However, the majority of these studies have been retrospective. Retrospective studies and reviews
(24–
27,
34,
37,
38) that have suggested an association between longer duration of untreated initial psychosis and poor outcome in schizophrenia have had significant methodological limitations, including unevenly characterized samples and not accounting for the effects of factors known to be prognostic of schizophrenia
(44). On the other hand, the number of prospective studies has been small. The outcome measures used in the prospective studies
(10,
36,
39,
40) have been based on symptoms, i.e., time to remission, level of remission, and relapse. Since the predictor measure (duration of untreated initial psychosis) and outcome measures (time to remission, level of remission, and relapse) are both symptom related, the chances of finding an association will be expectedly high. While symptom remission and relapse rates are important measures of outcome in schizophrenia, to solely use these measures in studies investigating the effects of untreated initial psychosis duration confounds the results and limits outcome measurement to a single dimension of the illness.
Outcome in schizophrenia is a complex phenomenon
(45). Over the years, investigators have become increasingly sophisticated in the assessment of outcome—from categorizing outcome into “improved” versus “not improved” or “good” versus “poor” to the use of multiple domains of outcome (such as rehospitalization rates, symptom relapse/remission, quality of life measures, and cognitive functioning). During the past 20 years, the concept of quality of life (including psychosocial functioning) has become an important outcome measure not only in clinical studies but also in patient care and health economic analyses
(46–
48). Although there is still no clear consensus about what constitutes quality of life or how to best measure it, investigators often use information from multiple sources (including the patient’s perceptions, reports from reliable informants, and the clinician’s own assessment) to gauge both the subjective and objective aspects of quality of life
(49,
50).
The aim of this study was to investigate the effects of untreated initial psychosis on outcome in schizophrenia. The potential confounding effects from other known prognosticators of schizophrenia and their interactions with untreated initial psychosis duration are explored. This permits better estimation of the unique contribution of untreated initial psychosis duration to outcome in schizophrenia. The outcome measures in this study will include both symptom severity and symptom remission as well as quality of life, assessed by examining both subjective and objective indicators.
Method
Subjects
The subjects were drawn from the ongoing Iowa Prospective Longitudinal Study of Recent-Onset Psychoses
(51). After complete description of the study to the subjects, written informed consent was obtained. The study design and method have been previously described. In brief, the study consists of subjects with schizophrenia or schizophrenia spectrum disorders who have had their first hospitalization during the previous 5 years. Approximately half of these are first-episode, neuroleptic-naive subjects. At the time of intake into the study, the subjects undergo an extensive evaluation, which includes phenomenological assessment (symptoms, family history, and obstetric complications), neurological examination, a neuropsychological battery, and a magnetic resonance imaging scan of the brain.
Two structured interview instruments, the Comprehensive Assessment of Symptoms and History
(52) and the Psychiatric Status You Currently Have—Baseline Version
(53), were used as part of the phenomenological assessment. The Scale for the Assessment of Negative Symptoms (SANS)
(54) and the Scale for the Assessment of Positive Symptoms (SAPS)
(55) form part of the two structured interview instruments. The Psychiatric Status You Currently Have interview has items that assess both subjective as well as objective measures of quality of life. Information from all available sources, including the subject, family members, and previous medical records, were incorporated to arrive at a consensus rating for each item in these structured instruments.
This report focuses on 74 first-episode, neuroleptic-naive subjects with DSM-IV schizophrenia (46 men and 28 women) who had been followed for at least 6 months. The mean age at intake into the study was 24.7 years (SD=5.8).
Ascertainment of Untreated Initial Psychosis Duration
Duration of untreated initial psychosis was defined in two ways: 1) the time period from the onset of the first symptom to the initiation of neuroleptic treatment and 2) the time period from the onset of a full positive syndrome to the initiation of neuroleptic treatment. The “first symptom” could include both positive symptoms (delusions, hallucinations, bizarre [disorganized] behaviors, formal thought disorder, and catatonic motor behavior) as well as prodromal symptoms that were mild variants of either positive or negative symptoms (e.g., social isolation, impairment in role functioning, peculiar behavior, impaired hygiene and grooming, blunted affect, digressive or vague speech, odd or magical thinking, and unusual perceptual experiences such as illusions). On the other hand, “full syndrome” refers to the presence of any one of the five positive symptoms at a severity level of moderate or worse.
