The gateway hypothesis holds that consumption of abusable drugs progresses in orderly fashion through several discrete stages
(1,
2) . The entire sequence, which is exhibited by only a small minority of drug users, begins with beer or wine and moves progressively through hard liquor or tobacco, marijuana, and finally hard drugs
(3) . Each stage is thus a component of both a temporal sequence and a hierarchy.
Kandel and Yamaguchi
(3) asserted that a causal linkage drives the sequence: “One licit drug is required to make the progression to marijuana use” (p. 71). This claim has not been empirically supported, however. Young et al.
(4) observed that marijuana was the first drug used by 42% of a sample of delinquent youths. Other researchers have reported that marijuana use is not a requirement for progression to hard drugs. Golub and Johnson
(5) found that 75% of inner-city heavy drug users began using cocaine before using marijuana. These authors also report that 1%–4% of hard drug users skipped both the alcohol/tobacco and marijuana stages
(6) . Mackesy-Amiti et al.
(7) reported that 39% of their sample started using marijuana after they had used hard drugs. Blaze-Temple and Lo
(8) reported that 29% of their sample began using marijuana after having used heroin, stimulants, or LSD.
The high rate of nonconformance with the “gateway sequence” notwithstanding, it is nevertheless the most common pattern, although the reasons remain obscure. One possible reason is that specific factors connect each successive stage of drug use comprising the overall sequence. According to Kandel and Yamaguchi
(3), “the identification of drug-specific risk factors for progression is technically related to the demonstration of causal linkages between stages” (p. 64). Alternatively, abuse of illicit drugs, whether or not preceded by use of licit compounds, may be more parsimoniously explained by their availability in the social environment and the level of the individual’s liability that is common to all abusable substances. For example, conduct problems in childhood presage consumption of all classes of abusable drugs. Genetic
(9 –
12), neurophysiological
(13,
14), neurochemical
(15,
16), and behavioral
(17,
18) investigations have shown that the same factors are associated with consumption of licit and illicit drugs. Indeed, 100% of the genetic variance in the risk for diagnosis of substance use disorder is common across all illicit substances
(10) .
Thus, two competing explanatory frameworks have been advanced to explain the transition from licit to illicit drug use. The gateway hypothesis
(3) holds that factors specific to the use of each drug determine the transition from one compound to the next in a meaningful causal sequence. The common liability model
(19), by contrast, specifies that the level of liability that is common to all abusable compounds accounts for the propensity to transition to illegal drugs.
This unresolved controversy has important policy and practical ramifications. For example, the presumption that specific risk factors are associated with the use of illicit drugs remains the cornerstone of U.S. drug policy (see, for example, Congressional Record, July 1999, pp. H6640–H6642). Similarly, the focus on illicit drugs by the White House Office of National Drug Control Policy tacitly assumes that the predisposing characteristics and the correlates of illegal drug use are different from those of licit drug use. Each perspective also has important implications for prevention of illicit drug use. Interventions framed conceptually within the gateway hypothesis emphasize breaking the pattern of drug use transitions by ameliorating the risk factors that cause use of the next drug in the sequence. The common liability model instead focuses on early childhood development, particularly socialization of normative attitudes and behavior, in which avoidance of illegal behavior, including marijuana use, is established.
In this prospective study, we sought to ascertain whether specific risk factors are associated with the transition from licit to illicit drug use. We used a panel of 35 variables encompassing individual, family, school, peer, and neighborhood characteristics to determine whether youths whose illicit drug use exhibited the gateway sequence are distinguishable from those whose use exhibited a reverse sequence (licit drug use following illicit drug use). We also sought to determine whether the gateway sequence has a superior (or at least different) capacity to predict substance use disorder and its rate of development between late childhood and young adulthood. Contrasting the gateway and reverse sequences provides an opportunity to evaluate the prognostic utility of the gateway pattern. On the basis of mounting evidence of common mechanisms that predispose individuals to consumption of abusable substances
(19), we hypothesized that 1) the first two stages constituting the gateway sequence—that is, use of licit drugs (alcohol and/or tobacco) and then use of illicit drugs (marijuana)—do not feature distinct characteristics; 2) in keeping with the common liability model, the propensity to progress to illicit drugs is due to general behavioral deviancy; and 3) there are no differences between youths who exhibit the gateway sequence (with licit drug use preceding marijuana use) and those who exhibit the reverse gateway sequence (with marijuana use preceding licit drug use).
