Suicide is the fifth leading cause of years of potential life lost before age 75
(1) and the 11th leading cause of death
(2) in the United States. Historically, whites have had higher suicide rates than blacks, but between 1980 and 1995 the overall rate in blacks increased, driven by a dramatic increase among male adolescents and young adult men
(3). Yet suicide among blacks remains poorly understood. Eight published case-control studies of suicide in the United States conducted since 1985
(4–
11) have yielded data for only 97 blacks, and only a handful of prospective studies examining suicidal behavior and its correlates have reported data stratified by race
(12–
14). It is difficult, therefore, to draw meaningful conclusions about factors relevant to suicide in blacks, and the formulation and implementation of suicide prevention programs targeting at-risk blacks have been compromised.
Postmortem, case-control studies of predominantly white samples have established that antisocial behavior
(7,
9,
15), substance use/abuse
(15–
17), mood disorders
(15–
18), and nonaffective psychotic disorders
(15,
16,
18) confer risk for suicide. Only Kung and associates
(19) attempted to identify race differences in risk factors. Using the 1986 National Mortality Followback Survey data set, Kung and colleagues reported that use of mental health services conferred risk for suicide in both blacks and whites. Whites who had at least a high school education, lived alone, and held blue-collar jobs were at greater risk; these demographic variables did not distinguish suicides in blacks. Heavy drinking was associated with suicide in whites, but not in blacks. Only 25 suicides in blacks were included in the 1986 National Mortality Followback Survey, so the nil findings for demographics and drinking could be ascribed to the small sample size.
The 1993 National Mortality Followback Survey oversampled black decedents and yielded a sample of 150 suicides in blacks. We used that data set to determine if antisocial behavior, substance use/abuse, depressive symptoms, and psychotic symptoms amplified risk among blacks. We also investigated whether there were race differences in risk factors for suicide.
Method
The 1993 National Mortality Followback Survey
(20) was conducted by the National Center for Health Statistics of the Centers for Disease Control and Prevention. The National Mortality Followback Survey is a multicomponent survey that examined a nationally representative sample of individuals age 15 years and older who were residing in and died in the United States in 1993, excluding South Dakota. A sample of 22,957 death certificates was drawn for the 1993 Current Mortality Sample. This subgroup is a 10% systematic sampling of death certificates received at the National Center for Health Statistics from state vital statistics offices. Death certificates do not provide data on situational (e.g., place of death) parameters surrounding the death. The 1993 National Mortality Followback Survey oversampled deaths due to homicide, suicide, and unintentional injury. Next of kin, identified on the death certificate, were contacted and asked to participate in the survey. Respondents were asked to provide information by telephone on the decedent’s background characteristics, lifestyle, health, and type of care received in the last year of life. Interviewers provided no clarification or operational definitions. The directions were as follows: “Now I’m going to read a list of behaviors. Please tell me how frequently (name of decedent) engaged in these behaviors during the last year of life. We would like to know if (name of decedent) engaged in the behavior often, sometimes, rarely, or never.”
For our analysis, suicide decedents (N=1,488; 157 blacks and 1,331 whites) were compared with fatal accident decedents (N=4,395; 783 blacks and 3,612 whites). The latter included decedents of motor vehicle accidents (drivers, passengers, motorcycle operators, pedestrians), poisoning, falls, and other accidents (e.g., drowning, choking). The dependent variable was cause of death, suicide or accident. The use of an accident victim comparison group allows for control of sudden death and the subsequent bereavement
(21), acknowledging that there may be differences in grief response after different causes of death. Misclassification of suicides by drivers as accidents is infrequent and has a negligible influence on suicide statistics
(22,
23).
