Worldwide, mental disorders are common, persistent, costly, and contribute substantially to the total burden from disease
(1,
2) . In spite of this, studies of developed Western societies have consistently documented that only a minority of people with psychiatric disorders receive some form of treatment
(3 –
6) . Although these estimates are disturbingly low, the rates of receiving treatment that conform with evidence-based recommendations
(7 –
18) are even lower
(19 –
23) .
Few studies from developing countries are available regarding the use of services among persons with a mental disorder
(24 –
27) . The available data show that an even smaller percentage of persons in need may get help for their mental disorder. Mexico is no exception, with preliminary and more limited research
(25 –
28) suggesting that the rates of mental health service use are low and that barriers, both psychological as well as limits in availability and access, abound. Also lacking have been up-to-date and rigorous data on the quality of treatments being received in Mexico.
Recent developments offer new hope that the problems of underuse and inadequate use of mental health services in Mexico can be better understood. In 2001–2002, the National Institute of Psychiatry in Mexico conducted the Mexico National Comorbidity Survey
(27), which is part of the World Health Organization’s (WHO) World Mental Health Surveys Initiative
(29,
30), devoted to evaluating the prevalence of psychiatric disorders in countries with varying degrees of development, determining the extent of unmet needs for mental health services, and directing public policy in this area.
Method
Sample
A general description of the Mexico National Comorbidity Survey has been presented elsewhere
(27) . The survey is based on a stratified, multistage area probability sample of persons ages 18 to 65 years in the noninstitutionalized population living in urban areas (population 2,500+) of Mexico. About 75% of the Mexican population lives in urban areas and meets this definition. Data collection took place in two phases from September 2001 through May 2002. The response rate was 76.6% (for a total of 5,826 interviews, well above the original targeted sample size of 5,000) and within the scope of other surveys from the World Mental Health Initiatives (response rate range=50.6%–87.7%)
(30) . All respondents were administered the part I interview, and a selected subsample of 2,362 received a supplemental number of questions on risk factors and supplemental mental disorders. The sample was administered part II of the interview and consisted of all respondents who screened positive for any disorder that was found to be positive on part I of the interview, plus a probability subsample of other part I respondents. All interviews were conducted at the respondents’ homes after a careful description of the study goals was given and informed consent was obtained. No financial incentive was given for the respondents’ participation. All recruitment and consent procedures were approved by the ethics committee of the National Institute of Psychiatry.
Measures
The instrument used was the computer-assisted personal interview version of the WHO World Mental Health Survey Initiative version of the Composite International Diagnostic Interview (CIDI)
(31,
32) . This structured diagnostic interview was administered by an interviewer in face-to-face interviews, which yielded DSM-IV diagnoses.
The Spanish version of the World Mental Health CIDI used in Mexico was developed by using the standard WHO approach (i.e., translating, back-translating, and harmonization of modules), the Spanish versions of ICD-10 and DSM-IV, and previous Spanish versions of the Diagnostic Interview Schedule and CIDI. These instruments have shown good performance in validity studies in Mexico
(33,
34) and other Spanish-speaking countries
(35) . The fieldwork was conducted by Berumen and Associates, an established survey research firm in Mexico, and employed a group of interviewers who had received training in using the computer-assisted personal interview version of the CIDI.
Disorders
For this article, we reported on the 12-month rate of service use for the following categories of psychiatric disorders—affective disorders: major depressive episode, minor depressive episode, bipolar I and II disorder, and dysthymia with hierarchy; anxiety disorders: panic disorder, agoraphobia without panic disorder, social phobia, specific phobia, separation anxiety disorder, generalized anxiety disorder, and posttraumatic stress disorder; substance use disorders: alcohol and drug abuse and dependence.
Treatment Sectors
Information about the receipt of 12-month treatment for emotional, alcohol, or drug problems, the type and context of professionals visited, as well as the use of self-help or support groups and hotlines was obtained. The number of treatment visits made in the prior 12 months was also assessed. Respondents could select as many professionals and treatment options as they used in the previous 12 months.