Method
Participants
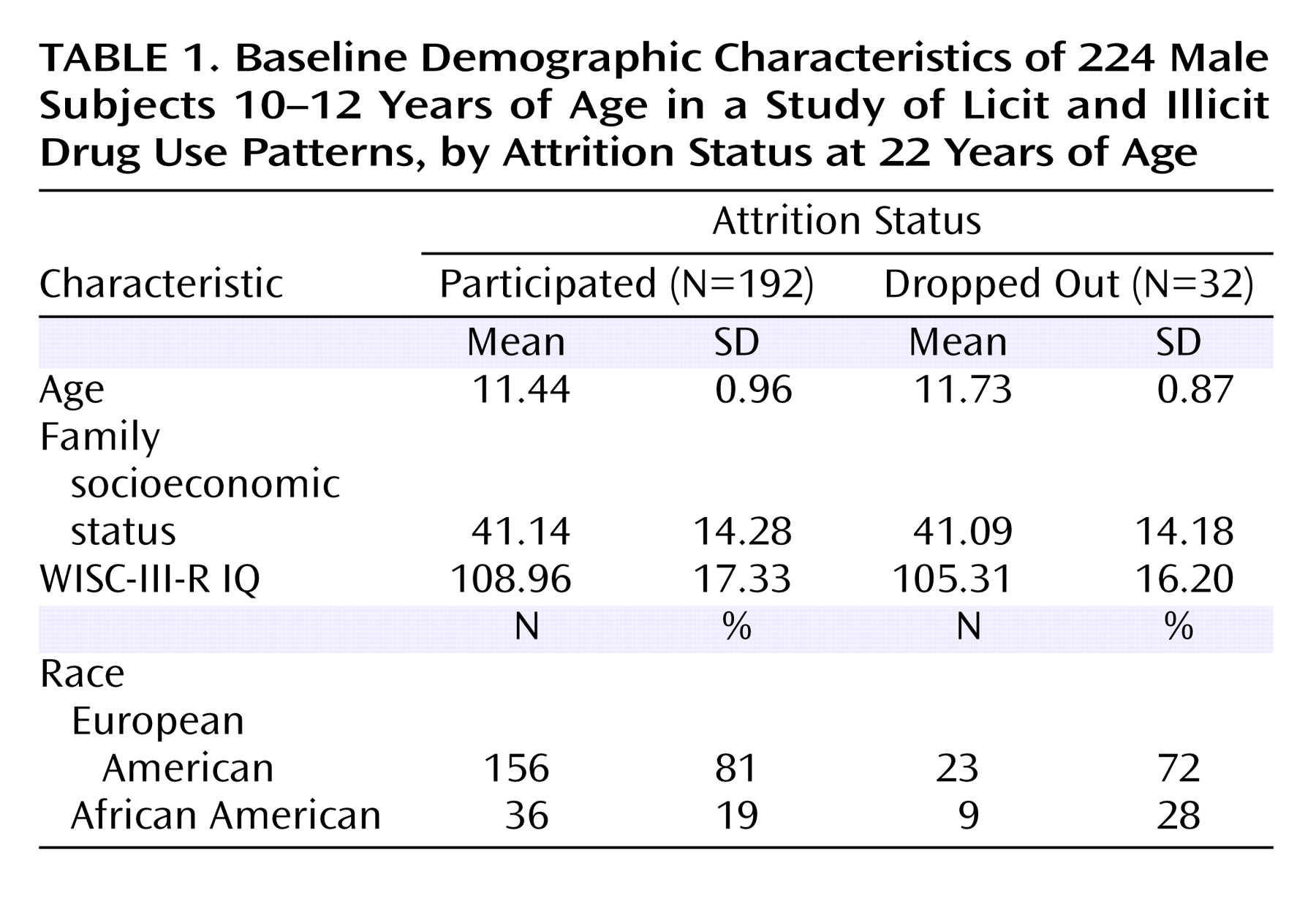
The participants were 224 males recruited at 10–12 years of age and reevaluated at ages 12–14, 16, 19, and 22. The study sample was confined to males because recruitment of girls began several years after the boys, and the sample of female participants was too small to allow longitudinal analysis. A history of chronic medical disease, psychosis, WISC-III IQ below 80, uncorrectable sensory or physical disability, and neurological injury resulting in hospitalization were exclusionary criteria. The presence of physical anomalies concomitant to prenatal alcohol exposure was a disqualifying criterion. A nurse conducted a physical examination before the research protocols were administered to ensure that participants had no current medical problems that could threaten the validity of the results.
