each year from 1988 to 1994 by matching dates, code numbers, names, ages, sex, and available investigative details. District 6 had separate computerized listings of homicides and suicides with descriptions of the events, but also cross-referenced when a homicide-suicide occurred, including circumstances when the homicide-suicide was not successful, i.e., either the perpetrator or victim did not die. A total of nine homicide-suicide attempts in older couples were recorded in District 6. In District 11 hard copy records were indexed yearly in books in which each page described a case, often cross-referencing a homicide-suicide. Information on lists from Districts 12 and 13 was minimal, consisting of only medical examiner codes, date, age, sex, and race.
Complete medical examiner files, including investigative and autopsy reports, toxicology results, and other information, were photocopied for all matches. The files often included newspaper reports, notes by decedents, photographs, family contacts, FBI reports, and fingerprints. Complete death certificates were in medical examiner files for 74% of the southeastern Florida cases and 59% of the west central Florida cases.
A search was also conducted to identify homicide-suicide stories from 1988 to 1994 by using CD-ROMs available for the two major newspapers in the west central Florida region, in order to ascertain additional clusters. Seventeen new stories of homicide-suicide were discovered, and medical examiner records were obtained for all of them. A CD-ROM was not available for the major newspaper in District 11.
Criteria for inclusion as a homicide-suicide case in this study were as follows.
1. Medical examiner reports concluded that a person had committed a homicide (or homicides) and subsequently committed suicide. When death certificates were available, they had to concur that the linked deaths of the victims and perpetrators were homicide and suicide, respectively.
2. It had to be determined that the perpetrator had committed suicide within 24 hours of the homicide. Proximity of deaths was established from information in medical examiner reports.
3. The homicide-suicide event had to be classified as one of the following nonoverlapping categories: spousal/consortial couples; filicide-suicide in which the homicide victim (or victims) was a child 0–16 years old; familial homicide-suicide in which the homicide victim was a family member (but not a spouse or consort) or a child older than 16 years; nonfamilial homicide-suicide in which the homicide victim (or victims) was not a family member; and mass murder in which five or more persons were hurt and at least three persons were killed. Dyadic deaths of older siblings were classified as familial homicide-suicide. A case of a husband or lover who killed a spouse or girlfriend and another family member 16 years or older before committing suicide was classified as a familial homicide-suicide. If the third person was a nonfamily member, the act was classified as nonfamilial homicide-suicide.
Exclusion criteria were as follows: 1) a homicide-suicide was attempted, but one or both parties did not die; and 2) a suicide note signed by both victim and perpetrator specified that the circumstances were a suicide pact and neither of the decedents had dementia.
Annual Incidence
We ascertained the number of new homicide-suicide cases each year, i.e., incidence, and calculated annual incidence rates for 7 years from 1988 to 1994, age-adjusted by year for total homicide-suicide events per 100,000 total population, per 100,000 persons 55 years and older, and per 100,000 persons 54 years and younger. A homicide-suicide case was assigned to an age group by age of the perpetrator. Annual rates were calculated through use of population estimates by age and by county from 1988 to 1994 from the Bureau of Economic and Business Research at the University of Florida (
13,
14). The bureau used a cohort-component methodology in which births, deaths, and migration were estimated separately for each age-sex-race cohort by county, to derive intercensual estimates from 1983 to 1993 as well as projections from 1994 to 2010.
Features and Characteristics
A total of 160 variables in seven areas were coded from information in the medical examiner files by using a format adapted from the U.S. Air Force autopsy protocol. There were 12 incident identification variables, e.g., file number, date of death, type of homicide-suicide; 15 sociodemographic variables; 24 variables describing physical circumstances, e.g., location of bodies, presence of suicide notes, drugs at the scene; 35 antecedent conditions, e.g., illness, separation, adverse life circumstances; 24 drug categories from toxicology studies; and 50 autopsy findings, including medical examiner ICD codes. Medical examiner reports and death certificates were primary sources. When death certificates were missing and ethnicity was uncertain, other information in the files was reviewed, including notes written in Spanish or another language, hospital records, fingerprint sheets, and FBI records, as well as an identification code unique to District 11, a stamp indicating the person was from Mariel, Cuba.
