Schizophrenia is a lifelong psychotic illness that begins in the early adult years. It is characterized by bizarre mental, cognitive, and affective symptoms, of both positive and negative types
(1). While some aspects of its biology are known
(2), the critical components of its pathophysiology remain to be discovered. Its course includes acute psychotic episodes and quiescent periods with residual symptoms, in highly variable combinations
(3–
8). Since 1974 it has been recognized that psychosis, negative symptoms, and social functioning are relatively independent domains
(9). In 1982 Andreasen and Olson
(10) separated positive psychosis into reality distortion and disorganization, and many studies have confirmed the three-factor symptom clusters
(1,
11). Whether these symptom dimensions represent distinct illnesses with their own etiologies and pathophysiologies or are merely multiple manifestations of a single illness has been a topic of repeated discussion
(9,
12–
16).
Primary negative symptoms, often called deficit symptoms, are manifestations of schizophrenia. Studying them to answer questions of etiology and mechanism has often been hampered by the almost ubiquitous confound of secondary negative symptoms, which influence deficit ratings. Secondary negative symptoms may occur because of depression, paranoia, medication side effects, and other conditions. We have proposed that decisive studies on the biology of deficit symptoms be based on contrasting deficit schizophrenia with nondeficit schizophrenia
(14). Already, distinguishing biologic characteristics of patients with primary deficit symptoms have been defined on the basis of genetic
(17,
18), risk factor
(19), electrophysiologic
(20,
21), and biochemical
(22,
23) studies. In a preliminary study
(24), we showed that patients with deficit schizophrenia had lower levels of neuronal activity at rest in the middle frontal cortex, inferior parietal cortex, and thalamus than did patients with nondeficit schizophrenia.
The development of modern techniques for human brain imaging has powerfully advanced not only our understanding of normal brain function, but also our concepts of human brain diseases. Brains of individuals with a defined CNS illness or subtype can be directly studied in vivo for CNS structural, neurochemical, or functional abnormalities characteristic of the brain disease. Functional human brain imaging is ideally suited to studying subgroup characteristics in schizophrenia, because the usual illness confounds among the patient volunteers are similar in the subgroups. These confounds include long-term administration of antipsychotic and anticholinergic medication, environmental deprivation, lifelong exposure to trauma and institutionalization, and other factors. Already, imaging techniques have advanced our basic knowledge of schizophrenia
(25–
35). In particular, several studies have already shown that positive and negative symptom dimensions are associated with different patterns of regional activation. Regional analyses of the correlations between primary negative symptoms and regional cerebral blood flow (rCBF) have implicated the middle frontal regions and inferior frontal cortex
(27,
36), as have dichotomies analyses contrasting subjects with and without primary negative symptoms
(24,
37).
Therefore, we hypothesized that low rCBF in the middle frontal and inferior parietal cortices bilaterally would occur with performance of an effortful task in deficit schizophrenia. In order to test this hypothesis, we recruited schizophrenic volunteers with and without deficit symptoms but similar in other symptom domains. The two groups were contrasted, without centrally active medication, with matched healthy volunteers free from all CNS disease. Using rCBF measures, we evaluated all volunteers with [
15O]H
2O and positron emission tomography (PET), performed during an effortful auditory discrimination task in which performance was matched across groups. We previously reported
(38) that when the total group of patients was compared to the normal volunteers, the patients with schizophrenia had less activity in the anterior cingulate.
Method
Volunteers
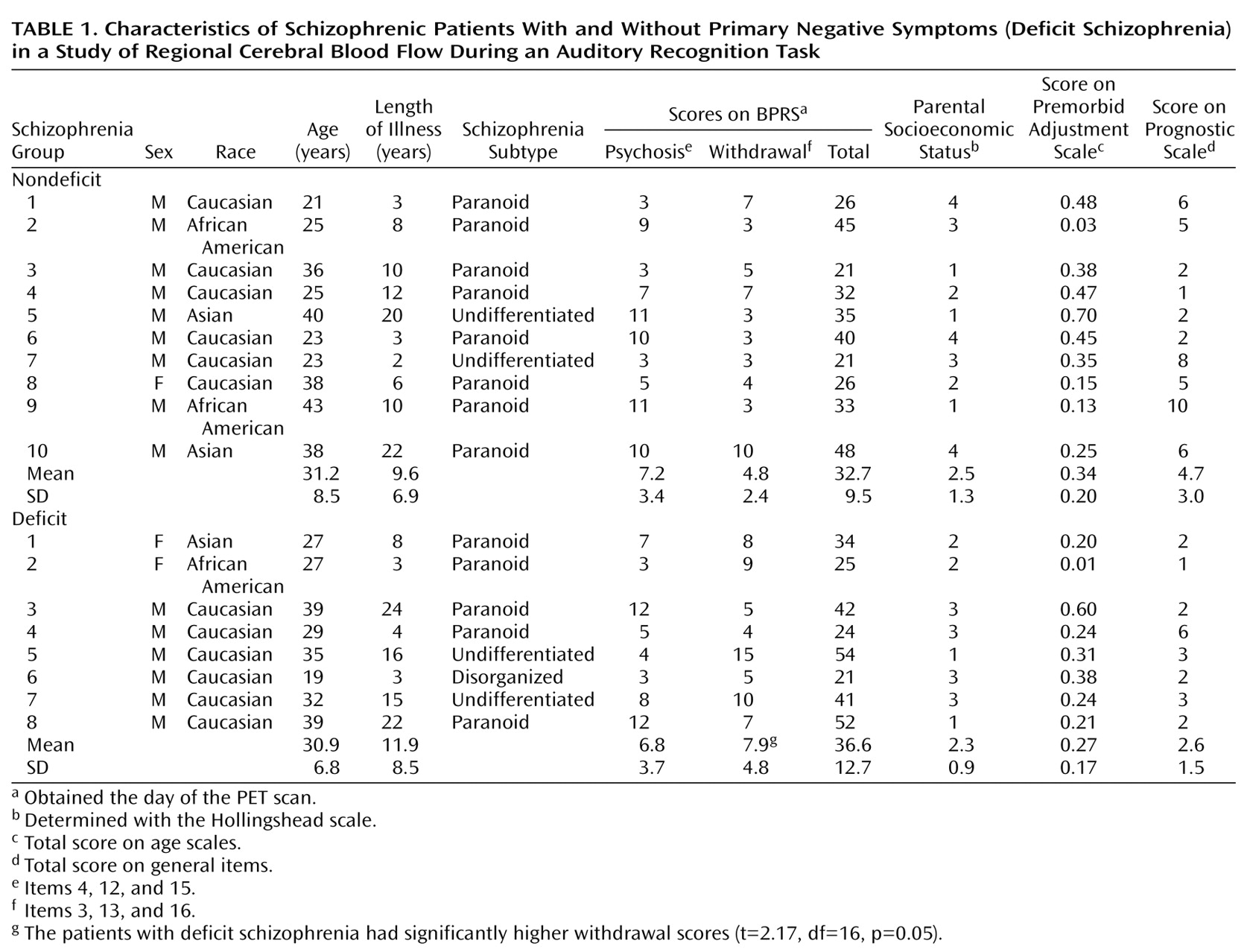
Eighteen medically healthy schizophrenic persons were recruited from the Residential Research Unit of the Maryland Psychiatric Research Center in Baltimore. Each underwent a Structured Clinical Interview for DSM-III-R (SCID) at hospital admission. Two research psychiatrists (A.C.L., M.A.W.) reached a consensus diagnosis of schizophrenia (according to DSM-III-R criteria) on the basis of the clinical interview and all other sources of data. The diagnosis of deficit syndrome (primary negative symptoms) was made by using the Schedule for the Deficit Syndrome
(39). This instrument allows the categorization of schizophrenic patients into those with and those without deficit symptoms on the basis of a semistructured interview. Diagnostic categorization is achieved through the use of operational criteria taking into account six negative symptoms (restricted affect, diminished emotional range, poverty of speech, curbing of interests, diminished sense of purpose, and diminished social drive), their stability over time, and whether the symptoms are primary or secondary (for instance, not secondary to factors such as neuroleptic akinesia, paranoid withdrawal, depressive anhedonia, withdrawal during compelling psychotic experience). This instrument has demonstrated good reliability in the schizophrenic population (kappa=0.73).