At the time this report was prepared, 107 participants were available for the age 22 assessment. Eighty-five of the 224 boys evaluated at baseline had not yet attained age 22, and 32 subjects dropped out before age 22. Thus, the attrition rate between baseline and outcome assessment was 14%. As
Table 1 shows, the retained and attrited participants did not differ in several key personal and demographic variables.
The boys were recruited through fathers (probands) who either qualified for a substance use disorder diagnosis related to use of an illicit drug (N=95) or had no adult axis I psychiatric or substance use disorder (N=129). We used the top-down high-risk paradigm because it efficiently yields a high rate of substance use disorder outcomes in offspring. Since average liability to substance use disorder is elevated in sons of probands with a substance use disorder
(12), transition to illicit drug use is likely to occur in this sample. We recruited probands from multiple sources to reduce the potential for sample bias, which could result from use of only one source. The men were recruited through advertisements in print media, public service announcements, posters placed in public locations, and random-digit dialing. Approximately 25% of the men with substance use disorders were recruited after discharge from treatment to ensure the full spectrum of severity of substance use disorder. The pattern and severity of substance use disorder among probands with the disorder were similar to those among comparable men in the Epidemiologic Catchment Area study
(20) . The men included in the study had no history of neurological disease or injury, no physical or uncorrectable sensory disability, and no lifetime history of psychosis.
For the analyses, participants were categorized into three groups. Group I (N=99) consisted of youths who used alcohol and/or tobacco between baseline (at age 10–12) and outcome assessment at age 22 without starting marijuana use. Group II (N=97) consisted of subjects who transitioned to marijuana use after alcohol and/or tobacco use, thus exhibiting the gateway sequence. Group III (N=28) consisted of subjects who started marijuana use and then transitioned to alcohol and/or tobacco use, thus exhibiting the reverse sequence. Comparing groups I and II allowed us to determine whether specific individual or environment factors were associated with the propensity to transition from legal to illegal drugs. Comparing groups II and III allowed us to ascertain whether the gateway pattern is meaningful and has differential predictive validity.
Instruments
Substance Use
The substance use variable selected for study is critical to obtaining an accurate evaluation of the gateway hypothesis
(21) . The gateway hypothesis was initially formulated in terms of lifetime exposure—that is, at least one consumption event any time in life
(1) —but this criterion has been criticized
(22) . More recently, Kandel and Jessor
(23) stated that “increased risk of transition through the drug sequence is associated far more strongly with intensity of use than it is with use per se” (p. 369). To operationalize intensity, we established two criteria for a substance to be categorized as one the participant used: 1) the participant ranked the substance as one of his top three preferred drugs; and 2) the participant had consumed the substance within the past 30 days. Section 1A of the revised Drug Use Screening Inventory (DUSI-R)
(24) was self-administered in paper-and-pencil format when the participants were 10–12, 12–14, 16, 19, and 22 years of age to measure frequency of past-month drug use.
Substance Use Disorder
The Structured Clinical Interview for DSM-III-R (SCID)
(25) was administered when participants were 12–14, 16, 19, and 22 years of age. The results were reviewed by a committee chaired by a psychiatrist certified in addiction psychiatry, another psychiatrist or psychologist, and the clinical evaluators. The best-estimate procedure, in which the results of the diagnostic interview in conjunction with all other available medical, social, and legal history information were reviewed, was used to formulate the diagnosis of substance use disorder
(26) . Diagnoses were determined in the context of the individual’s lifetime pattern of substance use, including age at first use, age when regular use began, onset of DSM-III-R symptoms, and age at first qualification for diagnosis.
Risk Factors
Kandel and Yamaguchi
(3) maintained that drug-specific risk factors underlie the causal linkage between the stages in the gateway sequence.
