Depressed patients often have psychomotor retardation, reduced mental processing speed, inability to make decisions, and inappropriate social responses (
1). These symptoms may be mediated in part by cortico-striato-pallido-thalamo-cortical pathway dysfunction (
1). Cortico-striato-pallido-thalamo-cortical pathway abnormalities result in dysfunctions in volition and purposive action, which are evident as deficits in initiation and errors in perseveration during cognitive tasks (
2). Geriatric depression often develops in the context of vascular disease, which may compromise the cortico-striato-pallido-thalamo-cortical pathway (
3). Measuring latency for the P300 response is a physiological means of examining the speed of psychomotor performance (
4); P300 latency has been found to be prolonged in patients with carotid arteriosclerosis (
5). For this reason, in this study we compared P300 latency in depressed geriatric patients with P300 latency in nondepressed elderly subjects.
The hypotheses tested were that 1) depressed geriatric patients have longer P300 latency than normal elderly subjects and 2) in depressed patients, longer P300 latency is related to deficits in initiation and errors in perseveration, and risk factors for vascular disease are associated not only with P300 latency but also with deficits in initiation and errors in perseveration.
METHOD
The subjects were 43 nondemented elderly patients with a diagnosis of major depression and 24 comparison subjects who were older than 60 years of age and who had no history of stroke. Depressed patients were included if they met Research Diagnostic Criteria (RDC) for unipolar major depression and had a score of 16 or higher on the 21-item Hamilton Depression Rating Scale. Age at onset of depression was determined during a clinical interview with the Schedule for Affective Disorders and Schizophrenia (SADS). The comparison subjects were also interviewed with the SADS, which revealed that none had a history of major psychiatric illness. Written informed consent was obtained from all subjects.
Cognitive capacity was assessed by using the Mattis Dementia Rating Scale (
6). Scores on the initiation/perseveration subscale of the Mattis Dementia Rating Scale were used to detect deficits in initiation and errors in perseveration. This subscale assesses the executive functions of volition, cognitive flexibility, resistance to perseveration, response inhibition, and motor control by using double alternating manual motor items, graphomotor copying, and category fluency tasks.
Risk factors for vascular disease were assessed by using the Framingham Stroke Risk Profile (
7). The patients were in a psychotropic-drug-free state for at least 3 days before assessments were made except for prescriptions of lorazepam as needed for five patients.
P300 was elicited on a Nicolet CA-2000 system. Subjects were tested following breakfast. EEG was recorded from Fz, Cz, and Pz sites, referenced to linked mastoids and bandpass-filtered at 0.5–30 Hz. The signals were 1 kHz standard, and 2 kHz target tones (ratio=4:1) were delivered binaurally every 1.1 seconds at 70 decibels (SPL) above hearing level. The subjects pressed a switch held in the right hand each time they detected a target tone. Between 40 and 50 artifact-free trials for targets were obtained. The responses were averaged on-line. The P300 wave was identified by a positive-negative-positive (P2-N2-P3) complex in the target response at the range of 280–600 msec, and maximal at the central and parietal sites (
8). Latency was measured at the intersection of extrapolating lines from the ascending and descending portions of the P3 wave. If two peaks for P300 were seen within the main peak, the whole peak was scored as a single peak. If the peaks were distinct, the second peak was scored for latency (
8).
Group comparisons were performed by using the Wilcoxon rank sum test because of the skewed distribution of clinical variables and their unequal variance. The differences in P300 latency were examined by using a robust generalized linear model, adjusted for the effects of clinical variables (
9). The relationship between P300 latency and domain scores for the five Mattis Dementia Rating Scale domains was examined by using Canonical correlation. The relationship among risk factors for vascular disease, P300 latency, and deficits in initiation and errors in perseveration was examined by using partial correlations.