RESULTS
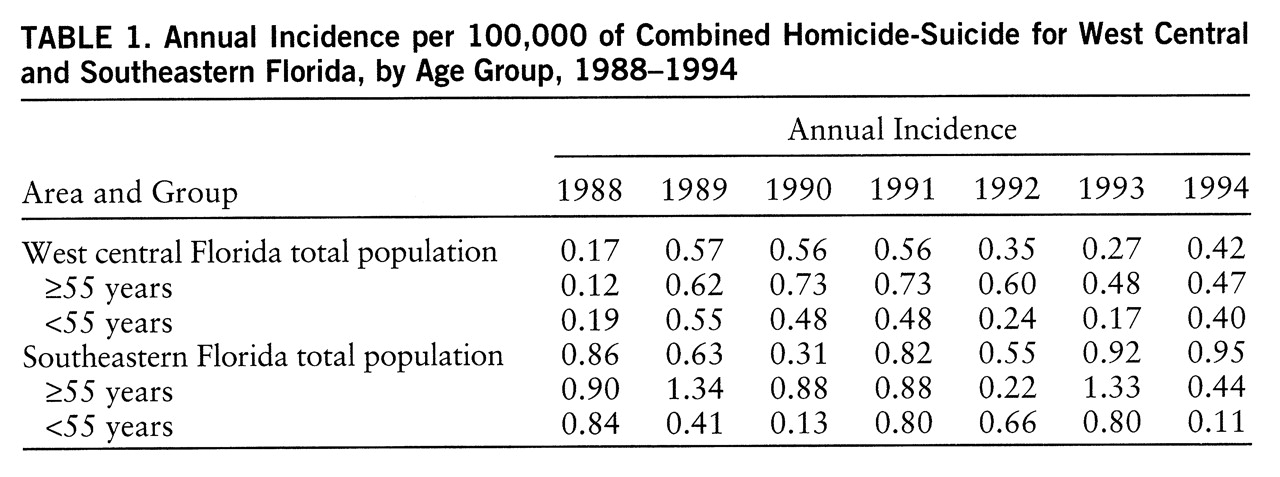
A total of 171 homicide-suicide events were identified between 1988 and 1994. The annual incidence rates for ho~micide-suicides over the 7-year period ranged from 0.4 to 0.9 per 100,000 persons age 55 and older and 0.3–0.7 per 100,000 for persons under age 55. The base rates for the older population were higher than those for the young every year except 1988 and 1994.
Table 1 shows the annual incidence rates by region. Perpetrators in the older age group were always men, and they committed 34% of the homicide-suicides, which accounted for 12.0% of all homicides and 2.4% of all suicides in this age group. The younger perpetrators were almost always men, and they committed 66% of the homicide-suicides, 2.5% of all homicides, and 3.8% of all suicides in this age group.
In west central Florida 88% of the homicide-suicides were spousal/consortial, compared to 75% of homicide-suicides in southeastern Florida. The remaining homicide-suicides in the older population of west central Florida included four familial homicide-suicides, all brothers and sisters, compared to three familial homicide-suicides and three nonfamilial homicide-suicides in southeastern Florida. The remaining homicide-suicides in the young population in southeastern Florida included four familial homicide-suicides, six filicide-suicides, and nine nonfamilial homicide suicides, compared to three familial homicide-suicides and two nonfamilial homicide-suicides in west central Florida.