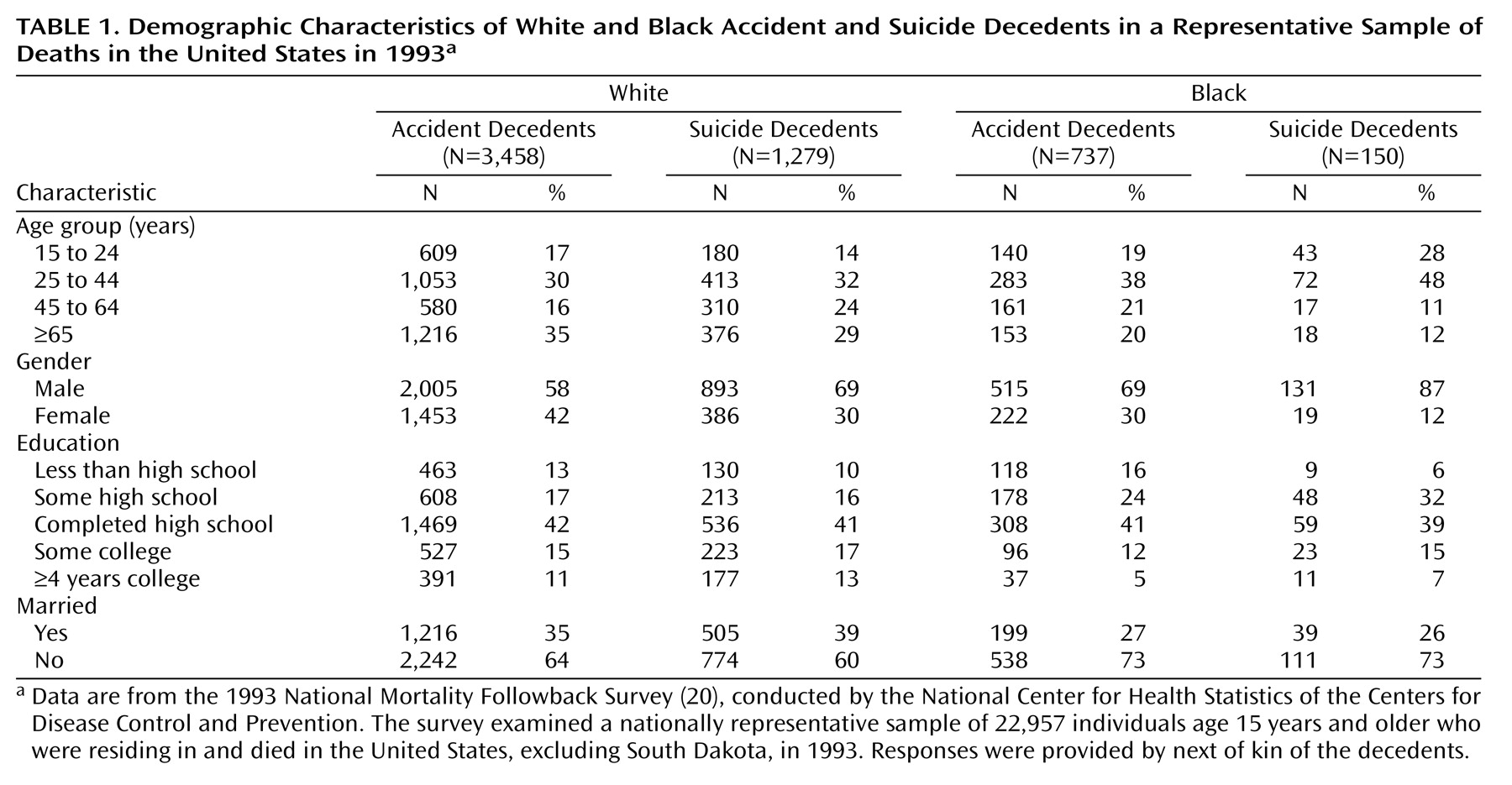
We restricted the sample to white and black non-Hispanics. There were 4,943 white and 940 black accident and suicide decedents. Records for 206 (4.2%) whites and 53 (5.6%) blacks were excluded from the analysis because of missing data for one or more of the following covariates: education, marital status, age, or gender. As for gender, among suicides