Mental health care in the 12 months before the survey was performed was divided into the following five sectors: 1) psychiatrists; 2) other mental health specialists, consisting of psychologists, counselors, psychotherapists, mental health nurses, and social workers in a mental health specialty setting; and 3) general medical practitioners, consisting of family physicians, general practitioners, and other medical doctors, such as cardiologists, or gynecologists (for women) and urologists (for men), nurses, occupational therapists, or other health care professionals; 4) human services, including outpatient treatment with a religious or spiritual advisor or a social worker or counselor in any setting other than a specialty mental health setting, or a religious or spiritual advisor, such as a minister, priest, or rabbi; 5) complementary-alternative medicinal Internet use, including self-help groups, any other healer, such as an herbalist, a chiropractor, or a spiritualist, and other alternative therapy.
We grouped the psychiatrists and mental health specialty providers under “any mental health care providers”; the psychiatrists, mental health specialists, and general medical care providers under “any health care services”; and the human services and complementary-alternative medicine professionals under “any non-health care service.”
Minimally Adequate Mental Health Care
With available evidence-based treatment guidelines for primary care
(7) and specialty mental health providers
(8 –
12), we defined minimally adequate treatment during the prior 12 months as receiving 1) minimally adequate psychotherapy, consisting of four or more outpatient visits to any provider
(36,
37) ; 2) minimally adequate pharmacotherapy, consisting of two or more outpatient visits to any provider and treatment with any medication for any length of time
(38), and 3) reporting still being “in treatment” at the time of the interview. Although this definition is broader than the one that we used previously
(23), it allowed us to obtain conservative estimates of minimally adequate treatment across sectors. In sensitivity analyses, a more stringent definition of minimally adequate treatment was also used in which we required 1) eight or more visits to any service sector for psychotherapy or 2) four or more visits to any service sector and 30 or more days taking any medication for pharmacotherapy.
Analyses
The data for the part II respondents were weighted to adjust for differential probabilities of selection and nonresponse. The sample receiving part II of the survey was additionally weighted to adjust for the differential probability of selection. Poststratification to the urban Mexican population according to the 2000 census in the target age and sex range was also performed. Estimates of standard errors for proportions were obtained by the Taylor series linearization method with SUDAAN software
(39) . Logistic regression analysis
(40) was performed to study demographic correlates. Two parallel analyses were performed, one for receiving any treatment among those with disorders and a second one for receiving minimally adequate treatment among those with disorders who received any treatment. Estimates of standard errors of odds ratios and corresponding standard errors from logistic regression coefficients were also obtained with SUDAAN, and 95% confidence intervals were adjusted for design effects. Statistical significance was evaluated with two-sided design-based tests with the 0.05 level of significance. The design effects varied from 3.25 for sex to 1.12 for any treatment among the entire sample.