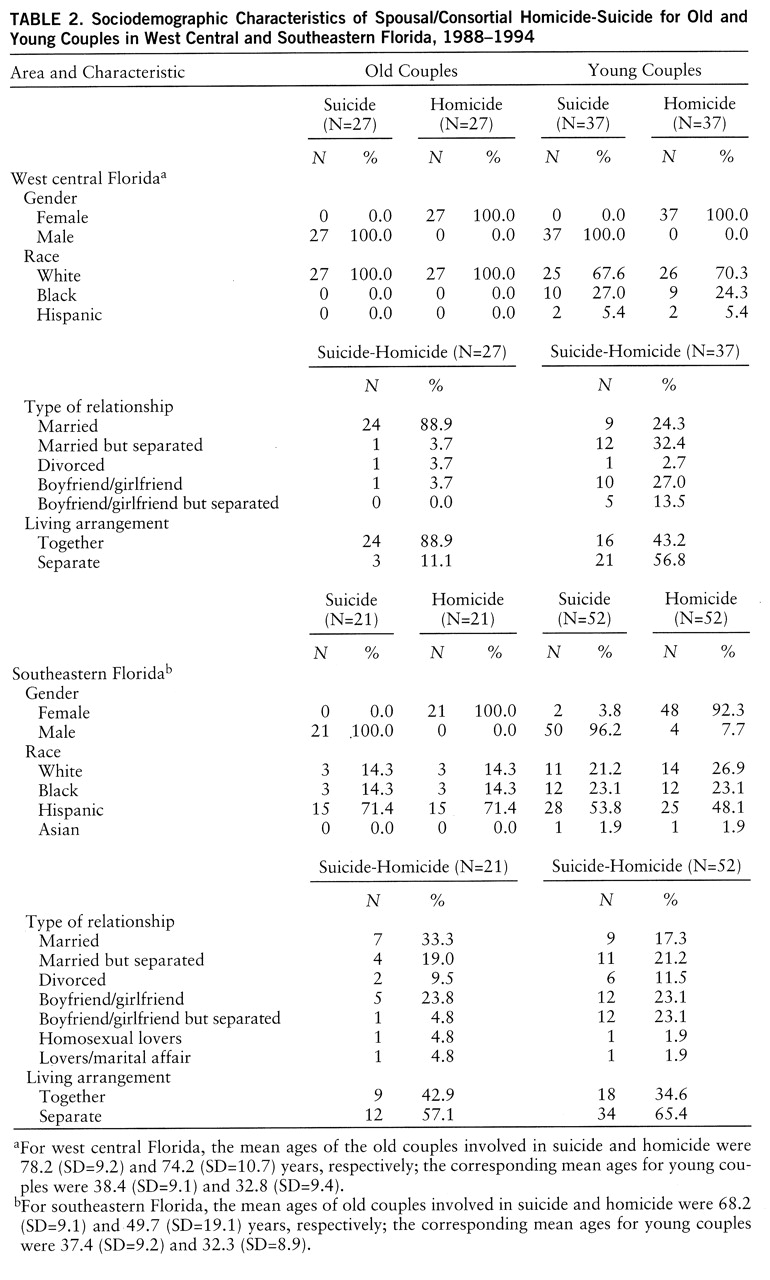
Sociodemographic characteristics of spousal/consortial homicide-suicide by age and region are shown in
table 2. In west central Florida the cases were all white older couples, almost always married and living together. The perpetrators were approximately 4 years older than their victims. This is in contrast to southeastern Florida, where more than two-thirds of the older couples were Hispanic and significantly younger than the west central cases. The perpetrators were 10 years younger than the west central Florida perpetrators and about 18 years older than their female victims. Less than half of the older southeastern couples lived together or were married.