The total schizophrenia volunteer group included 15 male and three female persons with a mean age of 31.6 years (SD=7.7). Seventeen of the 18 schizophrenic volunteers were right-handed.
The schizophrenic volunteers, all inpatients, were treated with a fixed dose (0.3 mg/kg) of haloperidol and no other neurally active medications for at least 4 weeks before the study. A drug-free period followed haloperidol treatment. All other aspects of inpatient treatment were continued. Symptoms of schizophrenia were assessed repeatedly during the haloperidol baseline and during the subsequent drug-free period by using the Brief Psychiatric Rating Scale (BPRS)
(40). Symptoms were rated by two trained raters, and a consensus rating was obtained. Clinical monitoring was continuous, and intervention was available when there was a clinical judgment of significant behavioral change requiring treatment.
Twelve healthy volunteers were recruited from the community through newspaper advertising and were screened by telephone for generally good medical health and the lack of major psychiatric illness. If suitable, they were further screened in face-to-face interviews using the Structured Clinical Interview for DSM-III-R—Non-Patient Edition and the Structured Interview for DSM-III-R Personality Disorders
(41) to rule out current or past history of axis I or axis II disorders. Family history of schizophrenia in any first-degree relative of the prospective healthy volunteer was ruled out by clinical interview. Six comparison subjects were male, and six were female. All were right-handed, and their mean age was 28.4 years (SD=4.6).
Informed Consent
The normal and schizophrenic volunteers were fully informed about the nature of the protocol, and afterward each gave informed consent. Only patients who were competent and clinically judged to be capable of understanding and appreciating the risks involved in this study were selected to participate. The nature of the protocol was presented on several occasions by separate people, including both the principal investigator (A.C.L.) and noninvestigator clinicians. Family members or care givers were involved in the information process when available.
Tasks
The decision condition was a forced-choice auditory discrimination task. The subject was instructed to immediately press a button held in the right hand when he or she recognized a high-frequency reference tone (1500 Hz) and to press the button in his or her left hand with a lower-frequency tone (800–1492 Hz). Equal numbers of high and low tones, each lasting 100 msec, were randomly presented in each stimulus condition; there were 100 trials in each training set and 60 trials in each imaging set. The interval between trials (onset of first tone to onset of subsequent tone) was 2 seconds. Failure to respond was scored as an error. Response time was calculated as the time from the onset of the stimulus to the button press.
During the active control task (sensory-motor task), the subject heard the same sets of tones that were presented during the decision task. However, he or she was instructed to merely press the right- and left-hand buttons alternately after each tone.
During the rest condition, the subject was instructed to lie quietly. Eyes were open, and earphones were in place during all scans.
Training
All subjects began training on the decision task 2–5 weeks before the scan sessions. Training occurred in a quiet, isolated room. The purposes of the training were to eliminate stimulus or task novelty, determine what frequency difference reliably provided 70%–80% accuracy in performance by the subject, and reduce performance variability within and between volunteer groups. Each volunteer participated in three to five sessions, and there were six training blocks per session. The patients began training during the haloperidol treatment phase and continued throughout the medication withdrawal period.
The tones presented during training were systematically modified by decreasing the frequency difference between the reference and test tones, as the subjects became increasingly accurate in recognizing the two types of stimuli. In the first training session the frequency differences between the high and low tones ranged from 700 to 20 Hz. If a subject was unable to perform with at least 80% accuracy at the largest frequency difference (700 Hz) after three attempts at training, the subject was dropped from further study.
PET Imaging
PET scans were obtained by using the General Electric (Milwaukee) 4096+ system, which produces 15 brain image slices at an intrinsic resolution of 6.1 mm in each dimension. The bolus [
15O]H
2O method
(42) was used without arterial blood sampling. Approximately 62 mCi of [
15O]H
2O were administered on each occasion. Ten to twelve minutes elapsed between scans. The relative CBF distribution was measured in each of three conditions—1) rest, 2) sensory-motor control task, and 3) decision task—with four scans per condition (12 scans per subject). The order of the scans was fixed for all subjects: rest, control task, decision task, consecutively repeated four times. In the rest condition the subject was inactive, with eyes open and ears unplugged; tone stimuli and motor activity were absent, but the earphones were in place. The sensory-motor control task consisted of exposure to the same tones presented during the decision task with alternation of right and left button presses in synchrony with the tones. During the decision task the subject was asked to press the right button when a high-frequency tone was recognized and the left button when a low-frequency tone was detected. Within a given scan the frequencies of the two tones were held constant. The frequencies were chosen on the basis of the training accuracy for that individual. Sixty trials were delivered during each scan; the tones began 15 seconds before tracer delivery, and scan acquisition began 20 seconds after dose delivery. PET data were acquired for 60 seconds.