Age at Onset and Premorbid Functioning
Ascertaining the age at onset in schizophrenia can be difficult, particularly for cases where onset is insidious or when the first indications of illness are nonspecific (e.g., drop in grades, loss of job). Therefore, in the Comprehensive Assessment of Symptoms and History, age at onset refers to the age at which the subject “first had problems.”
Premorbid functioning was assessed using the Modified Premorbid Adjustment Scale
(56). This scale yields two measures of premorbid functioning according to age group: childhood (ages 6–12, score range=0–10) and adolescence and young adulthood (ages 13–21, score range=0–13). The total Premorbid Adjustment Scale score is obtained by summing up the two subscores. Higher scores indicate poorer premorbid functioning.
The measures of untreated initial psychosis duration, age at onset, and Premorbid Adjustment Scale subscores had interrater and test-retest reliabilities (intraclass r values) that exceeded 0.87 and 0.55, respectively
(52,
56).
Assessment at 6-Month Follow-Up
As part of the longitudinal study, each subject was reevaluated 6 months later by the rater who had made the intake assessment. Follow-up versions of the Comprehensive Assessment of Symptoms and History and the Psychiatric Status You Currently Have were administered at follow-up to document the subjects’ quality of life and severity of symptoms during the previous 6 months.
Several quality of life domains, determined through both subjective and objective indicators, were assessed at the 6-month follow-up: degree of impairment in interpersonal relationships with family members, degree of impairment in interpersonal relationships with friends, degree of impairment in enjoyment of recreational activities, overall satisfaction, occupational functioning (percent of time during the preceding 6 months the individual was employed and degree of occupational impairment during the month preceding the follow-up evaluation), income source (percent of time during the preceding 6 months the subject was financially dependent on social service agencies), performance of household duties (percent of time during the preceding 6 months the subject was unable to perform household duties and the degree of impairment during the month preceding the follow-up evaluation), overall level of psychosocial adjustment, and the Global Assessment Scale (GAS) score
(57). For items in which degree of impairment was assessed, ratings were made on a 5-point scale, with 5 representing the most impairment.
The severity of symptoms during the week before the 6-month follow-up evaluation were assessed by using the SANS and SAPS. Three dimensions were used to summarize symptom severity, based on previous factor analytic studies
(58–
61). The negative symptom dimension was defined as the sum of the global ratings of alogia, anhedonia, avolition, and affective flattening (range=0–20). The psychotic symptom dimension was defined as the sum of the global ratings of delusions and hallucinations (range=0–10). The disorganized symptom dimension was the sum of the global ratings of bizarre (disorganized) behavior, positive thought disorder, and inappropriate affect (range=0–15). Higher scores represent greater symptom severity.
Positive symptom remission was defined as a rating of 2 or lower (not worse than mild severity) on all global scores within the psychotic and disorganized symptom dimensions persisting for at least 8 consecutive weeks. Positive symptom remission was dated from the time remission criteria were first met.
Statistical Analyses
As the two measures of untreated initial psychosis duration were not normally distributed, nonparametric statistical tests were used. Spearman’s correlation analyses were used to examine the relationships between the measures of untreated initial psychosis duration and age at onset, premorbid functioning, quality of life, and symptom severity at 6 months after the first hospitalization. Because multiple comparisons were made on outcome measures at 6 months, a Bonferroni correction (critical p=0.004) was applied to reduce the risk of type I error in the correlational and the extreme groups analyses. The Cox proportional hazards model (log rank test) was used to examine the relationship between untreated initial psychosis duration and remission of positive symptoms. All tests of significance were two-tailed.