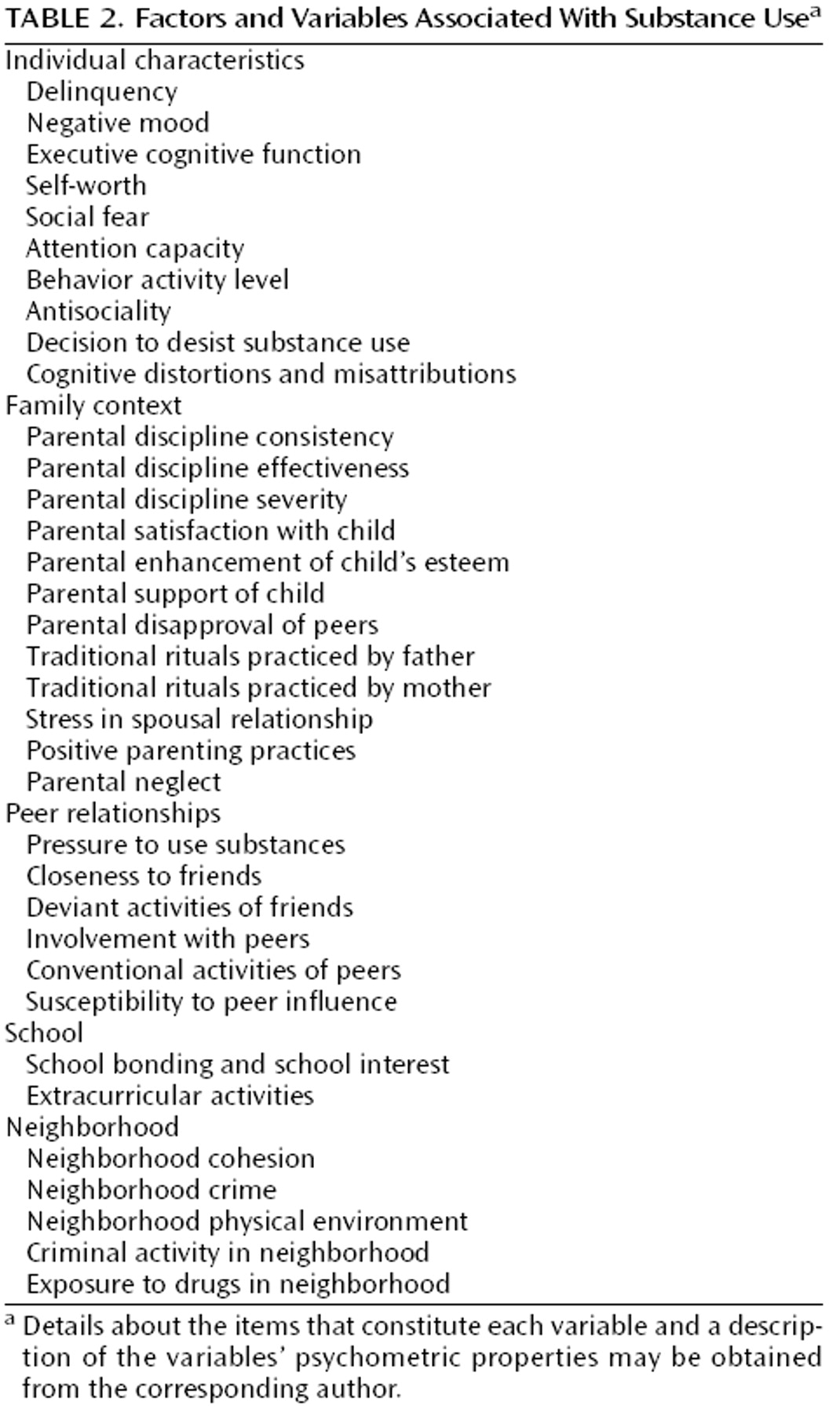
Table 2 lists the psychological, family, peer, school, and neighborhood variables used in this study to determine whether factors could be detected that are uniquely associated with each of the first two stages of the gateway sequence. Details about the items that constitute each variable and a description of the variables’ psychometric properties may be obtained from the corresponding author. As Vanyukov et al.
(27) explained, the variables were constructed from items in a large multidisciplinary data set that capture, according to their face validity, the characteristics that have been implicated in the etiology of substance use disorders. The items were then submitted to exploratory factor analysis to cull the variables that loaded on major factors (defined as accounting for at least 30% of the total variance). These items were then submitted to confirmatory factor analysis to verify unidimensionality and to item response theory analysis to derive a measurement index. After obtaining item response theory-based scores for each construct, the data were normalized to a T-scale distribution in which each variable had a mean score of 50 and standard deviation of 10.
Procedure
The same procedure was followed at each assessment. For participants under age 18, written informed consent was obtained from the parents, and participants signed assent forms before the research protocols were administered. Participants who had reached age 18 provided informed consent themselves. Privacy was assured by a Certificate of Confidentiality issued by the National Institute on Drug Abuse to the Center for Education and Drug Abuse Research at the University of Pittsburgh.
Breath alcohol and urine drug screens were conducted to ensure that the results would not be biased by the effects of recent substance use. The research protocol was administered in fixed order by experienced research associates. After assessments were completed, participants were debriefed. Financial compensation varied according to the amount of time needed to complete the research protocols, ranging from $50 to $150 between baseline and follow-up at age 22.