Results
Among the 2,362 respondents to the Mexico National Mental Health Survey, the 12-month frequencies of any anxiety, affective, substance, or any of these three types of disorders were 6.8%, 4.8%, 2.5%
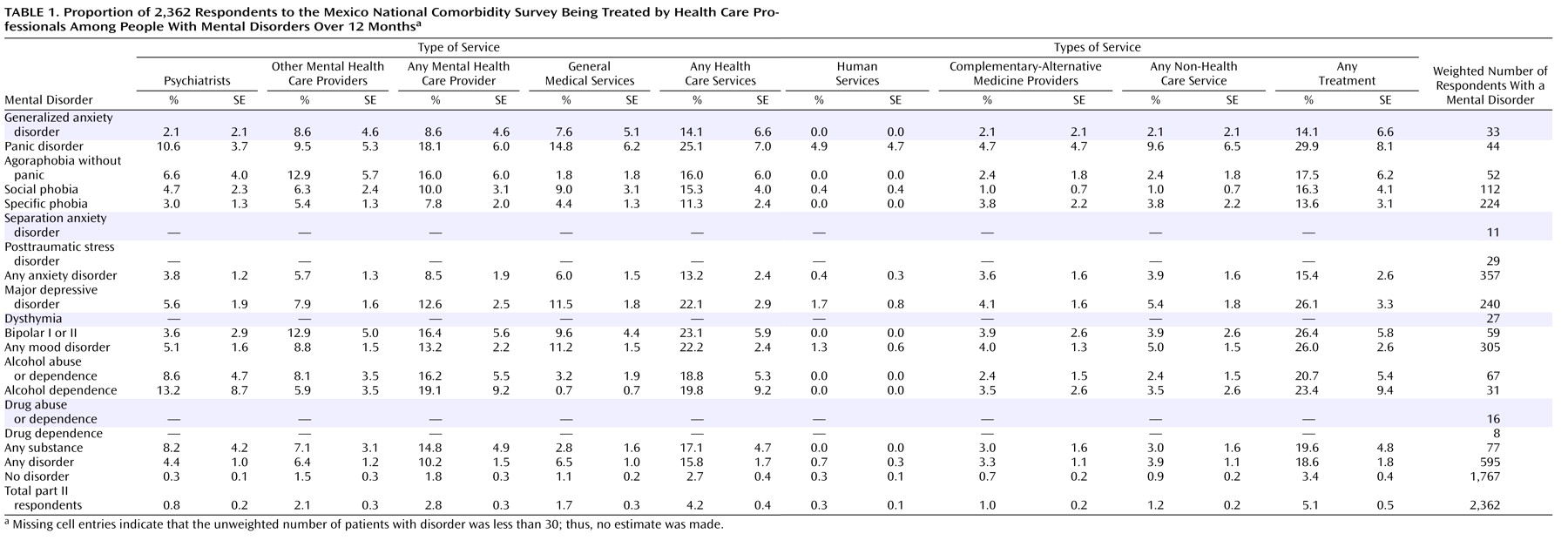
(30), and 11.6%, respectively. As shown in
Table 1, 5.1% of the total part II respondents reported using any service for the treatment of their emotional problems in the last 12 months. As expected, the proportion of any service use was lower among the respondents without any 12-month mental disorders (3.4%) and higher among respondents with any 12-month disorder (18.6%). Individuals with mood and substance disorders had the highest rate of service use. The sectors in which care was received differed among the three types of disorders; respondents with mood disorders made more use of general medical doctors, whereas respondents with substance disorders tended to use more mental health specialists. Among respondents with anxiety disorders, the mental health specialty and general medical sectors were most frequently used. The individual disorder with the highest use of any service was panic disorder, followed by bipolar I and II disorders. Unexpectedly, alcohol dependency had the highest rate of the use of psychiatrists. The combined use of both the health and non-health care sectors was relatively infrequent: among users of any service in the prior 12 months, 92 (76%) used only the health care sector, 21 (17%) used only the non-health care sector, and 8 (7%) used both.
Among the total sample of respondents, the mean number of visits for any treatment in the previous year was 4.2, and there were no differences in the mean number of visits among respondents with or without psychiatric disorders. The sector with the largest mean number of visits was the complementary-alternative medicine sector (44.7 visits), followed by other mental health care (5.9 visits), the general medical sector (3.5 visits), and the psychiatrist sector (2.8 visits). Patients with anxiety disorders had a slightly higher mean number of visits (5.0). (Results are not shown but are available upon request from the first author.)
Table 2 presents the adequacy of 12-month treatments. Overall, 57.0% of those receiving any services obtained treatment that could be considered minimally adequate. There were generally only minor differences across anxiety and mood disorders. Although we observed low rates of minimally adequate treatment among those with substance disorders, a small number of respondents in this category precluded us from making stable estimates. In the total sample, the psychiatrist sector showed the highest levels of treatment adequacy (67.7%).