Results
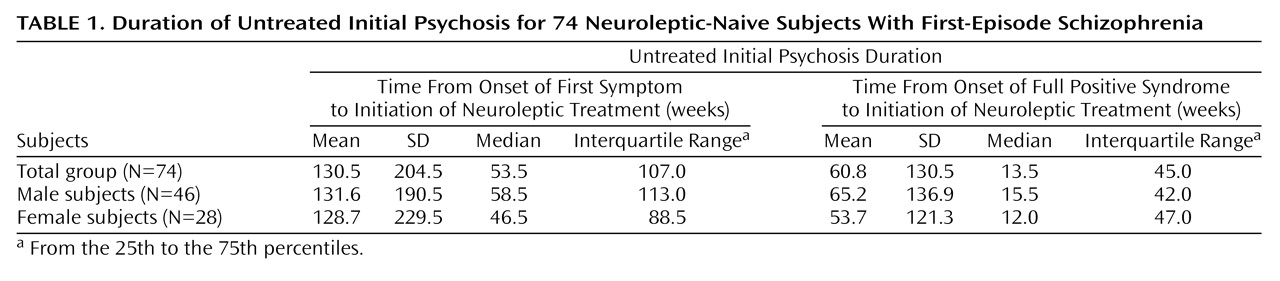
The duration of untreated initial psychosis for the 74 subjects, as well as a breakdown by gender, are summarized in
Table 1. Although male subjects sought treatment later than female subjects, the gender differences in untreated initial psychosis duration were not statistically significant for the time period from onset of either the first symptom or the full psychotic syndrome to the initiation of neuroleptic treatment (Wilcoxon rank sum z=–0.36 and –0.54, respectively, p>0.59 for both). An earlier age at onset was moderately correlated with longer time since onset of first symptom (
Table 2). Otherwise, no statistically significant associations were found between duration of untreated initial psychosis and age at onset or premorbid functioning.
All but one subject began neuroleptic treatment during the first psychiatric hospitalization. Since this is a naturalistic study, medication treatment was not controlled. The subjects received neuroleptics for the greater part of the 6 months after index assessment (mean duration of neuroleptic treatment=22.4 weeks, SD=6.6). At the 6-month follow-up, 15 subjects (20.3%) were not receiving neuroleptics, while 42 (56.8%) were taking typical neuroleptics (mean dose=502.5 mg/day of chlorpromazine equivalents, SD=476.8), and 17 (23.0%) were taking atypical neuroleptics (either risperidone [N=10; mean dose=4.8 mg/day, SD=2.0] or olanzapine [N=6; mean dose=8.8 mg/day, SD=3.8]; one patient was receiving clozapine, 300 mg/day). Multivariate correlation between duration of neuroleptic treatment and the 11 quality of life measures was examined after rank transformation of these variables. The overall R2 of 0.24 did not reach statistical significance (F=1.78, df=11, 62, p<0.08).
Quality of Life
In general, the quality of life was poor during the 6 months after discharge (
Table 2). The quality of relationship with family members was between very good and good, but the quality of relationships with friends, level of involvement and enjoyment in recreational activities, and overall satisfaction in life were all between fair and poor. The subjects had severe impairment in occupational functioning and were employed for only about one-third of the 6-month period. While the mean ratings suggested mild to moderate impairment, the subjects were able to engage in performing household duties for most of the 6 months. By the 6-month follow-up evaluation, 56.7% (N=42) of the subjects were financially dependent on social service agencies and had been receiving payments from social service agencies for nearly one-third of the 6-month period. The subjects’ overall psychosocial functioning was moderately to markedly impaired. The mean GAS score approached a level signifying major impairment.
Since there was a significant inverse relationship between age at onset and time since onset of first symptom, the possible confounding effects from early age at onset were statistically controlled by using a partial correlation analysis. In general, the correlations between the two measures of untreated initial psychosis and quality of life 6 months after the first hospitalization were weak at best (
Table 2). None of these outcome measures reached the critical p value of 0.004.
Symptom Severity and Remission of Positive Symptoms
At the 6-month follow-up evaluation, the disorganized and psychotic symptoms were of mild severity, and the negative symptoms were of moderate severity (
Table 2). The correlations between duration of untreated initial psychosis and symptom severity were again weak.