Statistical Analysis
One-way analyses of variance (ANOVAs) were conducted to contrast groups I and II. The significance threshold was set at 0.01 because of the large number of comparisons. Product-moment correlations were computed between each variable that distinguished the groups and substance use intensity. The z test was used to compare the magnitude of correlations to ascertain whether any of the variables were more or less strongly related in group I compared with group II.
Next, one-way ANOVA was used to compare groups II and III on the panel of 35 variables, with the significance threshold set at 0.01. (Separate between-groups ANOVAs were computed for groups I and II and groups II and III because a significant F ratio would still require post hoc pairwise comparisons.) Survival analysis was conducted to determine whether the subjects who conformed to the gateway sequence differed from those who exhibited the reverse sequence in rate of development of alcohol use disorder and marijuana use disorder. The proportion of the sample who succumbed to substance use disorder at a particular age, expressed in months of life, was determined. Survival functions were estimated by the Kaplan-Meier method. In addition, the log-rank test was used to compare the survival functions of the two groups. Cox proportional hazards analysis was used to evaluate whether the discriminating variables observed in the ANOVA were covariates along with sequence type (gateway versus reverse gateway) on the rate of succumbing to substance use disorder.
Results
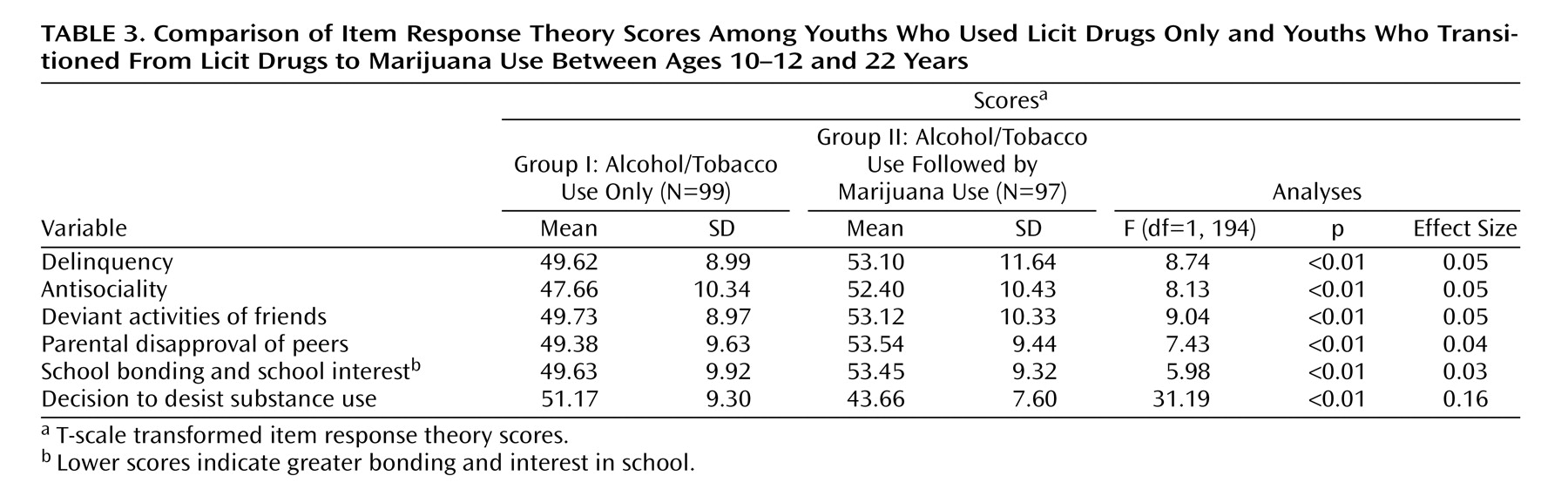
Comparison between groups I and II revealed significant differences on six variables (
Table 3 ). Youths who transitioned to marijuana use before age 22 were more behaviorally deviant, were affiliated with deviant peers, were less involved with school, had friends who were not approved by parents, and were less inclined to have made a decision to desist substance use. The effect size values were generally small, indicating that the magnitude of the difference was modest.