In sensitivity analyses with our more stringent definition, the proportion of respondents obtaining minimally adequate treatment among those with disorders receiving any services decreased to 19.2%; this proportion was 21.2% among respondents with anxiety disorders and 23.5% among those with mood disorders. (Results are not shown but are available upon request from the first author.)
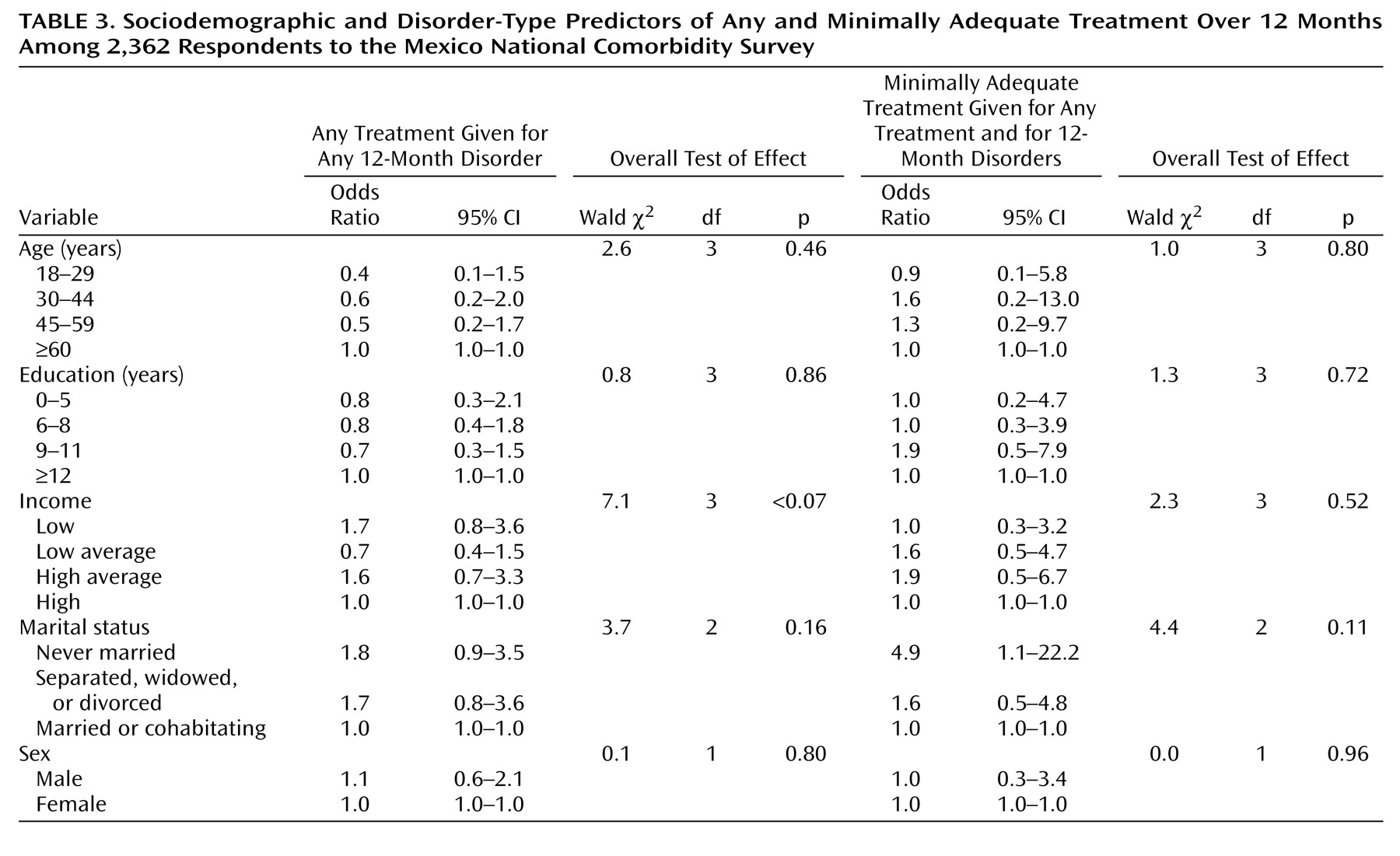
Table 3 presents the sociodemographic predictors of any service use among respondents with 12-month disorders and minimally adequate treatment among respondents with any service use and a 12-month disorder identified in multiple logistic regression models with control for disorder profiles. Few sociodemographic variables considered here were significantly related to any treatment among people with a psychiatric disorder. In addition, we did not find significant correlates of adequate treatment among people with a psychiatric disorder that had any treatment. There was a tendency for people who never married to have higher probabilities of beginning treatment and, once in treatment, receiving minimally adequate treatment.
