The subjective experience of patients treated with antipsychotic medication is related to quality of life
(1) and predicts medication compliance
(1–
3). Subjectively experienced side effects are more distressing than other side effects
(4).
Occupancy of dopamine D
2 receptors in the striatum by antipsychotic medication is thought to influence patients’ subjective experiences. The influence of cocaine on the dopamine system has a profound effect on subjective experience
(5). The striatum is involved in the control of motivation and reward. Extrapyramidal symptoms are related to D
2 receptor occupancy
(6), and, in particular, akathisia has an important subjective component.
Olanzapine and risperidone may be associated with a better subjective experience than typical antipsychotic drugs
(7,
8). However, if the severity of negative subjective experience is related to D
2 receptor occupancy of olanzapine or risperidone, then these agents might not demonstrate more benefits for subjective experience than typical antipsychotic drugs in doses that lead to the same range of D
2 receptor occupancy
(9).
In this study, we evaluated the relationship between subjective experience and striatal D2 receptor occupancy in patients whose schizophrenia was stabilized by olanzapine or risperidone.
Method
Twenty-one patients with schizophrenia and one patient with schizoaffective disorder, diagnosed according to DSM-IV criteria, were included in the study. Four of the patients were female and 18 were male; their mean age was 22 years (SD=4, range=16–28). Exclusion criteria were neurological or endocrine disease and mental retardation. Nine healthy comparison subjects were also included; their mean age was 24. After a complete description of the study to the subjects, written informed consent was obtained from all.
Patients’ subjective experience during the previous 7 days was measured with the Subjective Well-Being Under Neuroleptic Treatment Scale
(1) and the Subjective Deficit Syndrome Scale
(10).
Patients’ psychopathology was assessed with the Positive and Negative Syndrome Scale and the Montgomery-Åsberg Depression Rating Scale. Extrapyramidal symptoms and akathisia were assessed with the Simpson-Angus Rating Scale (range=0–40) and the Barnes Rating Scale for Drug-Induced Akathisia, respectively.
Single photon emission computed tomography imaging (SPECT) was performed with a brain-dedicated SPECT camera 2 hours after intravenous injection of 110 MBq of iodobenzamide ([
123I]]IBZM). Specifications and imaging procedures have been described elsewhere
(11). SPECT imaging was performed after a stable dose period of at least 6 weeks of olanzapine (N=15, mean dose=14.7 mg, SD=5.8, range=5–30) or risperidone (N=7, mean dose=4.1 mg, SD=0.9, range=3–6).
Subjective experience, psychopathology, and extrapyramidal symptoms were assessed within 2 days after SPECT imaging. None of the patients used alcohol, cannabis, or other nonprescribed drugs. Patients were blind to the main goal of this study, i.e., assessment of the relationship between medication and subjective experience.
Semiquantification of [
123I]IBZM binding was performed by placing a template of fixed regions of interest over the striatum and occipital cortex
(12). Specific striatal binding was defined as striatal binding divided by occipital binding
(12). All analyses were performed blind to clinical data. The nine healthy comparison subjects had a mean [
123I]IBZM binding ratio of 1.92 (SD=0.08), which was used to calculate the percentage of occupancy by medication as (ratio striatum/occipital region) – 1/(1.92 – 1)×(–100) + 100
(11).
We conducted one-tailed analyses because we hypothesized that high D2 receptor occupancy was related to worse subjective experience. Analyses were performed for the total group of patients (N=22) and for the group receiving olanzapine (N=15). Analyses for the subgroup using risperidone were not performed because there was minimal variation of doses in this group.