Image Analysis
The quantitative PET blood flow images were analyzed with modified statistical parametric mapping routines
(43). The scans from each subject were realigned by using the first one as a reference. The alignment procedure was modified to use 10 iterations to optimize the spatial correlation between data sets; the default procedure uses three iterations. After realignment, all images were transformed into a standard anatomical space
(44). Before generation of the statistical parametric map, the data were smoothed by using a 12-mm Gaussian kernel. Only clusters of connected voxels (face or edge) above a threshold (z=2.33, p=0.01, one-tailed, uncorrected for multiple comparisons) were tested for significance by means of spatial extent statistical theory, and significance was set at an alpha level of <0.05 after correction for multiple comparisons
(43). The full width at half maximum of the average noise subtraction image was used to determine the number of resels
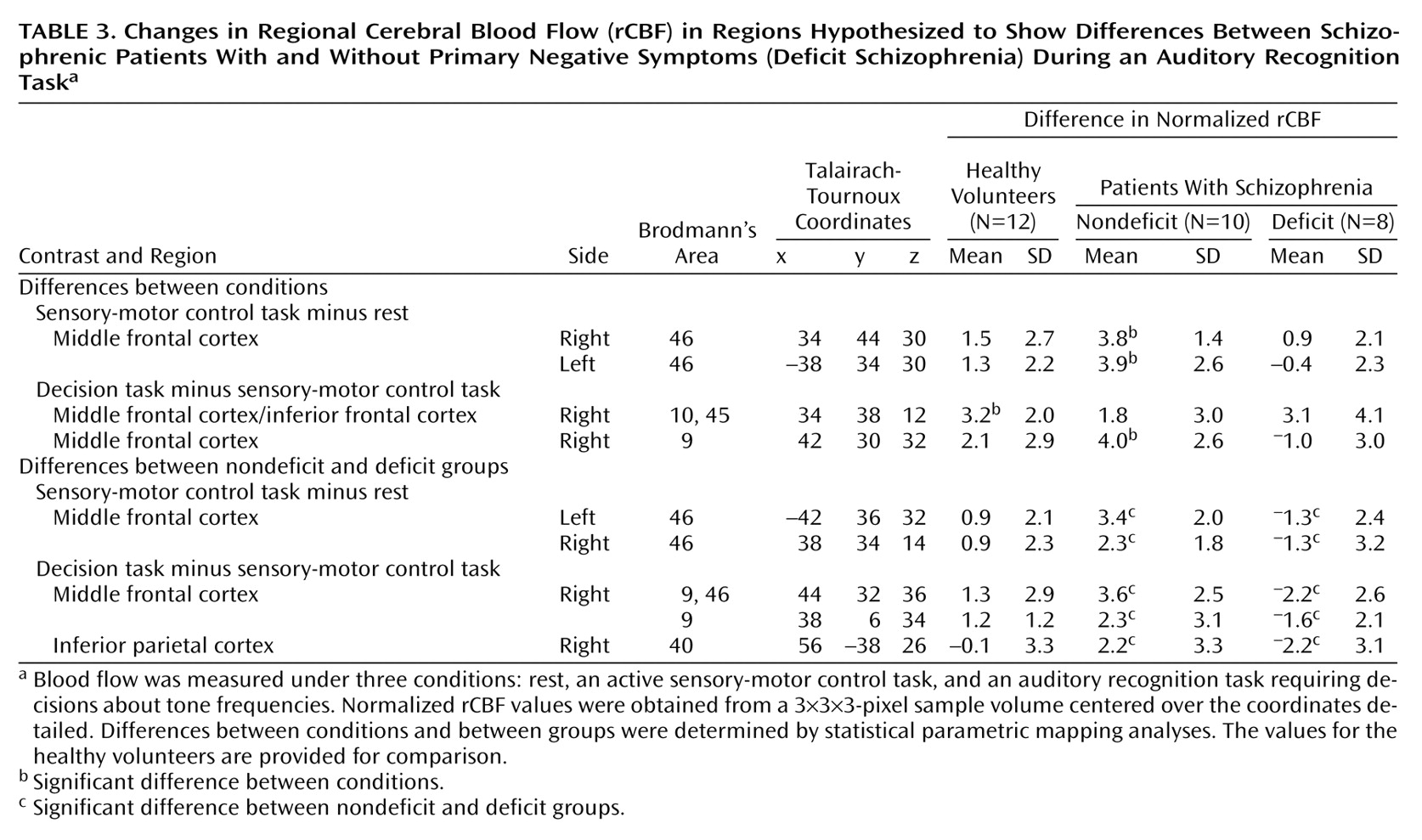
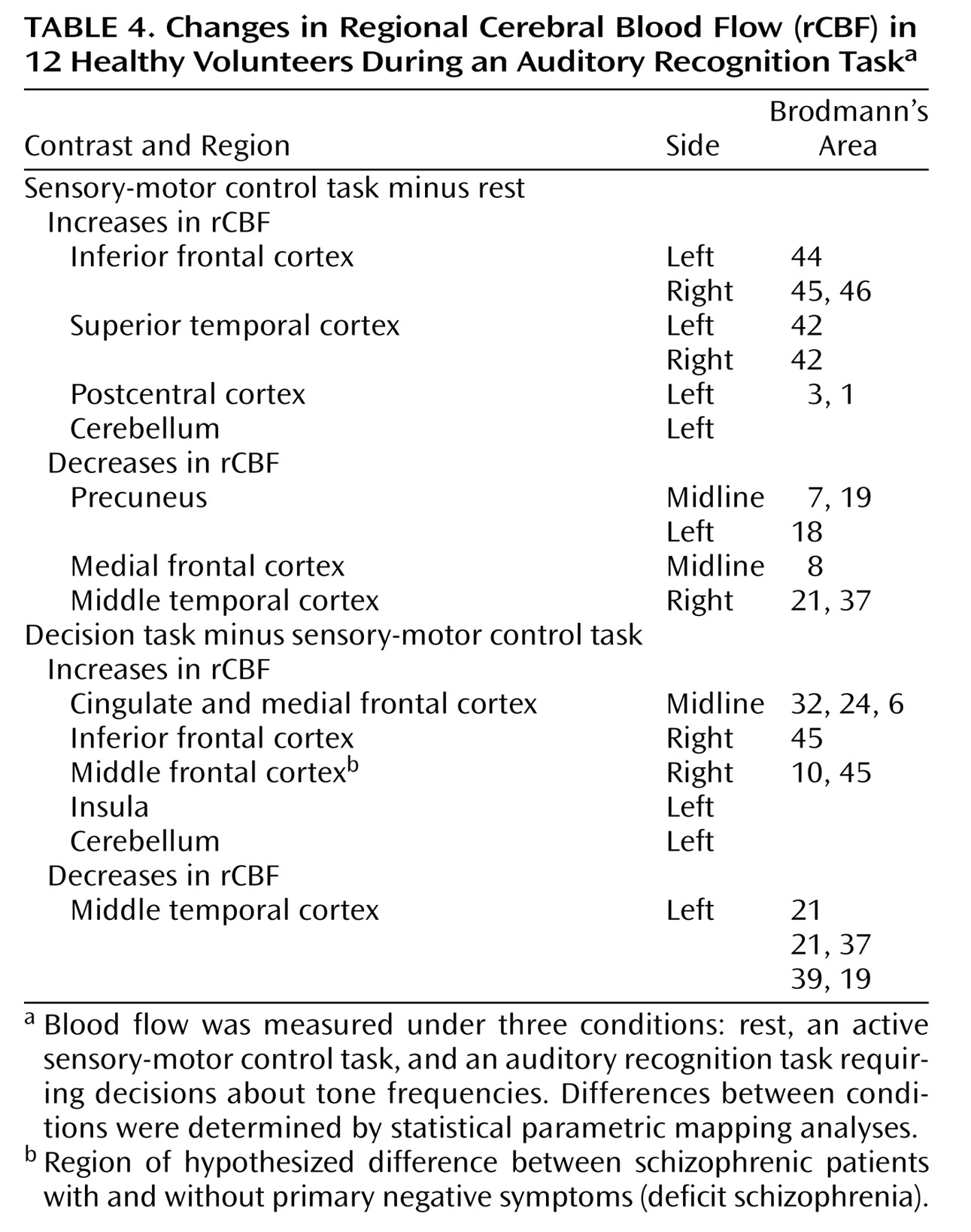
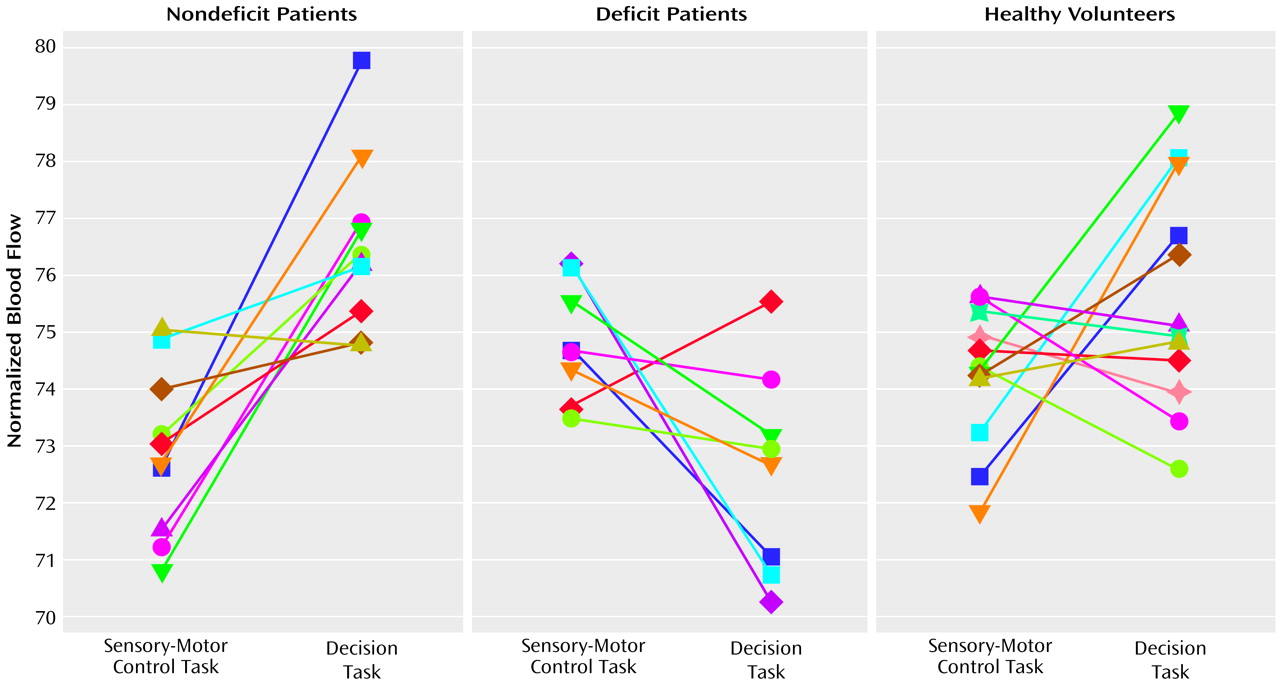
(45) available for analysis. Task-related changes in rCBF between the control task and rest and between the control task and decision task were evaluated for each volunteer group; increases and decreases were assessed. Patients with deficit schizophrenia were compared to patients with nondeficit schizophrenia on the same contrasts. The spatial/anatomical distribution and extent of each cluster was mapped onto matching magnetic resonance images aligned and warped to “fit” the statistical data. For hypothesized effects, an uncorrected significance level of alpha=0.05 was used to determine significant areas of activation. For all other analyses, a multiple comparison correction was used. In regions of hypothesized differences, the maxima of significant clusters in the statistical parametric mapping analysis were grown to a 3×3×3-pixel sample volume; adjusted rCBF values were obtained in these samples for each task condition.
By means of Pearson’s product moment correlations, days of medication withdrawal in all patients were correlated with rCBF in regions showing differences between patients with deficit and nondeficit schizophrenia. Similarly, negative symptoms as measured on the BPRS withdrawal subscale were correlated with rCBF in these regions for the patients with deficit schizophrenia only.