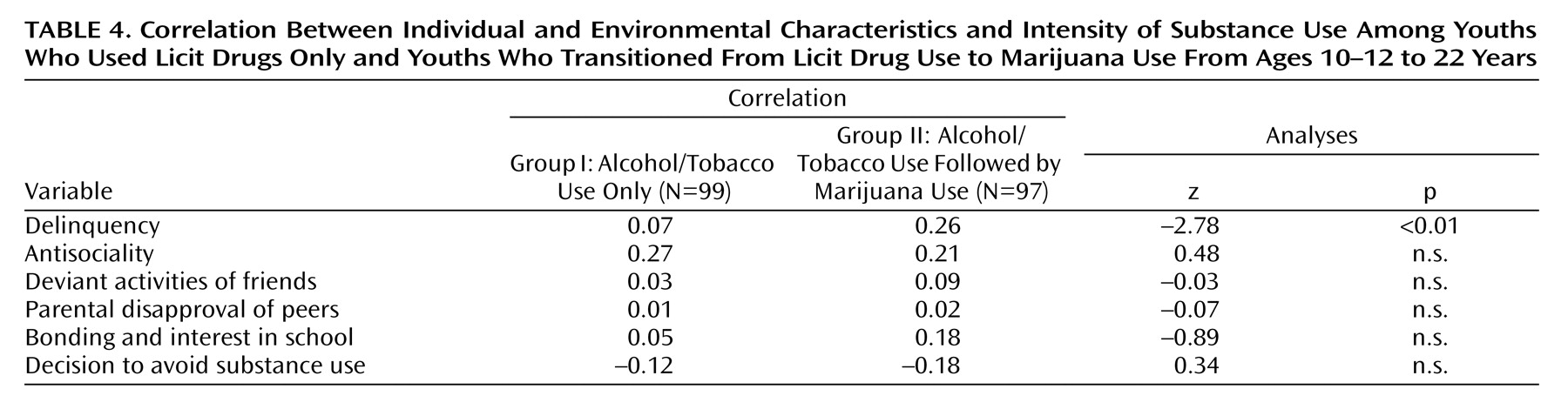
With the exception of delinquency, the magnitude of correlation between substance use intensity and the six discriminating variables was the same in groups I and II (
Table 4 ). Considered in the aggregate, these findings demonstrate that, apart from delinquency, the youths who confined consumption to licit drugs and those who transitioned to marijuana were more alike than different. Not surprisingly, boys prone to illegal behavior are inclined to use an illegal drug; however, specific risk factors associated with the transition to illicit drug use were not revealed.
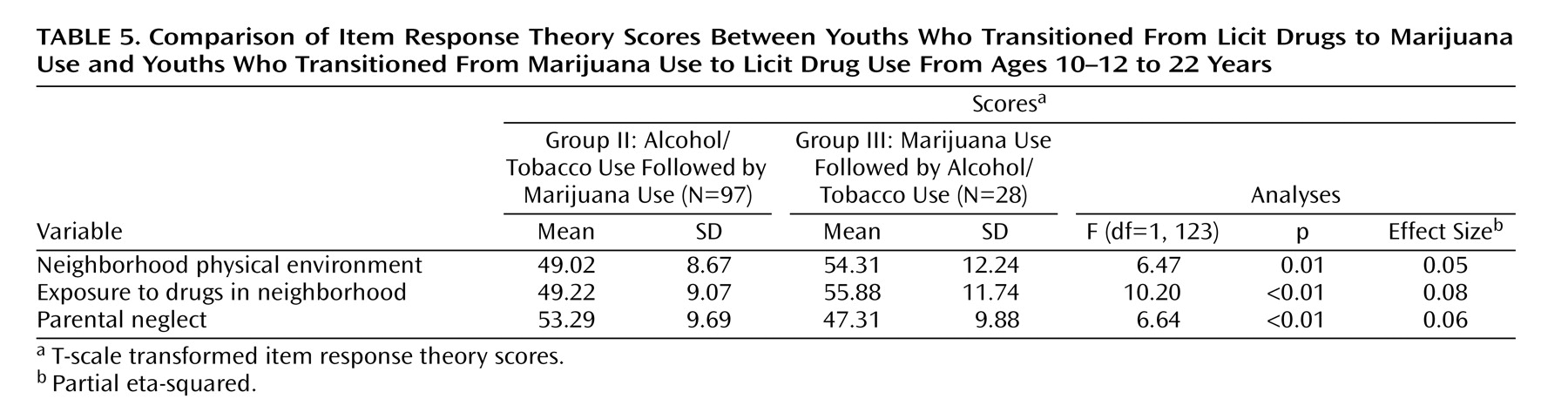
As
Table 5 shows, only three variables distinguished subjects who exhibited the gateway sequence from those who exhibited the reverse sequence. Youths in group III (reverse sequence) lived in a neighborhood with a poorer physical environment, had greater exposure to drugs in their neighborhood, and had more neglectful parents. The magnitude of these differences is small, as indicated by effect size values ranging from 0.05 to 0.08. Thus, the youths did not differ according to whether or not they conformed to the gateway sequence. When marijuana was the first drug used, it was concomitant to environmental facilitation and not individual risk factors.