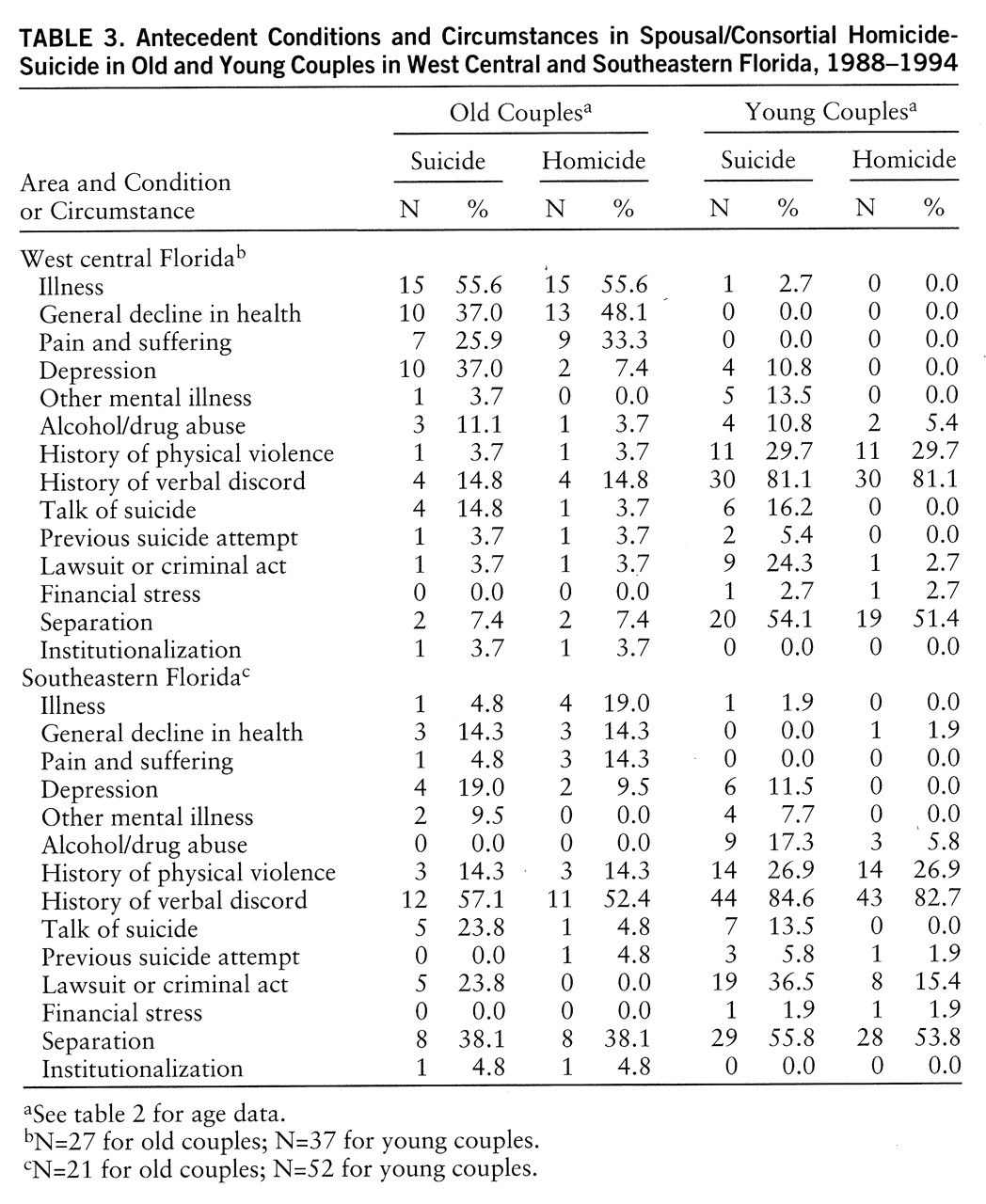
Table 3 shows that the antecedent conditions of the older couples were markedly different in the two regions, in contrast to the younger couples, who were similar to each other. Investigative information about the older couples in west central Florida suggests that both the perpetrator and victim were ill or in failing health more than half the time, with pain and suffering reported for 25% of perpetrators and 33% of victims. Physical violence was rare, but verbal discord was reported for 15% of couples. By contrast, for the older couples in southeastern Florida, health issues were less frequent, although homicide victims were sicker than perpetrators. Physical violence was prominent (14.3% and 3.7% in southeastern and west central Florida, respectively), and older perpetrators in southeastern Florida were five times more likely to be involved in a lawsuit or criminal activity than those in west central Florida.
