Managed care companies are applying increasing pressure on clinicians to transfer nonsuicidal, medically stable patients with anorexia nervosa from inpatient care to less intensive treatment early in their hospital course. Insurance reviewers often fail to consider possible indicators of a poor short-term prognosis for early transition when making these demands. Shorter inpatient hospital stays minimize immediate treatment cost, but a recent report
(1) concluded that, at least for depressed patients, shorter admissions “may place them at greater risk for adverse outcomes in the immediate posthospital period.”
Most treatment outcome and prognostic studies for anorexia nervosa have focused on intermediate to long-term outcome. Some of the variables associated with poor outcome include a very low body weight, longer duration of illness, older age at onset, and disturbed family relationships
(2,
3). Other factors that may be associated with poor outcome include greater intensity and frequency of eating disorder signs and symptoms, psychiatric axis I and axis II comorbidity, the presence of bulimic symptoms, and lower socioeconomic status. These factors are by no means universally accepted. Opposite associations exist, and there are numerous findings of no association
(4). Regardless of which long-term factors are well accepted, however, short-term prognostic factors may or may not be the same as intermediate or long-term factors. There is a relative absence of studies determining either predictors of short-term outcome or decision rules for when to transfer patients with anorexia to a less intensive level of care.
In 1995, Nozoe et al.
(5) suggested that many of the factors frequently associated with poor long-term outcome for anorexia nervosa (most important, older age at admission and lower minimum body weight after onset) may also predict increased duration of inpatient treatment. The work of two groups, Baran et al.
(6) and Hebebrand et al.
(7,
8), supports the critical importance of body weight in anorexia treatment outcome. Baran et al.
(6) reported that a lower inpatient discharge weight was associated with higher rates of rehospitalization. Hebebrand et al.
(7,
8) reported that a lower weight at referral, as measured by absolute body mass index or percentage of normal body mass index, was associated with less frequent attainment of normal body mass index at intermediate to long-term follow-up and a greater risk of chronic anorexia and death. Our study was designed to determine what other individual characteristics, in addition to body weight, can be used to predict success versus failure of rapid transfer to a day hospital program for inpatients with anorexia nervosa.
METHOD
Study Cohort
The study group consisted of 59 women who were consecutively admitted to a university eating disorder day hospital program as transfers from an inpatient unit. Fifty-seven of the patients were transferred from an eating disorder specialty unit, and two patients were transferred from other services. All patients had to meet DSM-IV criteria for anorexia nervosa or subsyndromal anorexia nervosa at the time of admission to the inpatient unit. Patients with a primary diagnosis of bulimia nervosa were excluded. Subjects with more than one admission to the day hospital program were included only once in the analysis to avoid biasing the results with overrepresentation of those patients.
Psychiatric Diagnoses
Three of the authors (W.T.H., K.K.E., and C.V.Q.), all of whom are mental health professionals with experience treating individuals with eating disorders, made the diagnoses of anorexia nervosa according to DSM-IV criteria after reviewing the medical records and the typed admission histories and discharge summaries. Assignment of psychiatric diagnoses other than eating disorders was based primarily on admission and discharge diagnoses.
Individuals who had a body mass index less than 95% of normal for a given age and sex and who met all but one of the following two DSM-IV criteria for anorexia nervosa (body weight less than 85% of expected or amenorrhea) were assigned a diagnosis of subsyndromal anorexia. According to DSM-IV nomenclature, these patients would qualify for the diagnosis of eating disorder not otherwise specified. The DSM-IV criterion of less than 85% of expected weight for the diagnosis of anorexia nervosa represents an arbitrary cutoff point between normal and abnormal weight, and Garfinkel et al.
(9) suggested that the presence of amenorrhea is not important for the diagnosis of anorexia nervosa when all other criteria are met.
Anthropometric, Psychometric, and Quantitative Measurement
Body mass index is calculated by dividing an individual’s weight in kilograms by the square of their height in meters. In DSM-IV, the weight criterion for anorexia nervosa is less than 85% of the normal weight for a given age, height, and sex. In the World Health Organization’s ICD-10, the weight criterion for anorexia nervosa is a body mass index of less than or equal to 17.5. For females 15 to 29 years old, body mass index values in the range of 17 to 19 correspond to the 85% DSM-IV requirement
(10). A disadvantage of the body mass index value is that it does not take into consideration an individual’s age and sex. Percentage of expected weight, in comparison, is limited by dependence on one of many nonidentical reference tables. If an individual’s body mass index value is divided by the median value for a given age and sex, the result when multiplied by 100 is the percentage of normal body mass index. Percentages of normal body mass index values in this study are based on median body mass index values obtained from the First National Health and Nutrition Examination Survey
(11), which collected data from a representative, noninstitutionalized, U.S. sample (N=28,043) in 1971 to 1974.
