Fulton County, Ga., contains virtually the entire city of Atlanta. The population of Fulton County is approximately 800,000 and has been growing at 2% per year. The population of Fulton County is divided nearly in half along ethnic lines (49% African American, 48% white, and 3% other). The goal of this study was to determine the role of cocaine and ethanol in all completed suicides in Fulton County during the second half of the 1990s. This time period was chosen because it was the most recent for which records could be obtained and hence the most relevant to current circumstances. The underlying hypothesis was that the pattern of substance use preceding suicide would be specific for different ethnic, gender, and age groups.
Results
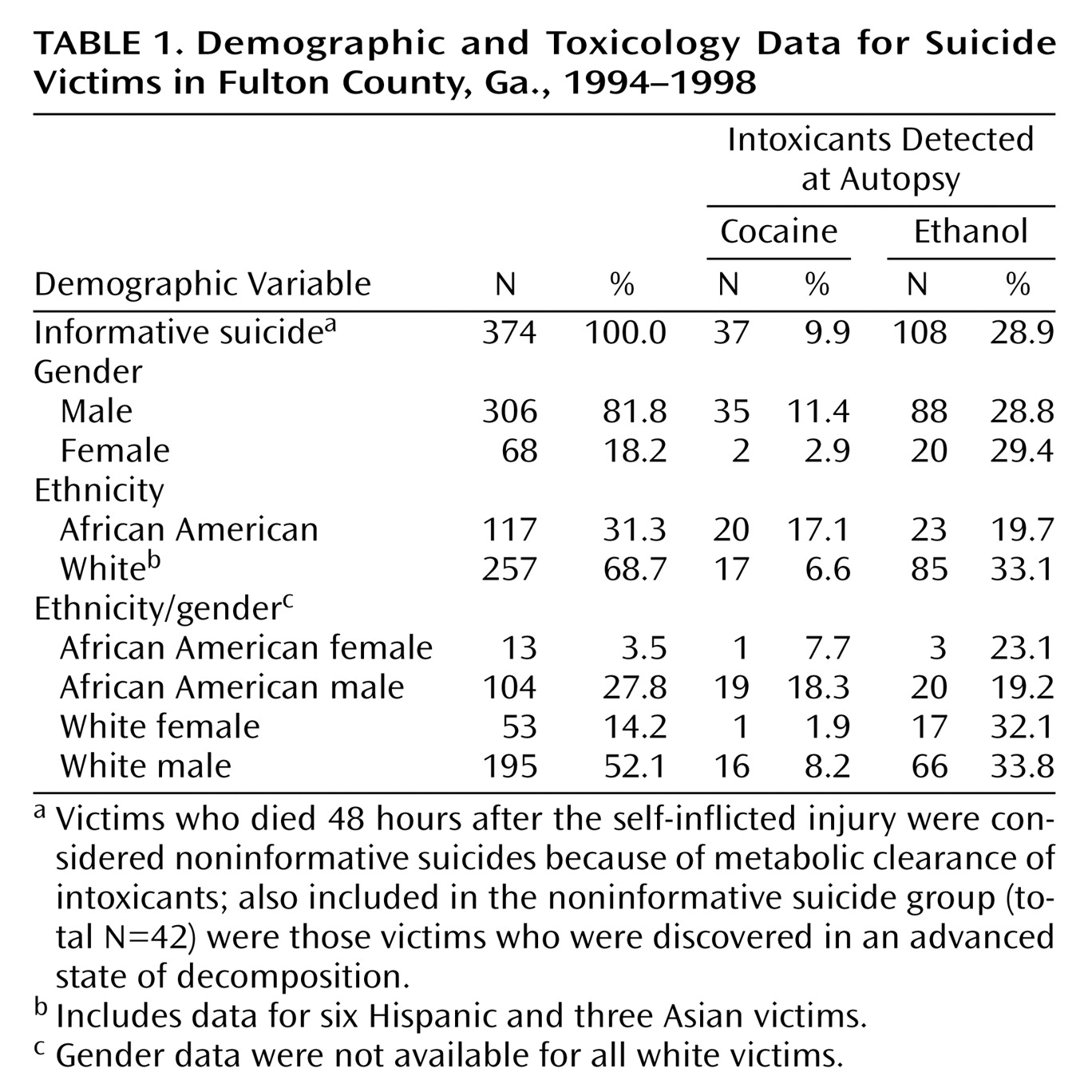
There were 416 suicides in Fulton County between 1994 and 1998, 374 (89.9%) of which were fully informative with regard to cocaine and ethanol toxicology. There were no significant differences between the informative and noninformative suicide groups in mean age (43.9 years [SD=18.5] and 38.6 years [SD=14.5], respectively), age distribution, demographic composition, method of suicide, or violence of method. Demographic and toxicology data of the informative suicides are presented in
Table 1. Since there were only six Hispanic and three Asian victims in the entire data set (2.4%), they were included in the white group in subsequent analyses. Most suicides were violent (84.5%, N=316), the dominant method involving use of a firearm (62.6%, N=234).