The information available from reports suggested the presence of mental health problems in most perpetrators. In west central Florida, the following features were identified in the medical examiner records of the older perpetrators: 37% were depressed, 11% were abusing alcohol or drugs, 15% had talked about suicide, and 4% had previously attempted suicide. In southeastern Florida depression was described for 19% of the older perpetrators, other mental illness in 10%, and talk of suicide in 24%. Physical separation was reported for 38% of the older couples in southeastern Florida, compared to 7% in west central Florida.
The younger couples showed strikingly similar circumstances in both Florida regions. A history of verbal discord was recorded for more than 80% of couples and physical violence for more than 25% of couples. More than half were separated at the time of the homicide-suicide. A lawsuit or criminal circumstance was noted for more than 25% of the perpetrators but was less common for victims. Eleven percent of the perpetrators, but none of the victims, were reported to be depressed.
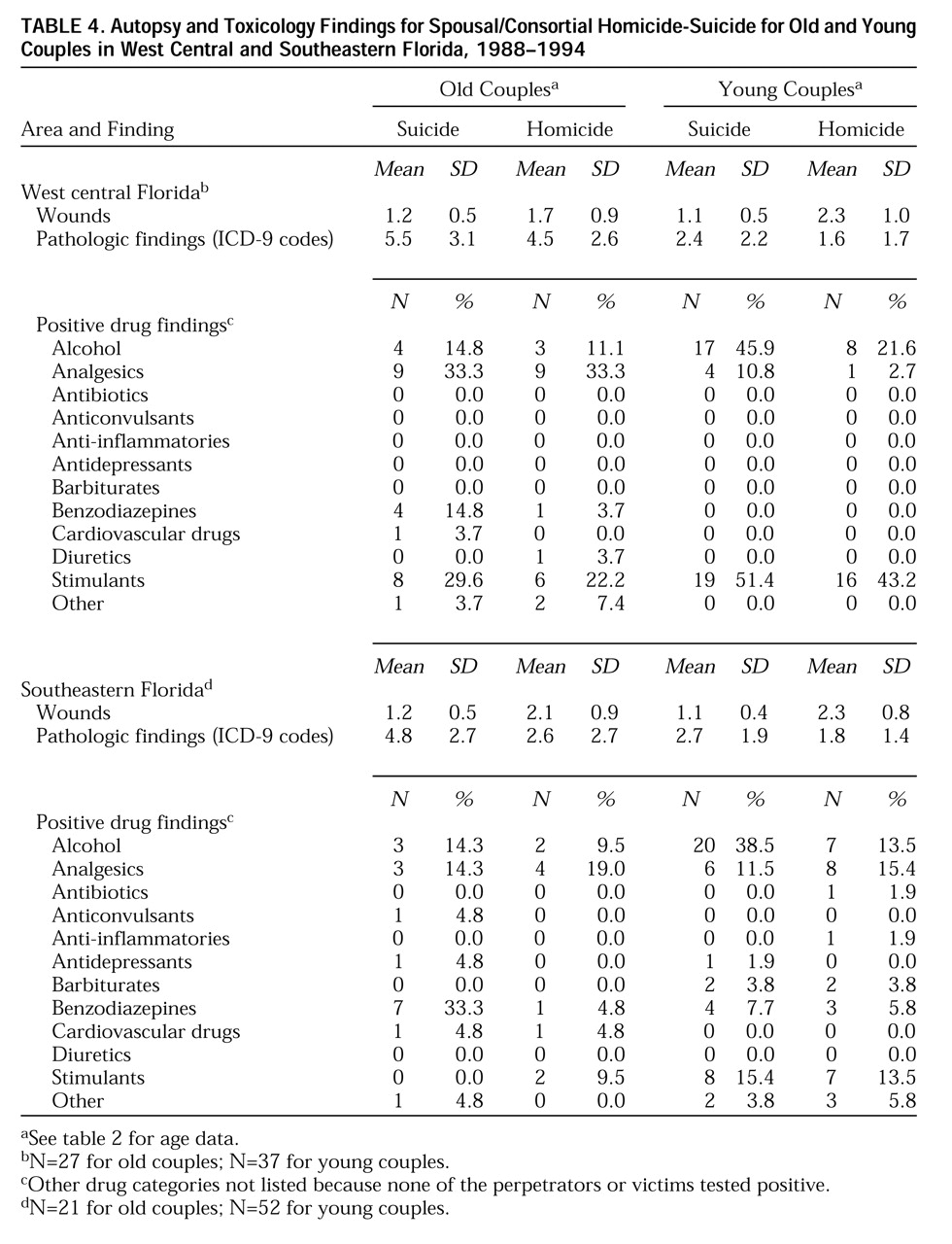
Table 4 describes autopsy findings by age group and region. For one-third of the older couples in west central Florida, drug test results were positive for analgesics; this rate is about twice as high as that observed in the older couples in southeastern Florida. Benzodiazepine use was four times higher in the older west central perpetrators than in their victims and was six times higher in the southeastern perpetrators than in their victims. Stimulant use was infrequent in the older couples in southeastern Florida, but about one-third of the west central perpetrators and one-fifth of the older victims tested positive for stimulants. Only one older perpetrator and one younger perpetrator in southeastern Florida tested positive for antidepressants, and none tested positive for antipsychotics. Alcohol was prominent in the younger couples in both regions, but stimulants were three times higher in the young west central couples.
DISCUSSION
