Screening Questionnaire
A brief screening instrument was developed with the objective of identifying individuals with symptoms of PTSD, panic disorder, social phobia, generalized anxiety disorder, OCD, major depressive disorder, or suicidal ideation. The questionnaire also probes readiness for treatment, history, functional impairment, and demographic characteristics.
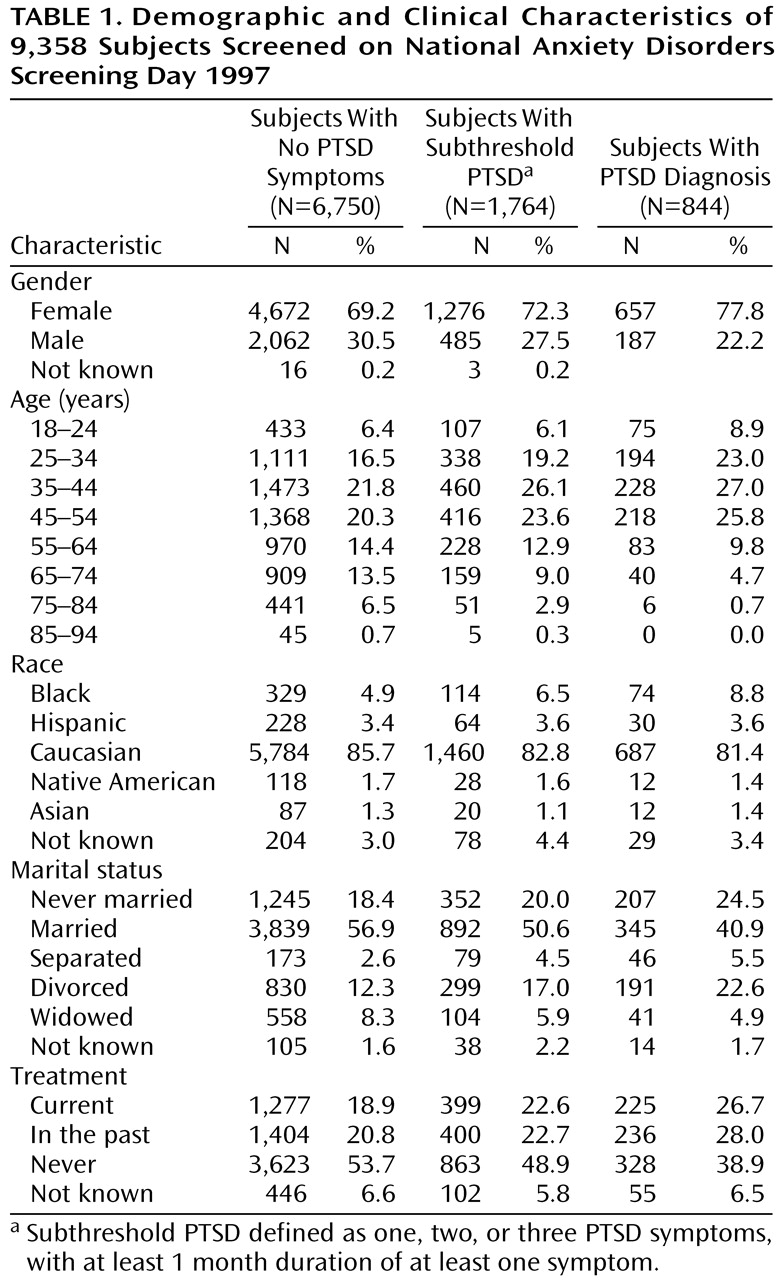
Given that the goal of the instrument is to rapidly and reliably identify individuals who may be in need of treatment, a disorder was defined as present on the basis of key features of the disorder. To assess PTSD, the screening instrument first assesses for history of a criterion A trauma with the following question: Have you ever had an extremely frightening, traumatic, or horrible experience like being the victim of a violent crime, seriously injured in an accident, sexually assaulted, seeing someone seriously injured or killed, or been the victim of a natural disaster? The instrument then assesses four symptom clusters: reexperiencing (Did you relive the experience through recurrent dreams, preoccupations, or flashbacks?), withdrawal/loss of interest (Did you seem less interested in important things, not “with it,” or unable to experience or express emotions?), insomnia (Did you have problems sleeping, concentrating, or have a short temper?), avoidance (Did you avoid any place or anything that reminded you of the original horrible event), and duration of symptoms for longer than 1 month. For this study, a subject was included in data analyses if he or she reported a criterion A trauma and reported at least one symptom lasting at least 1 month.