Cocaine was detected in 37 (9.9%) of the suicide victims. Cocaine-positive victims (mean=32.4 years, SD=8.2) were significantly younger than cocaine-negative victims (mean=45.2 years, SD=18.9) (F=16.57, df=1, 372, p<0.0001). All of the cocaine-positive victims were clustered between 16 and 50 years of age. Across all age groups, 17.1% of African American victims used cocaine before committing suicide, whereas 6.6% of white victims used the drug (χ2=8.76, df=1, p=0.003). Of all cocaine-positive victims, 54.1% (N=20) were African American, and 45.9% (N=17) were white. Almost all (94.6%, N=35) of the cocaine-positive victims were male (χ2=3.60, df=1, p<0.06). Across all male victims, 11.4% were cocaine positive compared with only 2.9% of all female victims. There were more African American male victims (51.4%) and fewer white male victims (43.2%) and white female victims (2.7%) than expected in the cocaine-positive group (χ2=13.16, df=3, p=0.004). There was no relationship between cocaine and method of suicide, use of firearm, or violence of method.
Of the cocaine-positive suicides, 11 (29.7%) also tested positive for ethanol. The dual substance subjects were indistinguishable from the cocaine group in demographic characteristics and in method and violence of method.
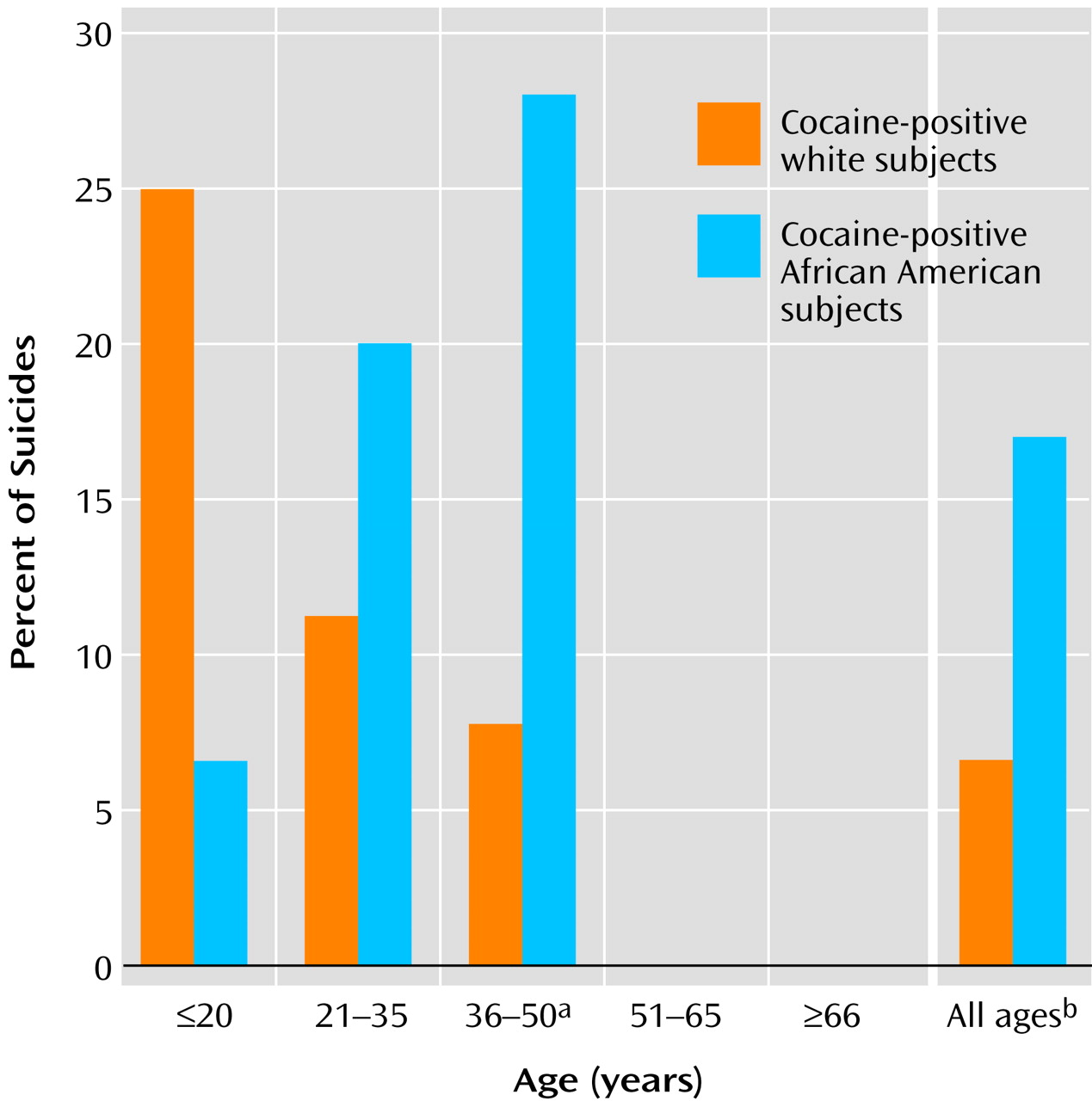
The pattern of cocaine use differed depending on the age of the victim (
Figure 1). Of the white teenage victims, 25.0% (N=3 of 12) were cocaine positive compared with only 6.7% (N=1 of 15) of the African American teenage victims. In the young adults (21–35 years of age), 20.0% (N=10 of 50) of all African American suicide victims were cocaine positive, and 11.3% (N=8 of 71) of white victims were cocaine positive. A significant difference was seen among the middle-age adults (36–50 years of age), in which 28.1% (N=9 of 32) of all African American victims were cocaine positive as opposed to 7.8% (N=6 of 77) of all white victims (