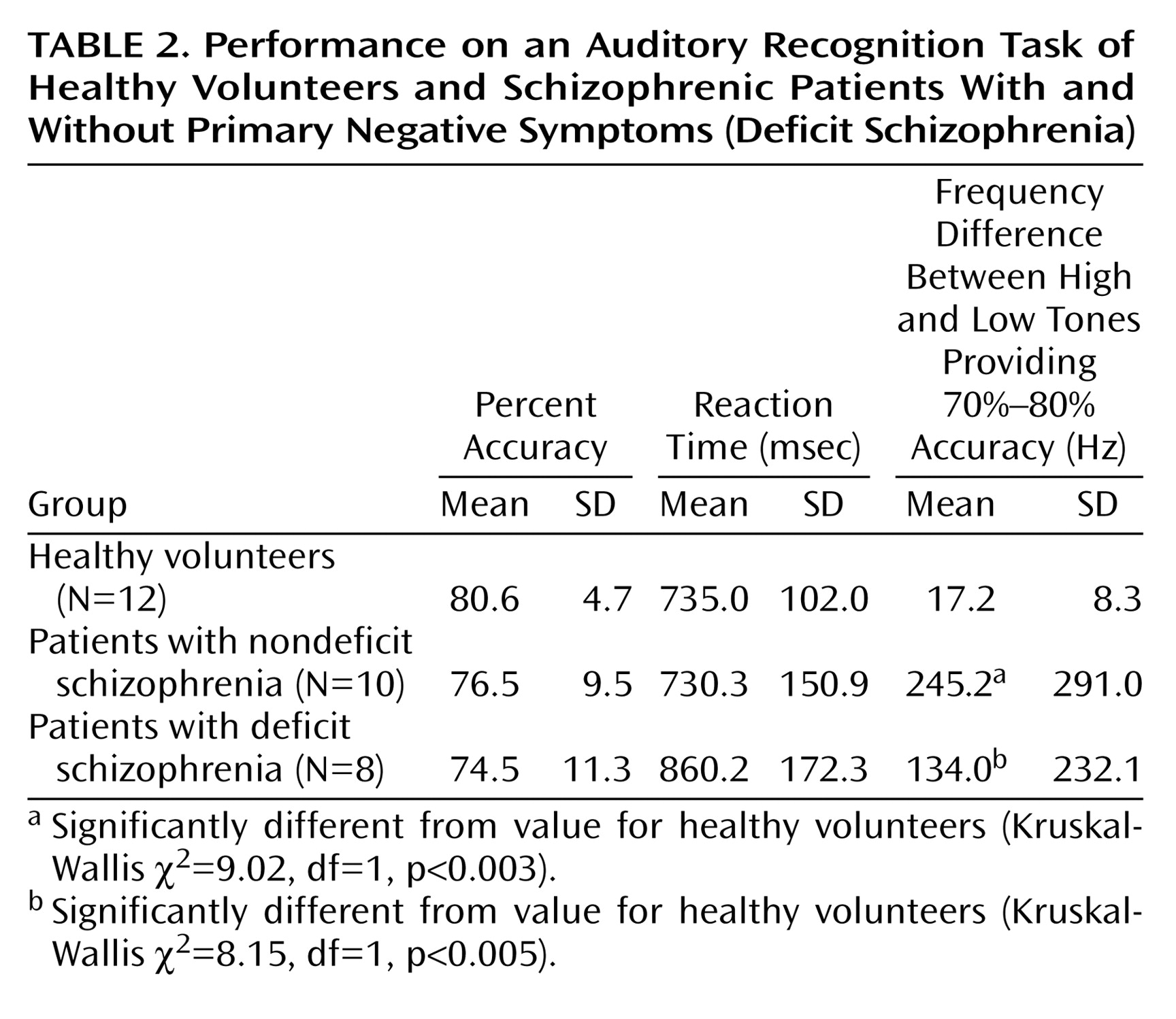
Behavioral outcome measures were extracted from all trials generated in the PET scan sessions during the control and decision tasks. These measures include mean accuracy, mean response time, and mean frequency differences between high and low tones for accurate trials. Differences among the three groups on those measures were each tested by using a Kruskal-Wallis test. Significant results were further tested by performing a Wilcoxon rank sum test on all pairs.
Discussion
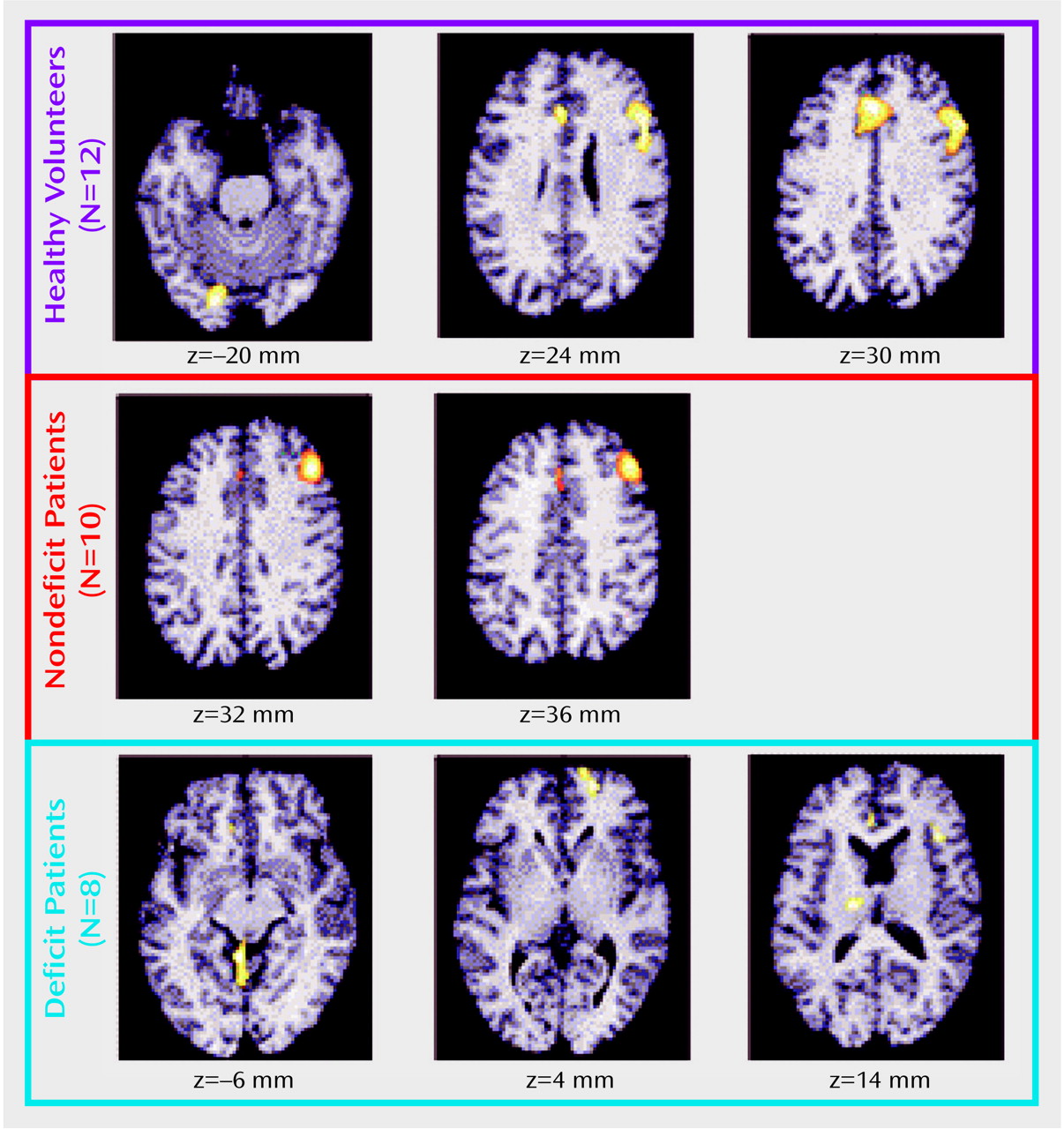
These data show that medication-free schizophrenic individuals who differ from each other primarily on the basis of the presence or absence of enduring negative symptoms differ profoundly in the