Bone density results are from dual-energy X-ray absorptiometry. The term “osteopenia” is used to indicate a bone density between one and two standard deviations below the maximum expected bone density for sex-matched normal subjects. The term “osteoporosis” indicates a bone density of more than two standard deviations below normal (
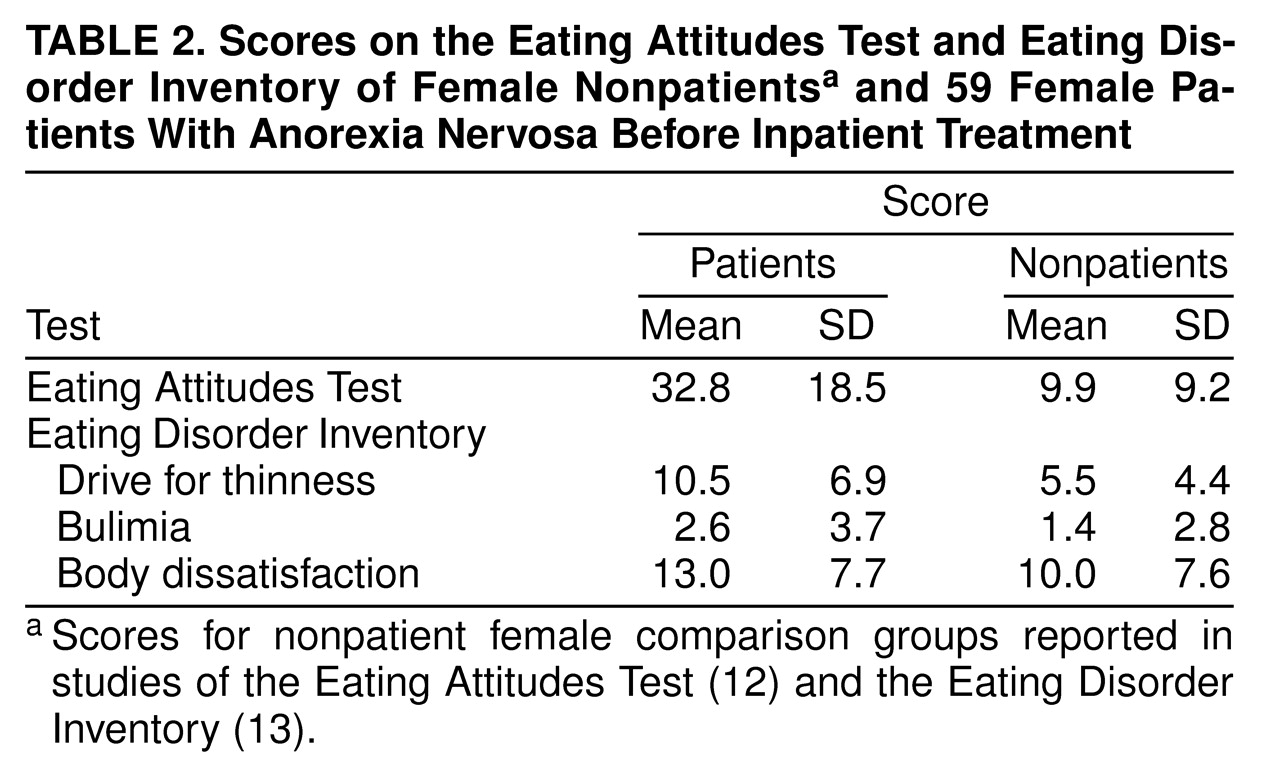
table 1). Both the Eating Attitudes Test
(12), and the Eating Disorder Inventory
(13) were administered at the beginning of the inpatient unit admission. Only the first three scales of the Eating Disorder Inventory—drive for thinness, bulimia, and body dissatisfaction—were screened for their possible predictive value.
Data Acquisition and Management
Data collection involved completion of a systematic form for the abstraction of data from medical records; this form included a variety of anthropometric, demographic, illness history, and psychometric variables. Data were entered by two of us (W.T.H., C.V.Q.) in a computer using the program Epi Info
(14). We used data quality control features of Epi Info, including programming of all fields to be entered with specified legal values and allowed ranges.