Figure 1). Of all the suicide victims 50 years of age and under, 16.6% (N=35 of 211) of the male suicide victims were cocaine positive compared with 4.3% (N=2 of 46) of the female suicide victims (χ
2=3.66, df=1, p<0.06). Among this same age group, 20.6% (N=20 of 97) of the African American victims were cocaine positive compared with 10.6% (N=17 of 160) of white victims (χ
2=4.89, df=1, p=0.02). Within each age group and across all suicides, there was no relationship between cocaine use and method of suicide, use of firearms, or violence of method.
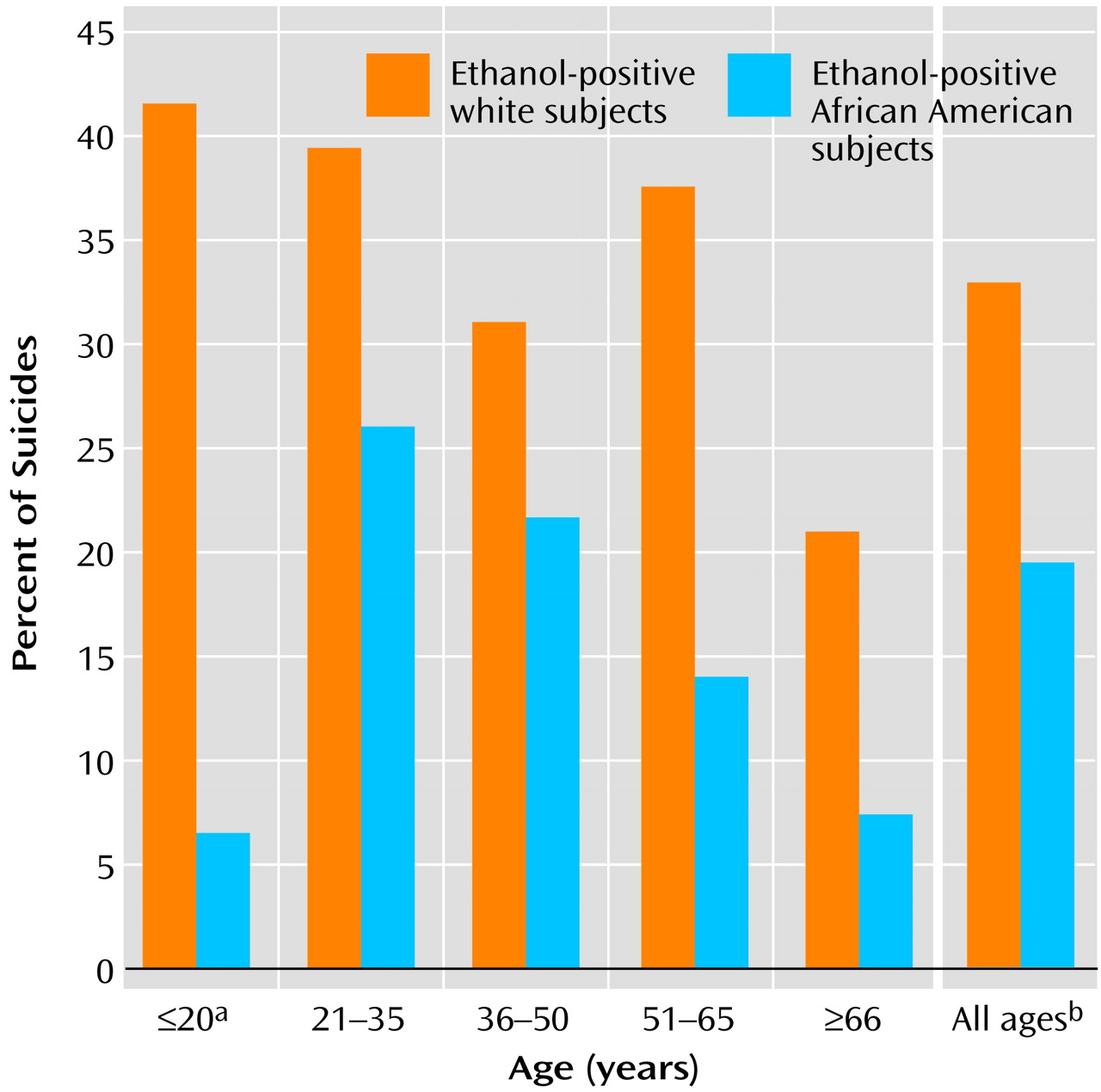
Alcohol was detected in 108 (28.9%) of the 374 informative suicides. Of the ethanol-positive victims, 25.0% (N=27) had blood alcohol levels below 80 μg/dl (designated as low), and 75.0% (N=81) had levels above 80 μg/dl (designated as high). The average age of the ethanol-positive victims (42.1 years, SD=15.9) did not differ from that of the ethanol-negative group (44.7 years, SD=19.5). Significantly more of the white suicide victims (33.1%) than African American victims (19.7%) were ethanol positive (
Figure 2). Of the white suicide victims, 24.7% (N=21) had blood alcohol levels in the low range, and 75.3% (N=64) were in the high range; of the African American victims 26.1% (N=6) had low levels, and 73.9% (N=17) had high levels. There were no gender-based differences in ethanol use: 29.4% of all female victims and 28.8% of all male victims were ethanol positive, and male and female victims had similar percentages with low and high blood alcohol levels. The rates of ethanol use by ethnicity/gender were identical to those associated with ethnicity alone (