pattern of rCBF abnormalities that is generated with effortful task performance, even when performance of the task is standardized. We have previously reported
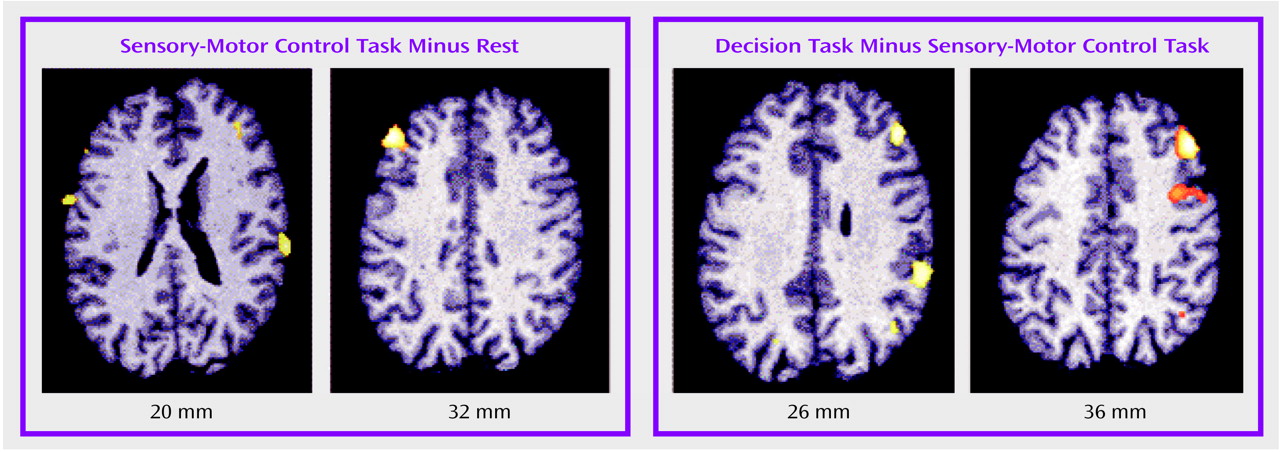
(46) that the normal individuals scanned for this study experience activation of the auditory and motor cortex with the sensory-motor control condition and activation of the anterior cingulate and right frontal cortex with the effortful decision task. Moreover, the task-activated rCBF pattern of the entire schizophrenia group (N=18) differed from the normal pattern only in the anterior cingulate cortex, where rCBF was lower in the patients with schizophrenia
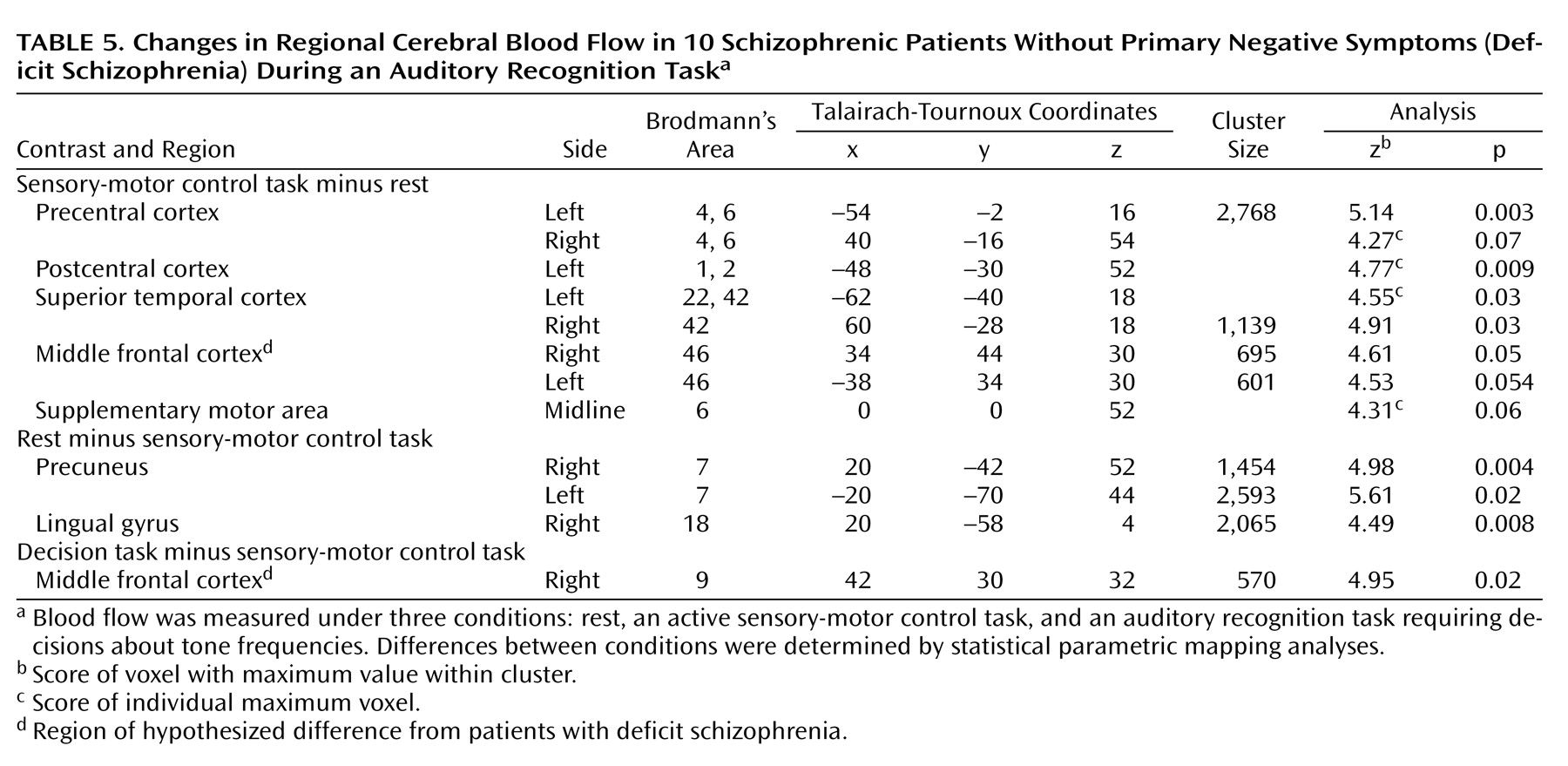
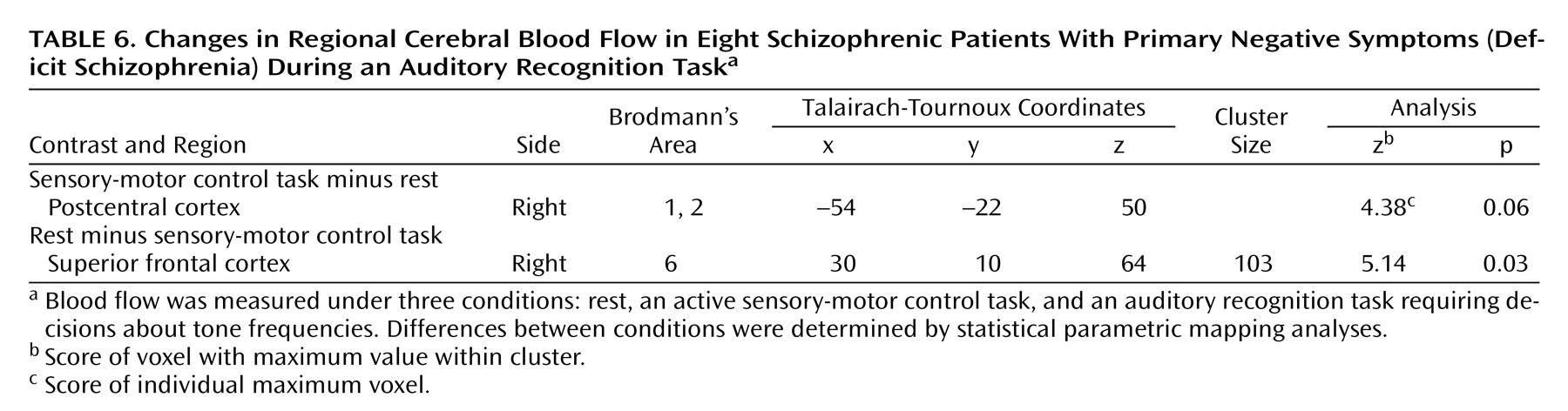