decedents in the National Mortality Followback Survey, the male-female ratio was 6.9:1 for blacks and 2.3:1 for whites. Demographic information is presented in
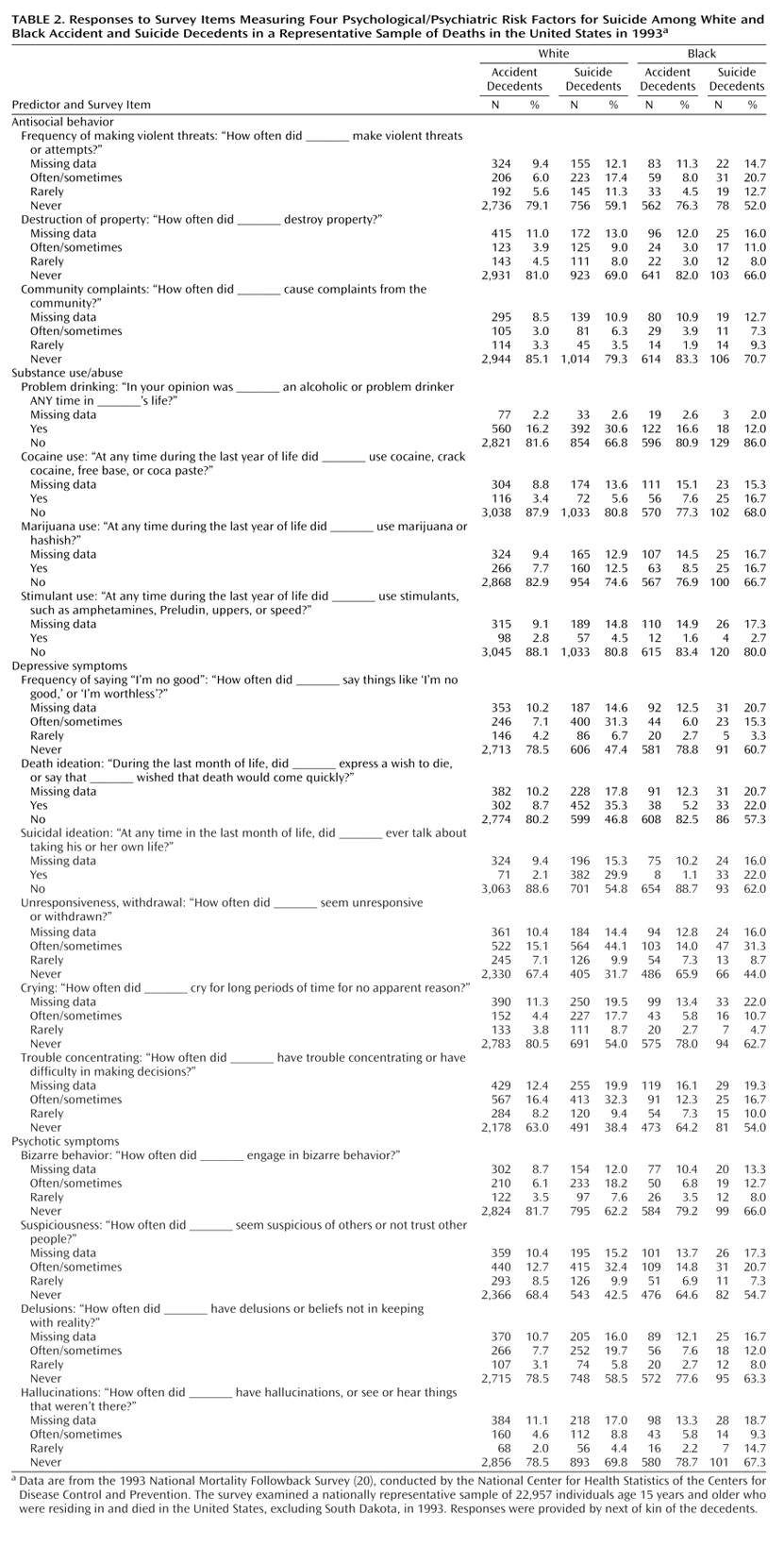
Table 1. Predictors were grouped into four domains: antisocial behavior, substance use/abuse, depressive symptoms, and psychotic symptoms. The items composing these domains are presented in
Table 2.