Results
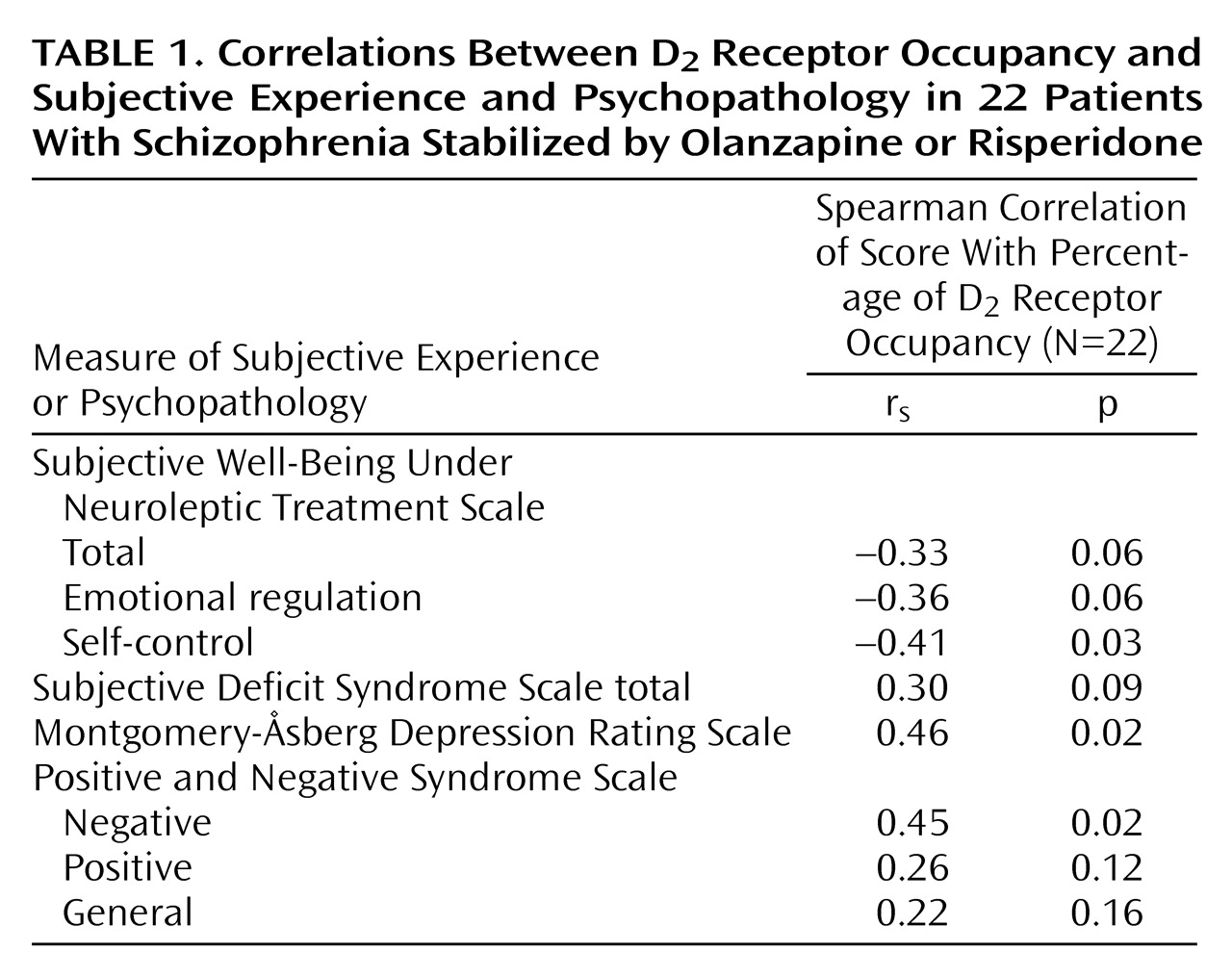
Both self-control and emotional regulation items on the Subjective Well-Being Under Neuroleptic Treatment Scale correlated with the percentage of D
2 receptor occupancy (
Table 1). Positive and Negative Syndrome Scale negative symptom ratings and Montgomery-Åsberg Depression Rating Scale scores also correlated with D
2 receptor occupancy (
Table 1). Other Positive and Negative Syndrome Scale subscale ratings were not significantly correlated with D
2 receptor occupancy.
Simpson-Angus ratings were zero in most patients, but two patients each had a total score of 3 and two patients each had a total score of 4. Six patients had a score of 2 on the Barnes scale. Extrapyramidal symptoms were not correlated with percentage of D2 receptor occupancy.
In the subgroup of patients using olanzapine, a significant correlation was found between D2 receptor occupancy percentages and the Subjective Well-Being Under Neuroleptic Treatment Scale self-control score (rs=–0.53, N=15, p=0.02) and the Subjective Deficit Syndrome Scale total score (rs=0.45, N=15, p=0.05). Olanzapine dose correlated with D2 receptor occupancy (rs=0.60, N=15, p=0.01).
The average D2 receptor occupancy was 67% in the olanzapine group and 77% in the risperidone group. The correlations found would not have reached statistical significance if they had been corrected for multiple comparisons by the Bonferroni test.
Discussion
We found a correlation between striatal D
2 receptor occupancy by olanzapine and risperidone and subjective experience, negative symptoms, and depression, in the absence of extrapyramidal symptoms. Higher doses of olanzapine were correlated with higher D
2 receptor occupancy and worse subjective experience. Negative subjective experience might be more sensitive to D
2 receptor occupancy than extrapyramidal symptoms. The substantial D
2 receptor occupancy of olanzapine and risperidone we found is in agreement with the recent findings of others
(9).
Our study design permitted assessment only of correlations between subjective experience and D2 receptor occupancy. Therefore, a longitudinal study is required to confirm these results, since a relationship between higher D2 receptor occupancy and worse subjective experience may have important implications for dosing strategies and compliance with antipsychotic medication.