Data Analysis
For the purpose of screening the potential predictive value of variables, day hospital treatment outcome was divided into two categories, success or failure. The outcome categories of success and failure were also used for risk ratio calculation. Successful treatment outcome is defined by individuals who, after being accepted in transfer from an inpatient unit, received a regular discharge from the day hospital program. The treatment failure group includes individuals who either relapsed in the day hospital and required transfer back to an inpatient unit or were discharged against medical advice from the day hospital program. Decisions regarding whether to readmit a patient to the inpatient unit from the day hospital were made on an individual basis by the treatment team. Reasons for readmission varied and included repeated food refusal, weight loss or failure to continue weight restoration, excessive exercise, or the persistent use of laxatives or diuretics.
To screen for an association between potential risk factors and adverse outcome, all demographic and clinical variables in
table 1 were evaluated with one exception—rate of weight gain in the day hospital. This variable represents a form of day hospital treatment outcome, not a potential risk factor measured on the inpatient unit. Categorical variables were screened by using the chi-square test or Fisher’s exact test, where appropriate, for association with treatment outcome (success or failure). Means of continuous variables for the two outcome groups (success or failure) were compared by using two-tailed two-sample t tests.
A maximum chi-square or t test screening p value of 0.05 was used for this first stage of potential risk factor identification. When the p value for a stage-one screening test was less than 0.05, the second stage of risk factor assessment involved dichotomizing the variable in an attempt to find a meaningful or natural cutoff point in the frequency distribution and to allow calculation of a risk ratio.
The uncorrected risk ratio and associated 95% confidence interval for a variable measure the risk that an individual with the particular characteristic, as measured on the inpatient unit, will fail day hospital treatment, compared with individuals without the characteristic. Hence, these are measures of relative risk. A risk ratio greater than 1 suggests a poor prognosis for someone with the given characteristic, whereas a risk ratio smaller than 1 suggests a relatively good prognosis. A risk ratio of 1 indicates no association between a given risk factor and outcome. A risk ratio whose confidence interval does not contain the number 1 is significant at p≤0.05. The magnitude of the risk ratio is also important. A risk ratio of 10, for example, indicates that an individual with the given characteristic is 10 times more likely than someone without the characteristic to fail day hospital treatment.
RESULTS
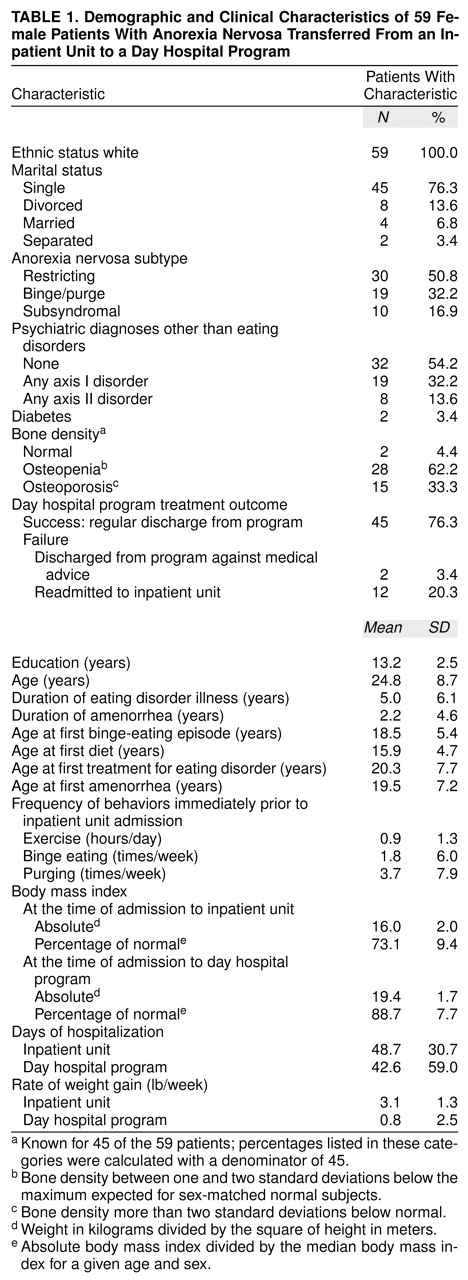
All 59 patients were female Caucasians, the majority were single, and their mean age was 24.8 years (
table 1). Most had the restricting subtype of anorexia nervosa (
table 1). Individual psychiatric diagnoses other than eating disorders were not screened for their predictive significance because so few patients had such diagnoses and are therefore not included in
table 1. Two individuals (3.4%) had diabetes, and 43 (96%) of the 45 women whose charts contained the results of a bone scan had at least moderately insufficient bone density, qualifying for either osteopenia or osteoporosis (
table 1).