All statistical analyses were conducted with SUDAAN software
(24). SUDAAN uses Taylor series approximation methods to compute variances that allow adjustment for the multistage cluster sampling strategy. Weights were used to adjust for survey oversampling and nonresponse to yield population estimates of suicide. The SUDAAN LOGISTIC procedure uses generalized estimating equation techniques to fit generalized linear models to binary outcomes. All models were adjusted for gender, age group (see
Table 1 for breakdown), education, and marital status.
Differences between blacks and whites were examined in a two-step process. First, separate regression analyses were conducted for blacks and whites. Eighteen predictors in four domains (antisocial behavior, substance use/abuse, depressive symptoms, and psychotic symptoms) were tested in separate models containing the baseline covariates. Second, to test whether there were significant differences, models for the overall sample that included an interaction term for race and the individual predictors were run, and the significance of the interaction was tested. Preliminary analyses showed a significant three-way interaction between race, gender, and age group. Therefore, the race-stratified analyses included a term for the interaction of gender and age group, and the analyses that combined data for blacks and whites included a three-way interaction of race, gender, and age group. To guard against type I error, a Bonferroni adjustment was used to set the significance level at 0.003.
Discussion
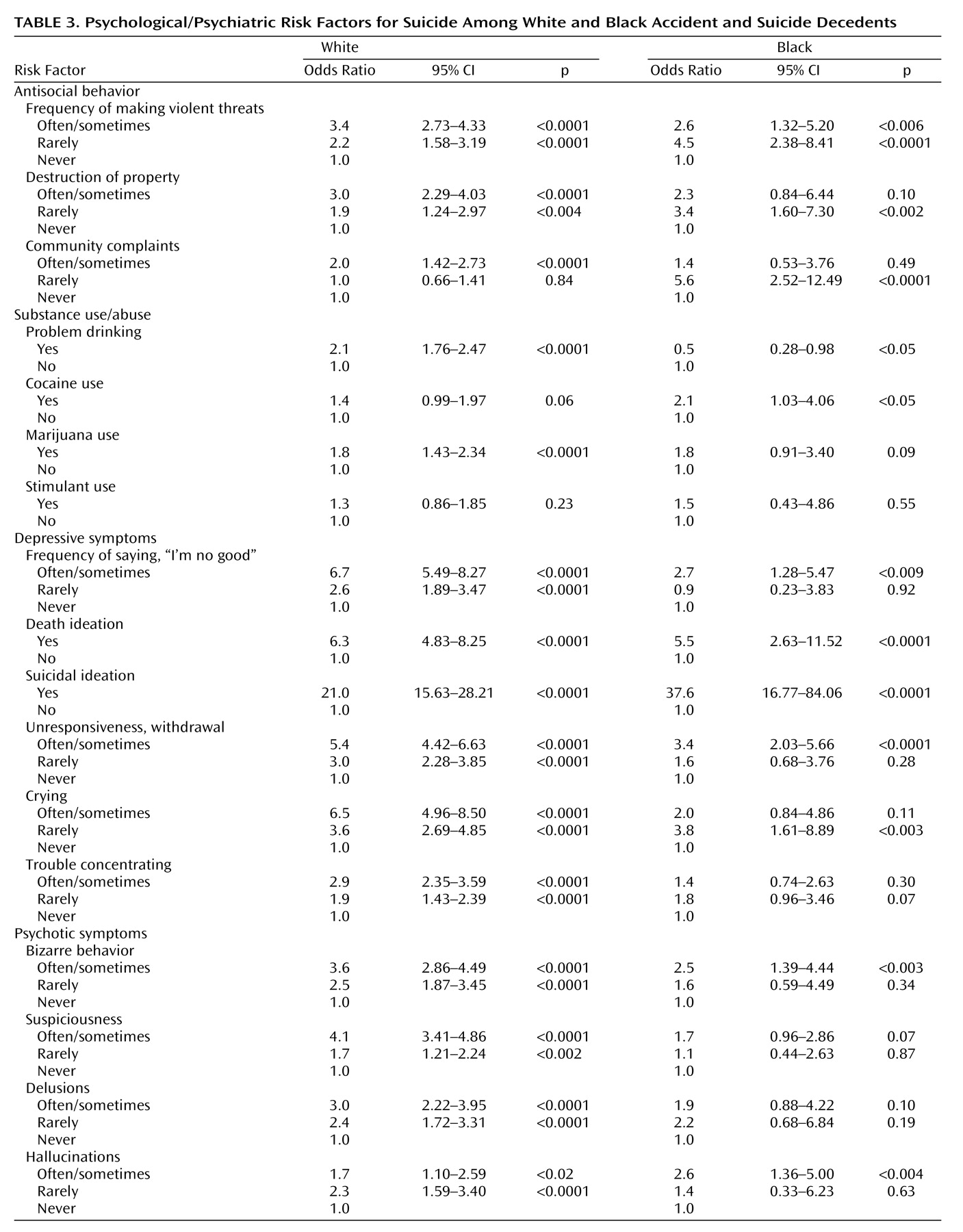
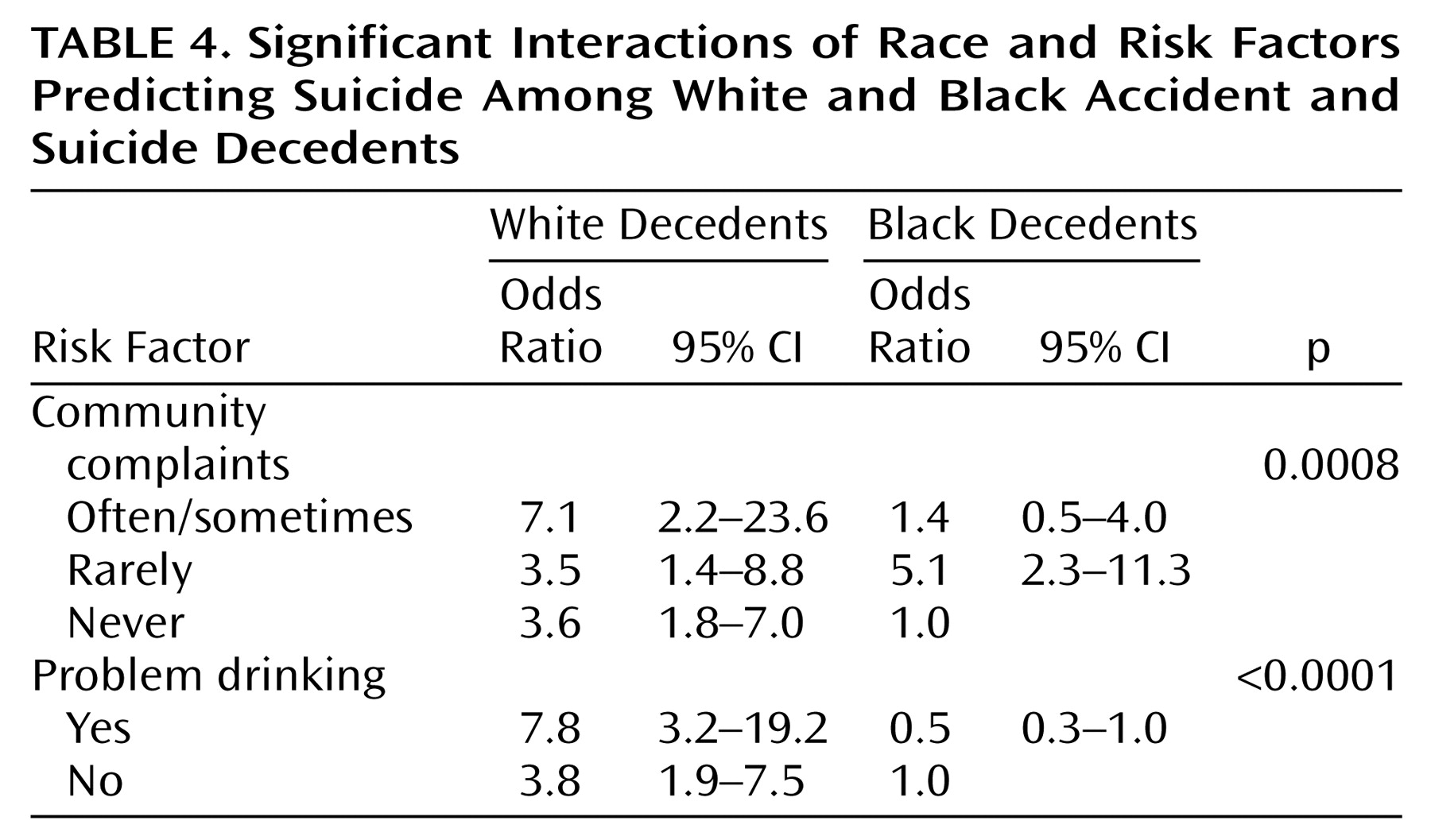