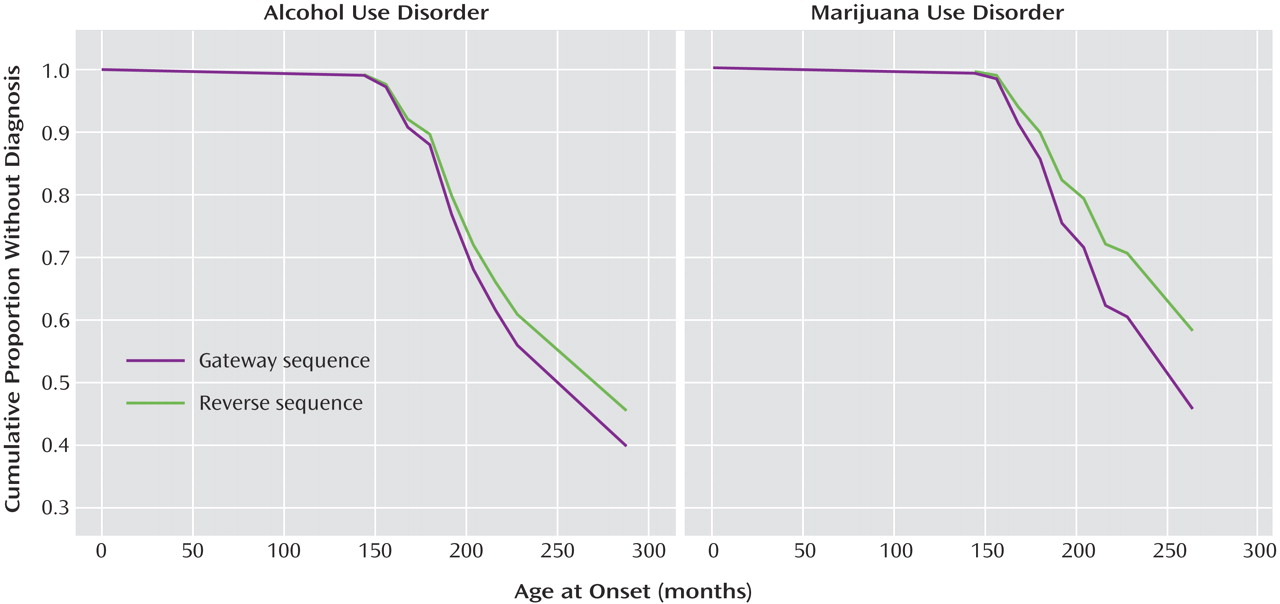
Figure 1 presents the results of the survival analysis. Subjects who exhibited the gateway (group II) and reverse (group III) sequences did not differ with respect to risk for and rate of development of alcohol use disorder (log-rank test=0.01, p=0.99) and marijuana use disorder (log-rank test=0.02, p=0.88). Alcohol use disorder was present by age 22 in 53% (N=51) and 37% (N=10), respectively, of subjects in group II and group III (χ
2 =18, p=0.67), and marijuana use disorder in 43% (N=42) and 50% (N=14), respectively (χ
2 =0.12, p=0.73). These results indicate that the particular type of substance use sequence—gateway versus reverse—was not related to the probability and rate of development of alcohol and marijuana use disorders.
In the Cox proportional hazards analysis, of the three variables listed in
Table 5 that discriminated groups II and III, only neighborhood physical environment was related to rate of development of marijuana use disorder. A one-standard-deviation decrease in quality of neighborhood increased the risk of marijuana use disorder by 89% (hazard ratio=1.89, p<0.01, 95% confidence interval=1.23–2.92). Thus, neighborhood characteristics, not gateway versus reverse gateway sequence, were associated with rate of development of marijuana use disorder.
Discussion
The gateway hypothesis holds that abusable drugs occupy distinct ranks in a hierarchy as well as definite positions in a temporal sequence. Accordingly, substance use is theorized to progress through a sequence of stages, beginning with legal, socially acceptable compounds that are low in the hierarchy, followed by use of illegal “soft” and later “hard” drugs ranked higher in the hierarchy. One of the main findings of this study is that there is a high rate of nonconformance with this temporal order. In a neighborhood where there is high drug availability, youths who have low parental supervision are likely to regularly consume marijuana before alcohol and/or tobacco. Consumption of marijuana prior to use of licit drugs thus appears to be related to contextual factors rather than to any unique characteristics of the individual. Moreover, this reverse pattern is not rare; it was observed in over 20% of our sample.