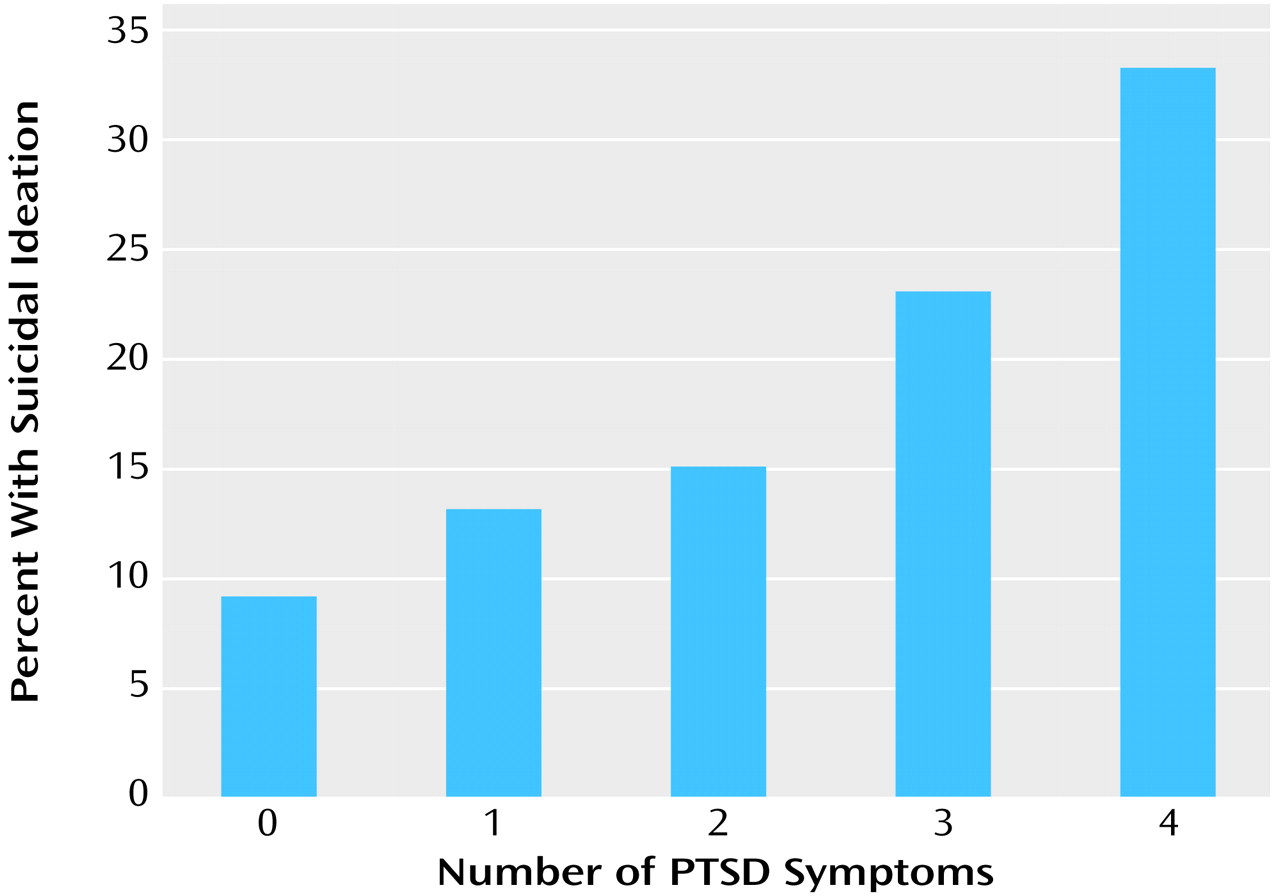
The following definitions were used for the other anxiety disorders. Panic disorder was diagnosed if individuals reported having a sudden, unexplained panic attack, plus two of the following: 1) fear of having more attacks, 2) fear of losing control, having a heart attack, or going crazy, and 3) change in behavior because of the attacks. Generalized anxiety disorder was diagnosed if individuals reported 1) persistent worry about several different things, such as work, school, family, money, and others, and 2) finding it difficult to control the worrying. OCD was diagnosed if individuals reported 1) having persistent senseless thoughts such as thoughts about death, illnesses, aggression, sexual urges, or contamination, and 2) spending more time than was necessary doing things over and over again, such as washing hands, checking things, or counting things. Social phobia was diagnosed if individuals reported 1) fearing being observed by others doing things such as public speaking, eating, performing, or teaching, and 2) feeling uncomfortable at social events. Major depressive disorder was diagnosed if individuals reported four of the following: 1) often feeling sad or depressed, 2) having stopped enjoying the same pleasures enjoyed in the past, 3) experiencing difficulty concentrating, making decisions, or completing tasks, 4) having difficulty sleeping or staying asleep, 5) usually feeling hopeless about the future. To assess suicidal ideation, subjects were asked if they had “recently (during the past month) thought of or are currently thinking of suicide.”