Fourteen (24%) of the 59 patients were considered failures in day hospital treatment, defined as either needing readmission to an inpatient unit or receiving a discharge against medical advice from the day hospital program (
table 1). The mean rate of weight gain on the inpatient unit was approximately four times the mean rate of weight gain in the day hospital. The patients’ mean body mass index was 16.0 at admission to the inpatient unit; this increased to 19.4 by the time of transfer to the day hospital program. The mean duration of inpatient treatment was 48.7 days, and mean duration of day hospital treatment was 42.6 days (
table 1).
Table 2 presents the scores of the 59 patients at inpatient admission compared with scores of female nonpatients on the Eating Attitudes Test
(12) and the Eating Disorders Inventory
(13).
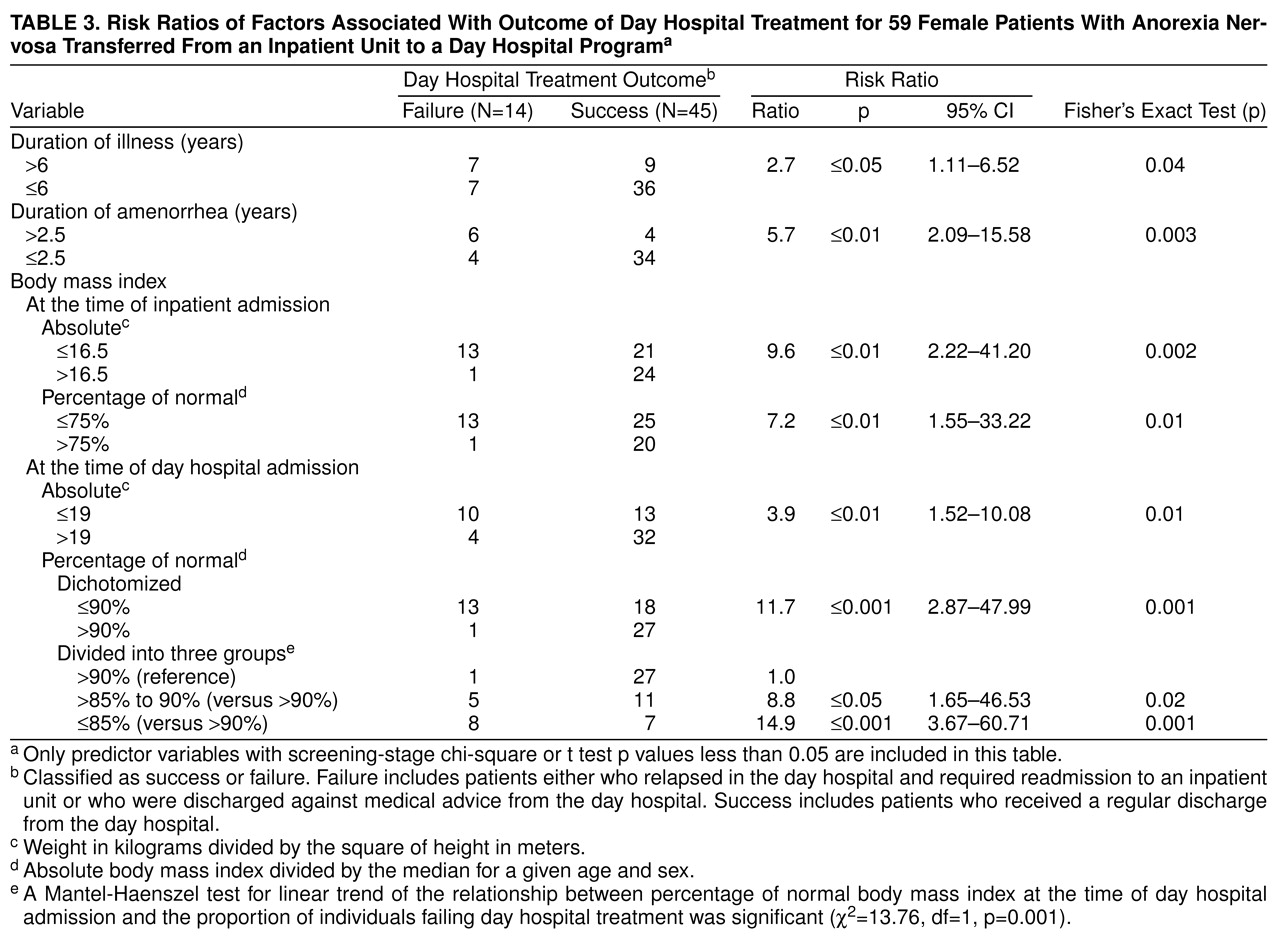
The risk ratios for predictor variables identified in the stage-one screening process are presented in
table 3. Both of the patients with diabetes failed the day hospital program, but this finding just missed the significance level required by the stage-one variable screening process (p=0.05). Variables in
table 3 with a risk ratio for failing day hospital treatment significant at p=0.05 include the following: greater than 6 years of illness, greater than 2.5 years of amenorrhea, a body mass index at the time of inpatient admission of 16.5 or less or 75% or less of normal, and a body mass index at the time of transfer to the day hospital program of 19 or less or 90% or less of normal.