RESULTS
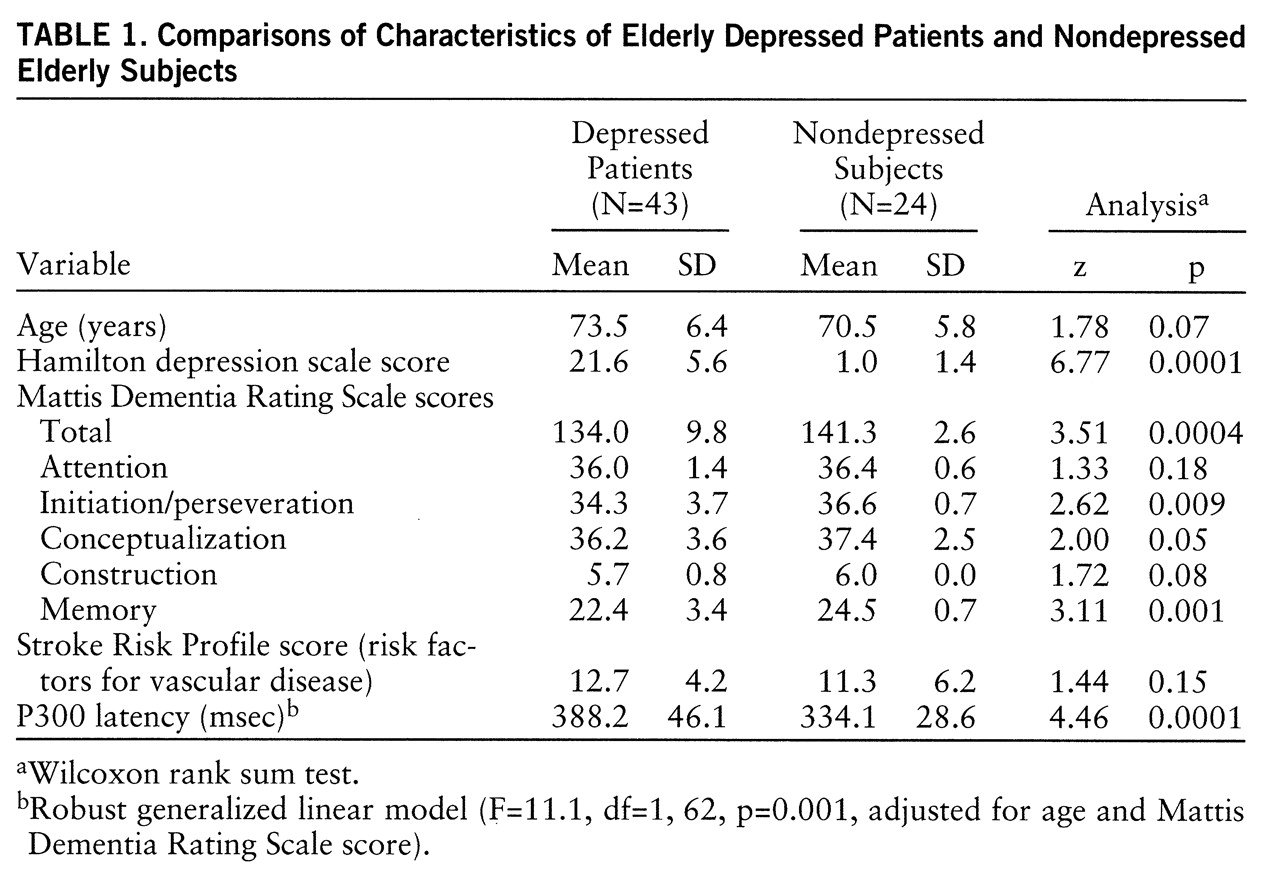
All subjects identified more than 85% of the target tones. Depressed patients had longer P300 latency than nondepressed subjects (F=11.1, df=1,62, p=0.001; robust generalized linear model adjusted for age and Mattis Dementia Rating Scale scores) (
table 1).