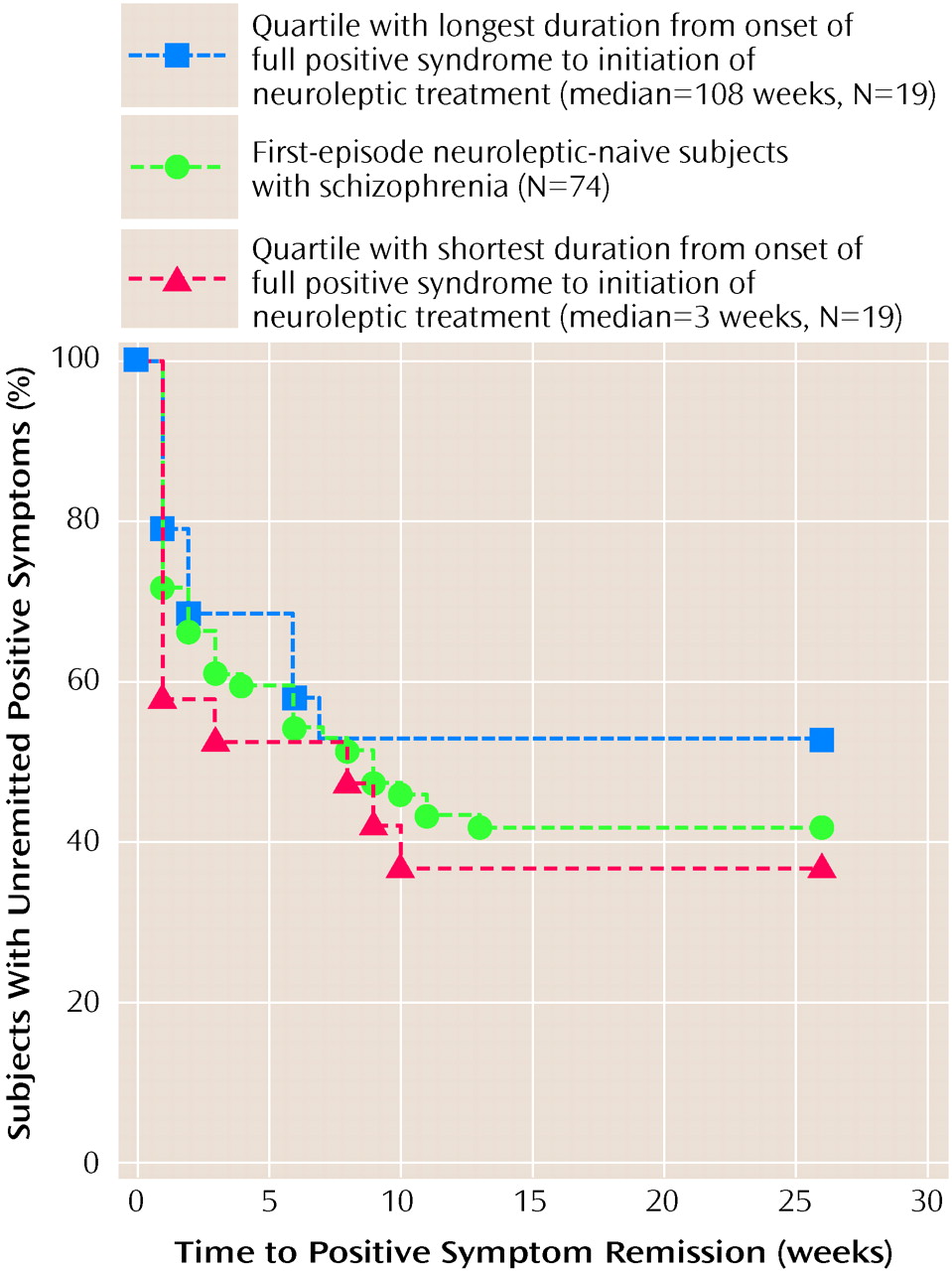
The median time to remission of positive symptoms was 9 weeks after discharge from inpatient hospitalization. Only 58.1% (N=43) of the patients met criteria for positive symptom remission at 6 months (
Figure 1). Neither measure of untreated initial psychosis duration approached significance based on the survival analysis (log rank test c
2<0.07, df=1, p values >0.80), indicating no evidence for an effect of untreated initial psychosis duration on positive symptom remission.