Individuals transferred to the day hospital program with a body mass index between 86% and 90% of normal were at approximately nine times greater risk of failing day hospital treatment than individuals transferred with a body mass index greater than 90% of normal, and the relative risk increased to 15 for individuals with a body mass index less than or equal to 85% of normal. Of the 28 women transferred to the day hospital program with a body mass index above 90% of normal, only one (3.6%) failed day hospital treatment (
table 3). When the body mass index at the time of transfer was between 86% and 90% of normal, 31.3% failed day hospital treatment, and the percentage failing day hospital treatment increased to 53.3% for individuals transferred with a body mass index of 85% or less than normal. A Mantel-Haenszel test for a linear trend of the relationship between percentage of normal body mass index at the time of day hospital program admission and the proportion of individuals failing day hospital treatment was significant (
table 3).
DISCUSSION
The lack of ethnic variety seen in
table 1 is not unexpected because the location of the eating disorder day hospital program—Iowa City, Iowa—has a very small minority population. Furthermore, the insurance precertification screening process may be an indirect method of selecting patients with higher than average socioeconomic status.
The psychiatric comorbidity rates of 32.2% (axis I) and 13.6% (axis II) are in the low range of what was expected
(2), perhaps due to conservative classification resulting from relying primarily on admission and discharge diagnoses. Loss of bone mineral density is one of the most serious, common, and possibly reversible consequences of anorexia
(15). All patients with anorexia nervosa in this university treatment program receive calcium supplementation, and that practice seems justified in view of the fact that more than 95% of the patients in this study cohort met criteria for either osteopenia or osteoporosis.
Restoring the weight of patients with both anorexia nervosa and diabetes is a challenging task, and both of the patients with diabetes in this study failed day hospital treatment. The restoration of patients with both anorexia nervosa and diabetes usually involves an interdisciplinary team approach with frequent collaboration between dietary and endocrinology services. We recommend restoration to 100% of ideal body weight on an inpatient unit before transferring a patient with both anorexia and diabetes to a less intensive level of care.
One of the most consistently reported poor prognostic indicators in the long-term outcome literature for anorexia nervosa is a longer duration of illness
(3,
4). The two variables that measured the length of anorexia in this study—duration of illness and duration of amenorrhea—passed the screening process for predictor variables and are included in
table 3. Thus, longer duration of anorexia appears to predict short-term failure as well as long-term outcome.
The strongest association between any inpatient predictor variable and day hospital treatment outcome was found for percentage of normal body mass index on admission to the day hospital program. Individuals who were 90% or less of their ideal body mass index at the time of transfer to the day hospital program were more than 10 times more likely than someone above 90% normal body mass index to fail day hospital treatment and require either readmission to an inpatient unit or a discharge against medical advice. Furthermore, our data are consistent with a dose-response relationship between percentage of normal body mass index at the time of day hospital program admission and the risk of day hospital treatment failure.
We conclude that the percentage of normal body weight at the time of inpatient discharge and the duration of anorexia, measured either in years of illness or in years of amenorrhea, are the two most important predictors of short-term anorexia nervosa treatment outcome and unsuccessful transfer to a less intensive level of care.