Our results showed annual incidence figures for homicide-suicides from 1988 to 1994 that were higher than previously published rates, and the older population had higher rates than the younger group for all but 2 years. To our knowledge, this is the first report of the incidence and characteristics of homicide-suicide in an older population group. Because the Florida counties surveyed had high concentrations of older people and there are no other published data on homicide-suicide rates in older persons, it is not possible to know whether our results are a demographic artifact or due to a true higher rate of homicide-suicide in older adults.
There are a number of actual and potential biases affecting the count of homicide-suicide cases, and our rates are probably conservative estimates of the annual incidence in these regions. Since there are no systematic surveillance or reporting systems for homicide-suicides, the available case series has a selection bias. Medical examiner records are often used to study the epidemiology of fatal injuries, but overall, these records report only about two-thirds of lethal injuries, and underreporting is more pronounced in older age groups and women (
15). Our search of newspaper databases reinforced this ascertainment bias.
The prominent role of men as perpetrators of homicide-suicide is consistent with evidence of lethal violence against women over the past 25 years (
12). Our results confirm earlier findings that female homicide victims are consistently younger than perpetrators. Previous research on fatal violence in spouses for homicide only in the United States demonstrated a greater risk of homi~cide victimization as the age difference between husband and wife increased (
16,
17), and this difference was especially apparent in the older homicide-suicide couples in southeastern Florida.
The consistency of homicide-suicide rates reported in previous studies has been attributed to the constancy of depression and other psychiatric problems in adult populations. Depression has been implicated in homicide, suicide in older men, and homicide-suicide of couples (
18–
20). The high rates of homicide-suicide in our older Florida couples may reflect the lethal consequences of depression and hopelessness in male caregivers (
21,
22). As people continue to live longer, with the greater likelihood of comorbidity, frailty, and disability, including Alzheimer's disease and related disorders, spouse caregivers will continue to be at high risk for depression and other psychiatric disorders (
23). The hypothesis that the rate of homicide-suicide is increasing in the older population has important psychiatric and public health implications.