Table 1). There was no relationship between ethanol use and method of suicide, use of firearms, or violence of method.
In all age brackets, more white victims used ethanol before committing suicide than African Americans (
Figure 2). Unlike cocaine, ethanol use before suicide occurred in every age bracket. The distribution of ages for the ethanol-positive suicides (17 to 81 years) coincided with the age distribution of all informative suicides (13 to 88 years).
Among teenagers, intoxicant use before suicide differed dramatically between ethnic groups. Cocaine and ethanol results were combined and designated as substance positive versus substance negative. Of the African American teenage victims, 86.7% (N=13 of 15) were substance negative at autopsy, whereas 50.0% (N=6 of 12) of the white victims were substance positive (χ2=2.77, df=1, p=0.09). One African American victim had used cocaine, and one had used ethanol before committing suicide. Five white teenagers (41.7%) had used ethanol (χ2=2.98, df=1, p=0.08), three had used cocaine, and two had used both substances. African American male subjects were the largest group of teenage suicide victims, but 85.7% (N=12 of 14) were substance negative. Of the white male teenagers, 44.4% (N=4 of 9) were substance positive, and 66.7% (N=2 of 3) of the white female victims were substance positive. The white female victims had both used ethanol and of the male victims, one had used cocaine, one had used ethanol, and two had used both. There was no relationship between substance use and method of suicide, use of firearms, or violence of method. Consistent with the larger data set, 63% of all teenage suicides were by firearm.