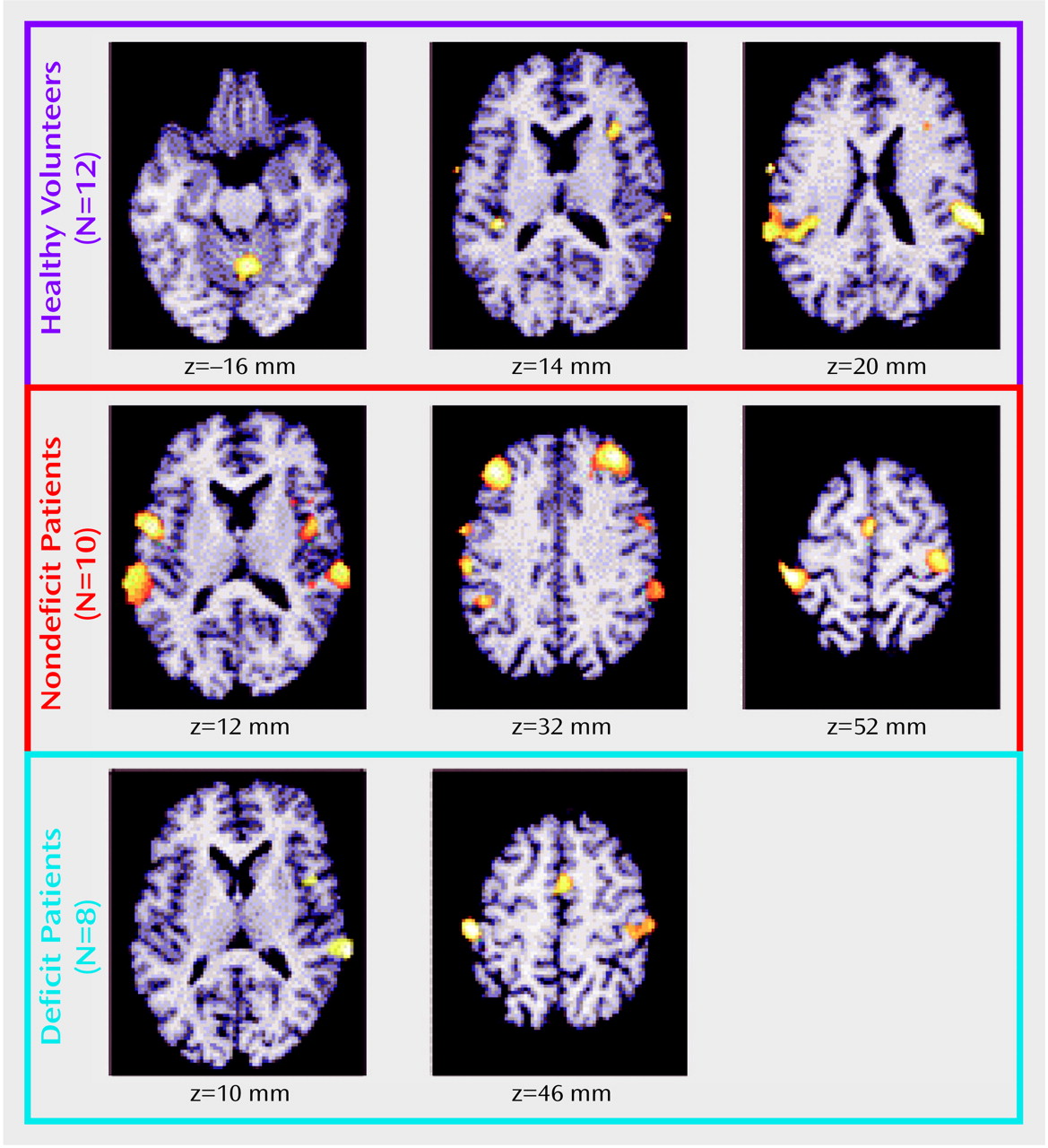
(38). Here we report that the deficit schizophrenia group showed low rCBF activation in the left and right middle frontal cortex during the control task and in the right middle frontal and right inferior parietal area during the effortful task. These flow differences occurred despite matched behavioral performance across the three groups. Moreover, these data may explain previous reports of “hypofrontality” in schizophrenia studies with skewed subject subgroups. When the two patient groups in this study were compared to normal volunteers, both showed significant hypoactivation of the anterior cingulate during the effortful task. Neither of the groups showed hypofrontality when contrasted to the normal volunteers.