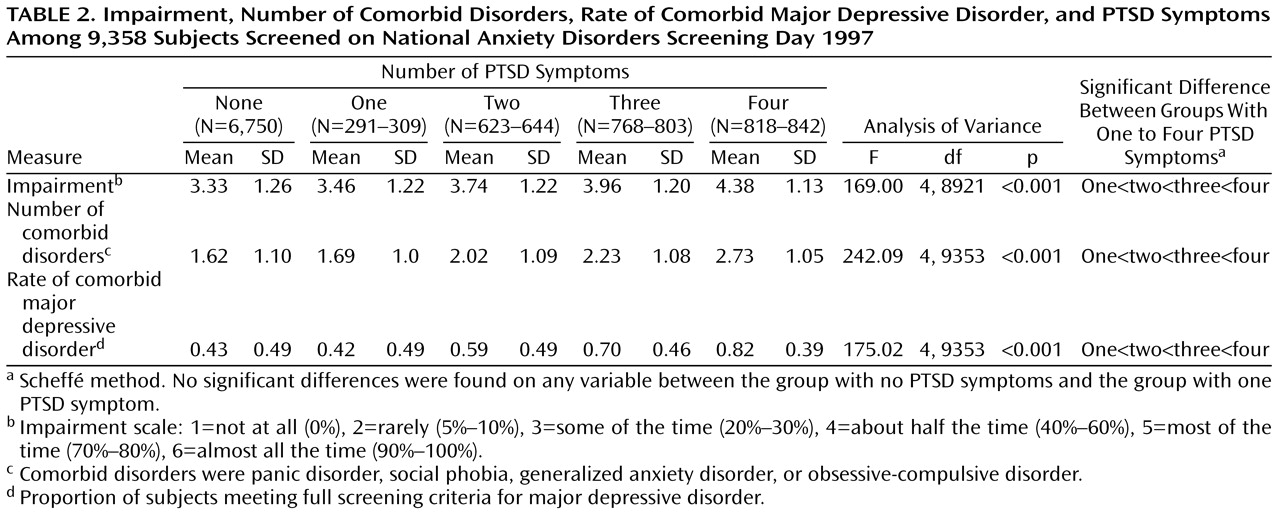
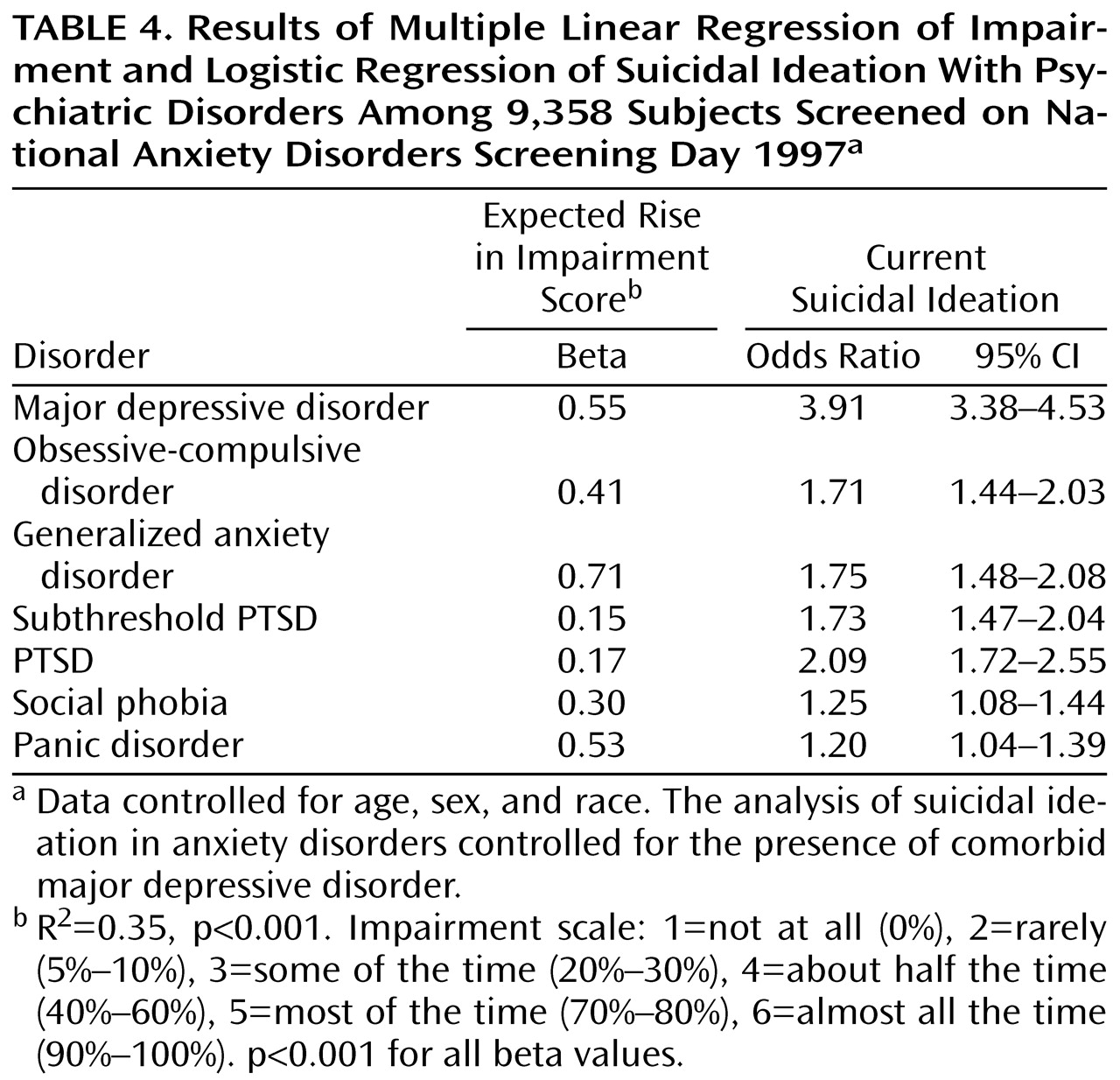
To assess impairment, the following question was asked: During the past month, how much of the time does your anxiety interfere with your daily life? The answer choices were 1) not at all (0%), 2) rarely (5%–10%), 3) some of the time (20%–30%), 4) about half the time (40%–60%), 5) most of the time (70%–80%), and 6) almost all the time (90%–100%).
To assess the screening instrument’s psychometric properties, a subgroup of individuals (N=203) were given the screening questionnaire, followed by a Structured Clinical Interview for DSM-IV. Sensitivity, specificity, and kappa, respectively, for each disorder were as follows: PTSD, 0.62, 0.94, 0.44; OCD, 0.5, 0.91, 0.39; major depressive disorder, 0.80, 0.72, 0.44; generalized anxiety disorder, 0.89, 0.55, 0.34; panic disorder, 0.87, 0.72, 0.50; and social phobia, 0.64, 0.85, 0.46. Mean sensitivity was 0.70, and mean specificity was 0.79. This demonstrates acceptable psychometric properties for a screening instrument (defined by Landis and Koch
[23] as kappa between 0.40 and 0.75).