An adjustment style featured by delinquency, affiliation with deviant peers, and low connectedness to school is associated with the transition from licit to illicit drug use. Kandel and Yamaguchi
(28) similarly concluded that deviancy and affiliation with nonnormative peers are associated with marijuana use. In effect, the greater the deviancy, the more likely an individual is to use an illegal drug. These findings underscore the need to prevent conduct problems in early childhood to diminish the risk of later illicit drug use.
The main task in prevention of substance use and substance use disorder thus involves promoting normative socialization such that during adolescence, when exposure to abusable substances sharply increases, the values and attitudes required for avoidance of illegal behavior, including marijuana use, will have been established. Toward this goal, fostering the caregiver’s emotional bonding to the child establishes the motivation for long-term investment in child supervision. Periodic home visits by nurses to counsel high-risk pregnant women have been shown to have a positive long-term impact on social adjustment in the women’s children
(29) . It is also noteworthy that a difficult temperament amplifies the risk of conduct disorder
(30) . Because parental reaction to children with difficult temperaments commonly features avoidance or harsh punishment, consolidating positive parent-child interactions by potentiating parenting skills facilitates the child’s normative development. Children with difficult temperaments disengage from the parental influence earlier in life than “normal” children
(31) . Given our finding in this study that low parental involvement predisposed to marijuana use before licit drug use, it would appear to be important to implement interventions directed at improving the quality of parent-child interactions by taking into account the child’s temperament. Attention deficit hyperactivity disorder (ADHD) also frequently presages conduct disorder. Evidence suggests that pharmacotherapy of childhood ADHD reduces the risk of substance abuse
(32) . Thus, rather than focus on putative drug-specific risk factors, the common liability model emphasizes an ontogenetic framework wherein prevention of early conduct problems reduces the likelihood of illegal behavior, including marijuana use.
The results of this study reinforce the need for conceptual clarity in research on the etiology of substance use and substance use disorder. Our key findings were that 1) there are no unique factors distinguishing the gateway sequence and the reverse sequence—that is, the sequence is opportunistic; 2) the gateway sequence and the reverse sequence have the same prognostic accuracy; and 3) a sizable proportion of substance users begin regular consumption with an illicit drug. These results, considered in the aggregate, indicate that the gateway sequence is not an invariant pathway and, when manifest, is not related to specific risk factors and does not have prognostic utility. The results of this study as well as other studies
(4 –
8) demonstrate that abusable drugs occupy neither a specific place in a hierarchy nor a discrete position in a temporal sequence. These latter presumptions of the gateway hypothesis constitute what Whitehead
(33) referred to as the “fallacy of misplaced connectedness,” namely, asserting “assumptions about categories that do not correspond with the empirical world.”
In contrast to the gateway hypothesis, the alternative common liability model has heuristic potential for quantifying a child’s risk for substance use disorder. Vanyukov and colleagues
(19,
27) have described the rationale and method for quantifying the common liability for substance use disorder. They also describe a provisional scale that quantifies liability severity and has discriminative and predictive validity. With further validation of this scale, the empirical foundation will be established to tailor the intensiveness of prevention of substance use disorder to severity of the child’s risk.
Several limitations of this study should be noted. First, the sample was confined to males; inasmuch as there are gender differences in the pattern of initiation and progression of substance use
(28), the results may not generalize to females. Second, only the first two stages of the gateway sequence were evaluated, and all licit drugs (beer, wine, liquor, tobacco) were combined into one stage to provide the best opportunity for confirmation of the gateway hypothesis. In early formulations of the gateway hypothesis, beer and wine were theorized to precede tobacco and hard liquor; however, the sequence was subsequently collapsed to combine tobacco and alcohol into one stage. Finally, it was not possible to rule out entirely the absence of unique associations between individual and environmental characteristics and use of a specific type of drug. Although 35 variables were examined, it is conceivable that other factors have a specific association.
The results of this study suggest that general behavioral deviancy and not specific risk factors accounts for illicit drug use. When illicit drug use occurs first, it is very likely due to the opportunity afforded by the neighborhood environment in context of low parental supervision. The probability and rate of development of a diagnosis of marijuana use disorder and alcohol use disorder were the same whether or not there was conformance with the gateway sequence. Evidence supporting “causal linkages between stages,” as specified by the gateway hypothesis (
3, p. 64), was not obtained. Nor were specific risk factors identified that were related to consumption of each drug. Our results indicate that efforts to prevent marijuana use should utilize strategies directed at averting the development of the characteristics prodromal to the manifestation of behavior problems.