We did an extreme groups analysis that compared subjects in the first quartile (median time from onset of full psychotic syndrome to treatment: 3 weeks) with those in the fourth quartile (median time from onset of full psychotic syndrome to treatment: 108 weeks) to further explore the effects of an extremely long duration of untreated initial psychosis. The pattern of results was similar to the correlation analyses. The quality of life and symptom severity of subjects whose durations of untreated initial psychosis were in the fourth quartile were not significantly worse than those of the first quartile (t values <2.5, df=36, p values >0.02). A stepwise discriminant analysis was also performed to find out which factors (quality of life and symptom severity measures at 6 months) best separated the groups with short and long durations of untreated initial psychosis. The only factor that discriminated the two groups was quality of family relationships (F=5.59, df=1, 35, p<0.02), which correctly identified 68.4% (N=13) of the subjects in the first quartile group and 63.2% (N=12) of the fourth quartile group.
Discussion
In this study of first-episode neuroleptic-naive subjects, we were interested in knowing what effects untreated initial psychosis has on outcome in schizophrenia. We first examined whether duration of untreated initial psychosis was related to known predictors of outcome (i.e., gender, age at onset of illness, and premorbid functioning) so as to better estimate the unique prognostic value of untreated initial psychosis. Only age at onset of illness was associated with untreated prodromal psychotic symptoms. There were no significant gender differences nor were there any significant associations between untreated initial psychosis duration and premorbid functioning. After partialing out the effects of age at onset, untreated initial psychosis duration did not significantly impair quality of life, symptom severity, or remission of positive symptoms 6 months after the first psychiatric hospitalization for treatment of schizophrenia.
While symptom severity and symptom remission are important measures of outcome, researchers have increasingly focused their attention on quality of life to arrive at a more comprehensive measure of outcome in schizophrenia. Assessing the quality of life allows one to understand the impact of schizophrenia on the patient’s general well-being, role functioning, and community integration. In our study, longer duration of untreated initial psychosis was not significantly associated with poorer quality of life. The median Spearman’s correlation coefficient between untreated initial psychosis duration and the different subjective and objective indicators of quality of life was only 0.115.
Unlike previous studies
(10,
36), we did not find longer duration of untreated initial psychosis to predict poorer positive symptom remission. This may be related to the frequency of assessment. Although we used all available information to arrive at the best estimate of symptom severity for each week during the past 6 months, the accuracy of such an estimate is less than when subjects were reevaluated more frequently (fortnightly to monthly in the study by Loebel et al.
[10]). Nevertheless, when symptom ratings for the previous week were obtained at the 6-month follow-up evaluation, there were still no significant correlations between positive symptoms and duration of untreated initial psychosis. Another possible reason for the lack of association between untreated initial psychosis duration and positive symptom remission may be related to the relatively short follow-up length. Hence, future studies will need to assess outcome after longer follow-up periods.
Duration of untreated initial psychosis is difficult to ascertain since the onset of psychosis is often subtle and insidious. Like previous studies
(10,
36,
62), we have used similar dual definitions of untreated initial psychosis duration, i.e., dating from the onset of first nonspecific psychiatric symptoms as well as from the onset of more specific psychotic symptoms. Although such definitions allow for comparison across studies, the latter definition (time since onset of full psychotic syndrome) may be more relevant in studies examining the effects of untreated psychosis. Nevertheless, the lengthiness and wide variance for both measures of untreated initial psychosis duration in our study are comparable with those found in previous first-episode studies
(10,
36,
62). Half of our patient group had experienced prodromal symptoms for greater than a year or had had severe psychotic symptoms for more than 3 months before they sought treatment. Many factors are likely to affect how soon after the onset of symptoms that patients with schizophrenia seek treatment. A wide array of sociocultural factors (such as educational level of patient and family members, socioeconomic status, availability and access to health care, beliefs and knowledge about mental illness, integrity of social support network) and psychopathological factors (e.g., insidious mode at onset, bizarre and disruptive behaviors, level of insight into illness and the need for treatment) may interact together to influence treatment-seeking behaviors
(63–
68). The net result of the interplay of these factors within the patient, and between the patient and his or her environment (family members and sometimes with the legal system as well), could either shorten or lengthen the duration of untreated initial psychosis.