The cost per day of this day hospital program is approximately one-third the cost of inpatient care; the average rate of weight restoration in the day hospital program is approximately one-fourth as fast as the rate on an inpatient unit (0.8 lb/week compared with 3.1 lb/week, respectively). Thus, the reduced expense of day hospital care compared with inpatient treatment appears to be offset by a slower rate of weight restoration. Of the patients who were transferred to the day hospital program when their body mass index was 90% or less than normal, more than one-third (13 of 31) failed day hospital care and needed readmission to an inpatient unit or were discharged against medical advice. Therefore, not only is inpatient weight restoration no more expensive than restoration in the day hospital program, but for individuals with less than 90% of normal body mass index, there is a strong economic advantage for continued inpatient treatment because it avoids the immediate relapse and readmission of more than one-third of those individuals.
The average rate of weight gain in the day hospital program for the treatment success group (1.2 lb/week) was higher than the value for the treatment failure group (–0.4 lb/week) (t=2.11, df=52, p=0.04). Only one of the 28 patients who were greater than 90% of a normal body mass index at the time they were transferred from an inpatient unit to the day hospital program failed day hospital treatment. Thus, day hospitalization appears to be an effective step-down treatment modality from 24-hour inpatient care for the continued treatment and restoration of individuals with anorexia nervosa, offering both an adequate rate of weight restoration and a low risk of immediate relapse, only for patients with 90% or more of healthy weight at the time of transition.
Limitations of the Study
Outcome misclassification was a possibility in this study. The day hospital treatment success group may be contaminated with individuals who deserved an against-medical-advice discharge but did not receive one. This potential misclassification would not be expected to introduce spurious associations, however, because including some treatment failures in the treatment success group would diminish differences between the two outcome groups. This should bias the results only toward the null hypothesis of no association.
Four additional study limitations will be mentioned. First, an individual’s eating disorder symptoms were measured with the Eating Attitudes Test and the Eating Disorder Inventory at the time of admission to the inpatient unit. Scores on these measures change significantly during the course of inpatient eating disorder treatment
(16). Therefore, it is entirely possible that these scores would predict day hospital treatment outcome if the tests were given at the time of admission to the day hospital program. Second, the presence of a comorbid psychiatric diagnosis on either axis I or axis II was not associated with adverse outcome; this may be a result of conservative diagnostic classification that was limited by the retrospective chart review method. Third, no multivariate analysis was presented. The chart review method of data acquisition resulted in frequent missing data, which in turn resulted in line-item deletions when attempting multivariate analyses. Attempts at multivariate analyses were also limited by the small number of individuals in the treatment failure group (N=14). For these reasons we focused on a two-stage univariate analysis that allowed for the initial screening of a large number of potential predictors (N=29) and closer inspection of only those variables associated with outcome (N=6).
Fourth and finally, the issue of multiple comparisons should be addressed. We screened for the predictive significance of all 29 variables in
table 1 and
table 2. Using a stage-one screening p value of 0.05, we might expect to find one or two variables associated with outcome by chance alone (one out of every 20 tested). We used a liberal uncorrected p<0.05 level for the first stage of the variable selection process to maximize sensitivity and to allow further inspection of potential predictors. Had a more stringent stage-one screening p value of 0.01 been used, all four measures of body mass index in
table 3 would still have passed the variable selection process, but neither years of illness nor years of amenorrhea would have passed. When variables passing the first screening stage were evaluated with risk ratios in
table 3, they were subclassified according to whether they were p≤0.05, p≤0.01, or p≤0.001. Five out of the six dichotomized risk factors in
table 3 were p≤0.01, and the strongest risk factor, percentage of normal body mass index at the time of admission to the day hospital program, was significant at p≤0.001. Furthermore, our a priori hypothesis was that individuals with a greater severity of illness would be at greater risk of failing the day hospital program; this supports the use of unadjusted p values for indicators of illness severity, including both duration of illness and duration of amenorrhea.
Clinical Recommendations and Future Direction
We recommend restoring the weight of individuals with anorexia nervosa in an inpatient setting until they are close to, if not greater than, 90% of their ideal body weight or normal body mass index. For individuals with anorexia and diabetes, we recommend restoration to full ideal body weight on an inpatient unit. It may make clinical and financial sense to try to transfer nondiabetic individuals with anorexia who are within 10% of their ideal body weight and have a relatively short duration of illness (fewer than 6 years) and amenorrhea (fewer than 2.5 years) to a less intensive level of care for the remainder of their treatment. Alternatively, inpatient restoration to 100% of their ideal body weight may be the more effective and efficient alternative for individuals who, even if within 10% of their ideal body weight, have a long history of amenorrhea and severe anorexia. Future prospective eating disorder treatment outcome studies will clarify further how to provide effective high-quality care that maximizes efficiency yet minimizes the chance of immediate relapse.