Although psychopathology is strongly implicated, homicide-suicides are probably multidimensional events, associated with the additive or multiplicative effects of many circumstances that lead to the emergence of homicidal-suicidal behavior. The use of drugs and alcohol, adverse life events, health status, psychosocial and cultural factors, relationship issues, and environmental features, e.g., availability of guns, have all been implicated (
1–
3,
24,
25). Our results suggest promising leads, but psychological autopsy studies are necessary to clarify clinical and biopsychosocial antecedents. Establishing a psychiatric diagnosis is difficult when both the perpetrator and victim are dead, but a recent report has described a psychological autopsy methodology to derive an axis I diagnosis in older suicide victims (
26). Only seven of the young perpetrators in our study were noted in the files as having a history of psychiatric treatment, compared to four of the older male perpetrators. Furthermore, the observation that only one of the older perpetrators and only one of the younger perpetrators tested positive for antidepressants, despite reports of depression, caregiver stress, and suicidal ideation, suggests the importance of education for primary care practitioners who routinely miss depression in the general population, but particularly in the aged (
23).
Our results suggest that the two subtypes of spousal/consortial homicide-suicide do not accurately reflect the complexity of homicide-suicide in couples. Separation, jealousy, and verbal and physical violence were common circumstances not only in the young groups in both regions, but also in the older group in southeastern Florida, in contrast to the older couples in west central Florida, in whom illness and pain were more common. The separation and marital discord in the older group in southeastern Florida, typically attributed to younger persons, suggest that jealousy and interpersonal problems played an important role in a predominantly Hispanic group in which older men were married to or involved with younger women.
Even though homicide-suicides in the United States are rare, relative to the number of suicides (approximately 30,000 per year [27]) and the number of homicides (approximately 22,000–24,000 per year [28]), further research is important to clarify whether homicide-suicide rates are increasing, especially in the aged. Persons over age 65 rarely commit homicides, but they have the highest suicide rates of any age group (20 per 100,000), with even higher rates in Florida (23 per 100,000) (
29). A recent report from the Centers for Disease Control (
30) indicated that suicide rates in the over-age 65 population increased from 1980 to 1993 in the United States, with an even greater increase in Florida. Suicide, homicide, and homicide-suicide are violent lethal actions that warrant epidemiologic study as well as clinical research in areas of assessment, prediction, intervention, prevention, and the interrelationship between these causes of violent death.
Since homicide-suicides are so complex, the definition and types of homicide-suicide are important methodological considerations in future research. Our findings suggest that the homicide-suicide continuum, at least for spousal/consortial events, includes completed events, nonfatal attempts at homicide and/or suicide, gestures, and ideation. Since these behaviors and thoughts are different from one another, it is likely that antecedent variables are different and that there are also variations within each of these categories. Therefore, accurate assessment and prediction of spousal/consortial homicidal-suicidal behaviors require definitions of the dependent variable to include subtypes. This will be a methodological challenge for such rare events.
Accurate descriptions of epidemiologic patterns, risk groups, and risk factors associated with homicide-suicide are the first step to developing intervention and prevention strategies. It is important to replicate our results, and long-term prospective studies are needed to test hypotheses about prediction and assessment. Research using psychological autopsy methods is essential to clarify the role of psychopathology as well as the intentionality and heterogeneity of motivations. Although depression, schizophrenia, and other mental disorders are strongly implicated, homicide-suicides are violent events with multiple cultural, psychosocial, health, and environmental antecedents. Homicide-suicides are probably the result of additive and/or multiplicative effects of diathesis, including culture, as well as multiple biopsychosocial and environmental stressors. Future research should clarify these interactions in order to better understand what mediates susceptibility to spousal/consortial homicide-suicide, in contrast to homicide or suicide.