Some investigators have proposed that there may be a threshold duration of untreated initial psychosis above which subsequent functioning may be impaired. However, such a relationship remains unclear, since these studies have significant methodological limitations. Browne and colleagues
(28) reported on a cohort of 53 patients with schizophrenia or schizophreniform disorder for which the median duration of untreated initial psychosis was 6 months. However, 43.3% of the subjects had durations greater than 12 months, and when the investigators compared these patients with the rest of the cohort, they found that the former group had significantly poorer quality of life at the time of presentation for treatment. However, whether poor quality of life persists on subsequent follow-up remains to be seen. In another study, McGorry et al.
(29) reported that patients with untreated initial psychosis durations greater than 28 days had poorer outcome at 12-month follow-up (i.e., slower remission of psychotic symptoms, greater symptom severity, and poorer quality of life) than those whose durations were less than 28 days. But only 40.5% of their patients met DSM-III-R criteria for schizophrenia or schizoaffective disorder, and 24% met criteria for schizophreniform disorder. A substantial proportion of the group (21.5%) consisted of patients with affective psychosis. More importantly, there were highly significant differences in untreated initial psychosis duration between diagnostic categories: the median duration of untreated psychosis in the schizophrenia-only group was 122.0 days, whereas the schizophreniform group and the remaining subjects had median durations of 10.5 and 14.0 days, respectively. McGorry et al.’s finding of poorer outcome among patients with longer durations of untreated initial psychosis may have been confounded by diagnosis. Patients with affective psychosis had shorter untreated initial psychosis durations, and, in general, they have better outcomes than do patients with schizophrenia.
In our extreme groups analysis, the minimum and median times from the onset of full psychotic syndrome to treatment for the group of patients in the fourth quartile were 50 weeks and more than 2 years, respectively. Yet, their quality of life, symptom severity, or rate of positive symptom remission were not significantly worse than those of patients in the first quartile (whose median and maximum times from onset of full psychotic syndrome to treatment were 3 weeks and 5 weeks, respectively). Thus, our data suggest that if there is a threshold duration of untreated initial psychosis above which subsequent outcome may be impaired, this threshold is greater than 50 weeks and may very likely be much longer than that.
Waddington et al.
(25) and Scully et al.
(26) have found longer duration of untreated initial psychosis to be associated with severe negative symptoms and cognitive dysfunction in a cohort of chronic schizophrenia patients with extremely long durations of untreated psychosis (means of 13.9 and 17.1 years). Because these patients became ill during the preneuroleptic era, psychosis had been left untreated for long periods of time—much longer than those of modern-day patients with schizophrenia. Under current psychiatric practice, such extremely long durations are seen only in a minority of patients and therefore may not be clinically relevant for the average patient with schizophrenia today.
Overall, the findings from this study bode well for patients. Despite the fact that many patients experienced long periods of untreated initial psychosis, this delay in seeking treatment does not appear to significantly impair subsequent outcome for the average patient with schizophrenia. These results also have implications for the debate about placebo controls in clinical drug trials, the use of “drug holidays,” and the advantages or disadvantages of medication discontinuation or withdrawal
(24,
41–
43). It appears unlikely that the brief periods of psychosis (lasting several hours to several weeks) that may occur during challenge studies or medication discontinuation will have adverse effects on subsequent symptom severity, psychosocial functioning, or quality of life.
Of course, our findings do not argue against preventive measures for schizophrenia. In fact, future studies should aim toward better understanding of why most patients wait so long before seeking treatment. Interventions to increase the public’s awareness and understanding of this devastating illness and its treatment may help bring patients to seek treatment sooner, and thereby reduce their suffering during the initial psychosis. Such long durations of untreated psychosis are clearly undesirable, since the psychotic experience is usually unpleasant, bewildering, and even painful to the patient and his or her family.
The hypothesis that untreated psychosis may be “biologically toxic” remains unsubstantiated. Clinical outcome studies alone, even those with the most robust methodology, can only provide indirect evidence to support or refute such a hypothesis. To effectively test the “toxic psychosis” hypothesis, biological measures of “toxicity” are likely to be more sensitive than the duration of psychosis. Such biological measures, which may include neuroimaging, neurochemistry, and neuropathology, are needed to provide more direct evidence as to whether untreated psychosis represents an “active morbid process” that is deleterious to outcome in people with schizophrenia.