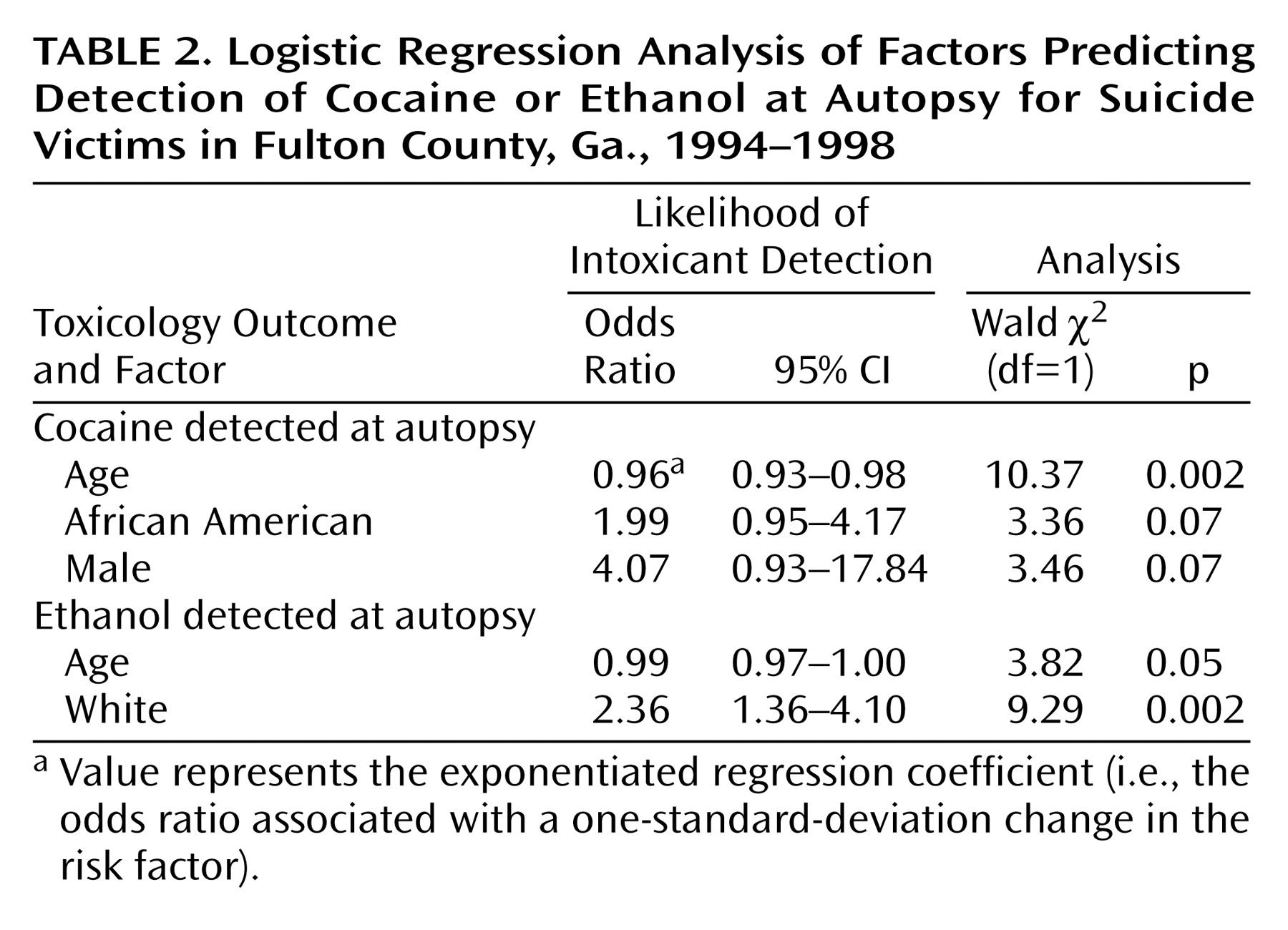
A series of logistic regression models were calculated to test the effect of various demographic factors (age, race, sex, use of ethanol or cocaine, method, violence, and use of firearms) on the likelihood of cocaine or ethanol use before suicide. Relative to cocaine use, variables that were significant or approached significance in the multivariable model were age (log likelihood χ
2=12.89, df=1, p=0.0003), sex (log likelihood χ
2=4.92, df=1, p<0.03), and race (log likelihood χ
2=3.36, df=1, p<0.07). As seen in
Table 2, cocaine use was four times as likely in male victims than in female victims and almost twice as likely in African American victims than in white victims. Relative to ethanol use, the only variables that were significant in the multivariable model were age (log likelihood χ
2=3.93, df=1, p<0.05) and race (log likelihood χ
2=10.07, df=1, p<0.002). White victims were more than twice as likely as black victims to have used ethanol before committing suicide (
Table 2).