In this study and in others
(9,
12,
14–
16,
27), a pathologic dimension within the schizophrenia syndrome was isolated in an attempt to establish homogenous subgroups with distinguishing physiologic, pharmacologic, and anatomic characteristics. Functional imaging analysis provided a critical tool in this comparison of these two populations of psychiatric patients, who were matched on key illness features (positive symptoms and illness characteristics) but were divergent on a single disease characteristic (primary negative symptoms). In this study patients with deficit and nondeficit schizophrenia were prospectively identified by using operational criteria for the presence or the absence of enduring negative symptoms
(39). All patients were medication free and trained to perform an auditory discrimination task at similar levels of performance, matched to that of healthy volunteers. Under these conditions, the lower rCBF in deficit schizophrenia in the middle frontal cortex and in the right inferior parietal cortex represents a regional functional deficit without performance confound. Although the patients were medication free for a mean period of 3 weeks, we cannot be certain that their brain function had returned to premedication status at the time of scanning. Postmortem studies
(47) have shown that antipsychotic medications are eliminated slowly from brain tissue. Further preclinical studies
(48) reveal slow return of receptor function to normal after exposure to antipsychotic medications. These are important considerations. However, because we did not find any correlations between the number of days of medication withdrawal and rCBF in regions showing group differences, we believe that residual medication effects did not significantly alter the results. The findings presented here replicate and extend the results of our previous PET/fluorodeoxyglucose study
(24), in which patients with primary negative symptom had low rates of glucose metabolism at rest in the middle frontal and inferior parietal cortices bilaterally.
These results are limited by several considerations. The number of patients was low, particularly in the group with deficit schizophrenia. So, despite the fact that clusters failed to develop in the deficit group as in the normal subjects, even at nonsignificant levels, low subject number and possibly greater task-associated regional variability may explain the failure to find an activation in the subjects with deficit schizophrenia. Moreover, although the subject groups were matched on performance, the frequency required to standardize performance at 70%–80% accuracy was highly variable across groups. These limitations introduce added variability into the results. However, these effects appear insufficient to account entirely for these results.
Low frontal cortex metabolism in deficit, but not nondeficit, schizophrenia has been observed in several other functional imaging laboratories
(27,
36,
37,
49,
50); low CBF in the inferior parietal cortex has been reported as well
(37). These regional associations between brain metabolism and negative symptoms, or the deficit state, in schizophrenia have characteristically been based on correlational analyses
(49,
51,
52) or factor analyses
(27,
50,
53,
54). Few studies have used a categorical approach (i.e., dichotomization according to a disease characteristic) to contrast flow characteristics across symptom domains
(24,
37). Moreover, because antipsychotic medications already reduce regional metabolism in the frontal cortex
(55), concurrent treatment with medications becomes a critical confound in studies conducted without withdrawal.
Heterogeneity of cerebral regions that behave abnormally within the diagnostic category of schizophrenia raises the question of whether schizophrenia, as we diagnose it, is a single disease with multiple manifestations or multiple diseases all within a distinct pathophysiology. While these data can illustrate the dilemma, they cannot answer the question. However, these data demonstrate the problem associated with grouping individual results into mean values across all schizophrenia subjects and the possibility of obscuring significant underlying pathology. The dichotomy of primary negative versus nonnegative symptoms of schizophrenia appears to have reduced the heterogeneity in this experiment, and other phenomenologic dichotomies may accomplish the same purpose.
These data provide additional evidence associating human behaviors with lower than normal functioning of the middle frontal cortex and inferior parietal cortex. We can speculate that deficit or primary negative symptoms, like impaired aspects of social affiliation, impaired interpersonal communication, and minimal goal-directed cognitive performance, are generated by functional failures of neuronal populations in these regions. The normal functions of the middle frontal cortex have been inferred from lesion studies and human in vivo functional imaging experiments. Overall, lesion studies suggest the involvement of this area in personality expression and certain aspects of cognition
(56,
57). The specific cognitive processes mediated by the middle frontal cortex depend on region and laterality
(58). In vivo functional imaging studies implicate this area (Brodmann’s area 9/46) in working memory (verbal on left and nonverbal on right), episodic retrieval, semantic processing, spatial processing (right hemisphere), and attention
(59). Multiple type of experiments with humans and primates
(60–
63) implicate the inferior parietal cortex in visuomotor integration and spatial attention processing. In imaging studies
(64–
67), the inferior parietal cortex is activated by tasks requiring selective visual attention and spatial processing. Lesions of the inferior parietal cortex in humans are associated with the inability to look on command at a visual target, with optic ataxia, and with oculomotor deficits. Some but not all of the functions associated with these regions are deficient in schizophrenia. Attention, working memory, and executive function are the deficits most often mentioned
(68–
70). Buchanan and colleagues
(11,
71) have reported that subjects with deficit symptoms have worse neurocognitive performance than nondeficit patients. Patients with deficit symptoms may not be able to integrate internal and external representations or sensory cues in an adaptive, rapid manner. Parietal lobe dysfunction may be responsible for this integrative failure. A secondary consequence of parietal lobe failure may be withdrawal from social and environmental novelty.
These data demonstrate functional heterogeneity within the overall diagnosis of schizophrenia, an observation that has implications for diagnosis and clinical management of the illness. This heterogeneity has been reduced by the deficit/nondeficit dichotomization. Whether both subgroups have the same underlying pathology, only differently distributed, or entirely different pathologies is still a matter of conjecture. In either case, these kinds of data can advance the field by suggesting a focus for studies of postmortem tissue pathology. Prospective analyses of postmortem tissue from these hypothesized regions of the brains of people with schizophrenia have already been productive
(72,
73). Although it is premature to suggest the diagnostic use of rCBF patterns, one could propose this rCBF abnormality associated with the deficit state as a surrogate marker of primary negative symptoms in the illness and as a target rCBF pattern for development of new therapies for negative symptoms. Currently there is no treatment for deficit symptoms in schizophrenia, and clinical outcome for this patient group is poor
(74,
75). For these reasons, the needs for advances in the treatment of this schizophrenia cohort and technical tools to expedite discovery are particularly pressing.