The 1993 National Mortality Followback Survey provided an unprecedented opportunity to identify risk factors for suicide in blacks and to examine potential race differences in suicide. A number of risk factors for suicide were common to both blacks and whites: withdrawn behavior, death ideation, suicidal ideation, and bizarre behavior. There are important differences, however. Whites who died by suicide were more likely to be problem drinkers, a finding that dovetails with the large literature on suicide and substance abuse
(25,
26), and prior data on race differences in suicide risk factors
(19). As well, the straightforward linear relationship between antisocial behavior (violent threats, destruction of property, community complaints) and suicide in whites was consistent with studies of predominantly white samples showing that violent behavior
(27–
29), antisocial behavior
(30), and disruptive disorders
(30,
31) confer risk for suicide and suicide attempts. However, our data suggest that the association between antisocial behavior and suicide in blacks warrants further empirical scrutiny. Whites who generated “frequent” community complaints, a proxy indicator for antisocial behavior, were at increased risk of suicide by more than sevenfold. For blacks, the association between community complaints and suicide was nonlinear. A low or high level of complaints did not confer risk, but a moderate level did (odds ratio=5.6). This finding may be ascribed to race differences in reporting of community complaints, but similar nonlinear patterns were found for destruction of property and making violent threats. Juon and Ensminger
(32) found somewhat similar results.
There were some limitations to the current study. First, the 1993 National Mortality Followback survey, a secondary data set, was used in this study. Consequently, additional information that may have been obtained from practitioners was not available. Second, data collection relied on a phone interview with a proxy respondent. Third, the measures that were used to construct the various domains were brief. In addition, items in the questionnaire that inquired about participation in mental health services in the last year of life and history of emotional/mental health problems were dichotomous. More detailed information about mental health service utilization and mental health history was not available. Fourth, the smaller number of suicides in blacks (N=150) relative to whites (N=1,279) limits statistical power to a greater degree in blacks. These limitations are offset by the uniqueness of the data set, which offered an unprecedented opportunity to examine suicide in blacks and to include a comparison group of accident decedents.
In summary, depressive symptoms amplify suicide risk in blacks and whites, but there may be important race differences in the contributions to suicide risk of antisocial behavior and substance use/abuse. The current study underscores the need for examination of race differences in the relationship between antisocial behavior and suicide. It will also be essential to examine other variables that were unavailable in the National Mortality Followback Survey data set, particularly racism, perceived discrimination, and feelings of alienation from the dominant culture
(33–
36). Research on the interplay of these culturally relevant variables and established psychiatric risk factors may be warranted.