Discussion
The following three sets of limitations should be kept in mind when interpreting the results of this study. First, we may have underestimated the prevalence of mental disorders, both because the disorders assessed were only a subset of those in DSM-IV as well as because of potential nonresponse bias. In addition, we may have missed many of the most severely impaired individuals because the homeless and institutionalized were excluded. This set of limitations is likely to have caused us to underestimate the magnitude of unmet needs for any mental health treatment and minimally adequate treatment. Although previous versions of the CIDI have been validated in Mexico and other Spanish-speaking countries, the reliability and validity of the version used in this survey have not been established in Mexico. Finally, recent studies of the exclusion rules used within the alcohol and drug disorder modules suggested that our current prevalence figures may be underestimations
(41) . Indeed, the 12-month prevalence estimates of anxiety disorders, affective disorders, and substance use disorders reported for the Mexican survey appear low compared to estimates from other countries within the WHO World Mental Health Survey Consortium, especially from the region of the Americas
(30), but previous cross-national comparisons on more limited surveys have also suggested that Mexico has a low prevalence of psychiatric disorders
(28) .
Second, although some investigators
(13 –
18) have shown that treatments that conform to recommendations in evidence-based treatment guidelines improve clinical outcomes, we are not aware of any studies that have validated our exact definition of minimally adequate treatment. The nonrandom use of treatments in our study population made it impossible to investigate whether receiving our definition of minimally adequate care was associated with improved health outcomes.
Third, we only examined the relationships between a small number of patient factors and the receipt, type, and adequacy of mental health treatments; we did not have the ability to investigate other potentially important variables, such as the characteristics of providers. Finally, we cannot conclude that factors associated with receiving any treatment or minimally adequate treatment are related causally because of the study’s cross-sectional nature.
Within the context of these limitations, these results shed light on an enormous public health problem facing Mexico. We found large unmet needs among those with psychiatric disorders and extensive underutilization of mental health services. Fewer than one in five respondents with any psychiatric disorder in the last 12 months had used any service. Although the rates of service use by those with some disorders (e.g., mood disorders) are somewhat higher, in absolute terms, treatment rates remain quite low. These data confirm previous research in Mexico showing that the majority of people with a recent psychiatric disorder have not received recent treatment
(25,
42) . A recent report contrasting 14 participants in the World Mental Health Survey Initiative
(30) showed that Mexico scored the lowest in the rate of service use in the Americas but higher than other developing countries, such as Lebanon, Nigeria, and two major cities of China. In the United States
(43), 40.9% of subjects with a mental disorder received some treatment over 12 months, more than two times higher than our results for Mexico. Our data do raise the concern that scarce resources for mental health care may be being misallocated. Although respondents with a DSM-IV disorder were 5.5 times more likely to receive treatment than respondents without a disorder, the latter comprised 58% of the population using services. However, some services may be used by respondents with lifetime histories of disorders, possibly for secondary prevention; other respondents without apparent disorders may also be using services appropriately for primary prevention, subthreshold symptoms that do not qualify as full-blown disorders, or for disorders not assessed by our survey
(30) . Given these possibilities, it may be premature to make recommendations for the health care system regarding delivering treatment to persons with no apparent disorders. Furthermore, it is not clear if and how reducing treatment among subthreshold cases would lead to increased use among diagnosed cases. Further research on how to optimally allocate mental health resources is needed to create rational future policies in this area.