The P300 latency obtained in comparison subjects was used to construct an age-latency regression line. According to a convention used in electrophysiology (
8), normal P300 latency is defined as values within two standard errors of the age-latency regression line (
8). On the basis of this convention, abnormal latency was noted in four of 24 comparison subjects and 29 of 43 depressed patients (Yates-corrected χ
2=16.5, df=1, p=0.0002). There was no relationship between latency and age at onset of depression. Eighteen of 21 patients with depression onset after age 60 years had abnormal latency compared with eight of 14 patients with depression onset before age 60 years (Yates-corrected χ
2=2.25, df=1, p=0.13). There was no difference in P300 latency between the 28 patients with an RDC diagnosis of definite endogenous depression (mean=386.8 msec, SD=43.7) and the 15 patients who had probable endogenous depression or nonendogenous depression (mean=370.4, SD=31.8) (F=0.90, df=1,40, p=0.34, age-adjusted analysis of covariance).
In depressed patients, P300 latency was related to deficits in initiation and errors in perseveration (r=0.62, p=0.01, age-adjusted partial correlation). Canonical correlation of P300 latency with scores for the five Mattis Dementia Rating Scale domains showed P300 latency to be associated with deficits in initiation and errors in per~severation (r=0.65) (F=5.09, df=5,36, p=0.001, age-adjusted Wilks's lambda). Deficits in initiation and errors in perseveration had the largest loading (0.96) on the standardized Canonical coefficient.
In depressed patients, risk factors for vascular disease were associated not only with P300 latency (r=0.38, p=0.01, age-adjusted partial correlation) but also with deficits in initiation and errors in perseveration (r=0.32, p=0.04, partial correlation). However, when both P300 latency and age were taken into account, the score for risk factors for vascular disease was not correlated with deficits in initiation and errors in perseveration (r=0.11, p=0.46, partial correlation). Similarly, the score for risk factors for vascular disease was not correlated with P300 latency when the variance accounted for by deficits in initiation and errors in perseveration and age were taken into consideration (r=0.24, p=0.13, partial correlation).
DISCUSSION
The principal finding of this investigation was that P300 latency is prolonged in geriatric major depression. In depressed patients, P300 latency was correlated with deficits in initiation and errors in perseveration. The prefrontal cortex is a modulator for the P300 response (
10), and deficits in initiation and errors in perseveration are associated with prefrontal abnormalities (
2). The association of P300 latency with deficits in initiation and errors in perseveration identified by this study suggests that these measures reflect related prefrontal dysfunction in elderly depressed patients. Both of these measures in elderly depressed patients appear to be related to risk factors for vascular disease.
Our finding of prolonged P300 latency in geriatric depressed patients differs from the findings of others (
11,
12), who observed no differences in P300 latency between geriatric depressed patients and normal comparison subjects. Differences in amplitude, however, have been noted in young depressed patients compared with control subjects (
13). The studies in the elderly were based on smaller numbers of depressed patients (seven to 11 subjects), whose task performance varied considerably (
11). In contrast, the subjects of the present study identified more than 85% of the target tones that are critical for eliciting P300 (
4).
It has been proposed that some depressive syndromes may result from disruptions of the cortico-striato-pallido-thalamo-cortical pathways or their connections to monoaminergic centers (
1,
3). It is conceivable that this may explain the difference found in P300 latency between groups. However, nonpsychotropic medications prescribed for medical illnesses may also help explain the latency differences. In this study, depressed patients had longer P300 latency and deficits in initiation and errors in perseveration than nondepressed subjects, although their risk factors for vascular disease scores were similar. Differences in the site of vascular lesions may account for this finding. A speculation may be that the depressed group had lesions impairing the cortico-striato-pallido-thalamo-cortical pathways, resulting in depressive syndromes associated with prolonged P300 latency and deficits in initiation and errors in perseveration, while the comparison group had lesions in other brain regions. This study was a preliminary exploration of these relationships using clinical measures for vascular disease. Therefore, these findings do not conclusively support the relationship between vascular disease and geriatric depression. Further research may be pursued with brain imaging studies of the prefrontal area and basal ganglia, as well as tests of specific prefrontal functions.