Discussion
Several key conclusions can be drawn from this study. The first is that cocaine use preceding suicide occurs overwhelmingly in men between 21 and 50 years of age. African American men in this age range appear to be particularly vulnerable; paradoxically, however, African American male teenagers do not use cocaine immediately before suicide. In contrast to cocaine, alcohol was detected in one-third of all white suicide victims, regardless of gender or age, and in almost 20% of black suicide victims. The final and most important conclusion is that substance use in teenage suicides differs dramatically by the race of the victim. Most African American teenagers (86.7%) did not use ethanol or cocaine immediately before committing suicide. In contrast, 50.0% of white teenagers used one or both before committing suicide.
Cocaine use in the United States peaked in 1985–1986 at almost 6 million users and declined to around 1.5 million by 1992. The rate of cocaine use remained around 1.5–2 million users for all of this decade. The rate of frequent use in 1997 was 682,000 users and has not changed appreciably since 1985. Since the peak years, the rate of casual cocaine use has dropped dramatically, by 70% or more. Cocaine was detected in a substantial number of suicides (14.4%) in the at-risk age group in Fulton County, albeit less than the 21% reported in New York City in 1985, during the peak of the epidemic
(7). This suggests that the suicides are occurring among the frequent, heavy cocaine users.
There was a dramatic change in cocaine use preceding suicide in African American male victims between the teenage and young adult years. Among 14 male teenage African American suicide victims, only one was cocaine positive, but in the next two age brackets (21–50 years), cocaine use preceding suicide jumped up to 23.2% (N=19 of 82). The exact opposite pattern was observed among white suicide victims: the high rate of use among teenagers dropped to only 9.5% (N=14 of 148) among white victims 21–50 years of age. Three age-based cohorts of drug users were identified in New York City: an older heroin injection group that was born between 1945 and 1954, a cocaine/crack cohort that was born between 1955 and 1969, and a marijuana cohort born since 1970
(8). The peak rate of cocaine use preceding suicide in Fulton County among African Americans was seen for subjects in the 36–50-year range, consistent with the cocaine/crack cohort in the New York City study.
Alcohol use preceding suicide followed a very different pattern than cocaine. Fully one-third of white suicide victims used ethanol before committing suicide, whereas about 20% of African American victims had. In the case of alcohol, the use of the intoxicant appears to be much more proximate to the suicidal act, since 21% of all victims met the legal definition of intoxication at the time of their death. Overall, the national rates of current ethanol use for white and African American individuals are 55% and 39%, respectively. The corresponding rates of heavy ethanol are 6% and 4.9%. The rate of ethanol detection at autopsy was closer to the rate of current use than to the rate of heavy use. Clearly, alcoholism is a chronic risk factor for suicide
(2), but ethanol detected at autopsy seems to be defining a larger class than the habitual heavy users. One possibility is that with the loss of judgment and control that accompanies intoxication, subjects are more likely to impulsively commit suicide, regardless of their long-term use pattern.
There were two unexpected observations in the teenage group. The first was the low rate of cocaine use among African American teenagers, given the high rates in the older age groups. The second observation was the overall lower rate of substance use in the African American victims than in the white victims. African American male subjects were the largest subgroup of teenage victims but had only two substance-positive suicides, whereas one-half of the white teenagers were substance positive. Data from the “Monitoring the Future” program indicate that 70% of African American teenagers have used ethanol by the 12th grade and 2% have used cocaine
(9). The National Household Survey on Drug Abuse reports the past-month rates of ethanol use among those aged 12–20 years as 32.1% among white and 21.1% among black individuals. The low rate of cocaine detection at autopsy among the black teenagers may reflect low overall use in the community, but the rate of ethanol detection appears to be much lower than the level of ethanol use by black teenagers. The causes of the higher rate of suicide among male African American teenagers remain obscure
(4,
10,
11), but the results of this study suggest that intoxicant use is not a significant proximate cause of suicide in black teenagers. A very different conclusion can be drawn for white teenagers. In this group there is a very high rate of substance use. Substance use, in particular ethanol, is clearly a major risk factor for suicide in white teenagers.