Although results concerning the receipt of any treatment are troubling, the rates of receiving minimally adequate treatment for mental disorders were even lower because only 56% of those with a psychiatric disorder met our broad criteria. More stringent criteria showed that this proportion can be as low as 19.2%. There are many potential reasons for this failure to receive minimally adequate care. Individuals with mental disorders, especially those with the most serious and impairing forms, may lack the ability and resources to consistently access mental health treatments
(44) . Patients may also find prescribed treatments intolerable
(45) . Providers may lack the training to recognize and properly diagnose mental disorders or lack the knowledge concerning optimal treatment regimens
(46 –
48) . It is difficult to contrast our results regarding the adequacy of treatment with previous research that used even more stringent criteria, but limited evidence suggests that the low mean number of visits is a key factor. For example, in our sample, the median number of visits among all respondents was 4.2, but it was 14.8 in similar research in the United States
(43) . This U.S. research also discovered a large difference in the mean number of visits between respondents with a disorder (17.0 visits) and without a disorder (11.6), but in Mexico, both types of respondents had exactly the same mean number of visits (4.2).
These results may not be surprising, given the dearth of mental health resources in Mexico. For a population of about 100 million inhabitants in 2000, the WHO estimated only 6,000 psychiatric beds nationally; 2,500 psychiatrists graduated as of 2000, of which only 890 are certified, and the majority are concentrated in Mexico City; 1,500 psychiatric nurses and fewer than 400 psychiatric social workers have graduated. Although almost 46,000 psychologists had graduated nationally as of 1990, only 73% were working as such. According to the WHO Atlas on Mental Health Resources in the World
(49), the number of psychiatrists per capita in Mexico ranks in the second lowest tier among the nations of the world (with a median ranging between 1.01 and 5.00 per 100,000 individuals). Mexico’s rating is only just above the rating for countries in the African region and Southeast Asia and considerably lower than the rates observed in Europe (median range=9.0), Canada, and the United States (median per 100,000 inhabitants was greater than 10).
No sociodemographic characteristic predicted the use of mental health services among subjects with psychiatric disorders nor the adequacy of services. The lack of differences in service use among men and women was unexpected because earlier research suggested that women have a greater ability to translate nonspecific feelings of distress into conscious recognition that they have emotional problems and are therefore more likely to seek and accept treatment
(50 –
51) . Never-married persons may tend to use more services and receive more adequate treatment in Mexico because difficulties forming or maintaining relationships may lead those who are not married to seek out mental health treatment; alternatively, dysfunction from psychiatric disorders may lead to both difficulties in relationships and the use of treatment
(52,
53) . Although Mexico is a country with a low socioeconomic status, and the lack of financial resources may help explain the low rate of service use, we did not find an association between education and income upon receiving any treatment or minimally adequate treatment in our survey.
This study provides evidence of the enormous challenges faced by those with mental illness and those who deliver or seek to improve mental health care in Mexico. In spite of the existence of effective treatments, few with mental disorders received any form of care. Even those that ultimately access treatment do so only after experiencing considerable delays. Compounding these challenges are the enormous tasks of improving the quality of providers’ treatments and improving patients’ adherence to treatments, tasks made more difficult by the severe limits on current health care resources. Future studies will need to focus on increasing our understanding of modifiable reasons for these enormous unmet needs
(54) . Such information will be crucial in designing and targeting public policy and cost-effective interventions to improve treatment access, treatment quality, and, ultimately, the health outcomes of those with mental illness in Mexico.