Suicide has proven to be a persistent public health problem, accounting for 30,000 deaths per year in the United States, and the rate has not varied appreciably over the past three decades. The availability of effective treatments for mental illnesses has not altered the population rates of suicide, although this lack of change may be due in part to undertreatment
(1,
2). Suicide risk is not equal across individuals in the population, as the rates in different ethnic and demographic groups and geographic regions vary considerably. In particular, the rate of suicide is lower in blacks than whites
(3). This difference may be due to the interplay of risk and protective factors that are differentially expressed and experienced by different demographic and cultural groups. The known risk and protective factors are psychiatric, socioeconomic, demographic, cultural, and biological in nature.
Suicidal ideation is part of the diagnostic description of major depression (DSM-IV), but completed suicide is not limited to people with this disorder
(4–
6). The persistence of suicide as an adverse outcome of mental illness, despite effective treatments, and the variation in rates between different demographic and ethnic groups suggest that suicide results from some inherent vulnerability diathesis, independent of specific psychiatric disorders or symptoms
(7). There may be subpopulations of individuals that are constitutionally much more vulnerable or resistant to suicide. A psychiatric disorder or high level of psychic distress in combination with high suicide vulnerability may result in a dramatically increased risk of death by suicide. Likewise, robust expression of protective and resilience factors may mitigate otherwise overwhelming levels of distress
(8).
Fulton County, Ga., contains virtually the entire city of Atlanta, with a population of more than 800,000. The population is divided almost equally in half along ethnic lines, with 44.6% African American, 48.1% white, 5.9% Hispanic, and 1.4% other races. Fulton County has a professional medical examiner’s office (as opposed to an elected coroner), staffed by forensic pathologists. Death investigations and autopsies are carried out with standard operating procedures, applied uniformly to each case, and all suspected suicides receive full autopsies. The consequence is that the cause of death (natural, accidental, suicide, or homicide) is determined consistently and with a high degree of certainty. In comparison, the national data set contains the reported cause of death, which may or may not have resulted from an autopsy, so there is much less detail for each case. The large number of cases in the national set (approximately 30,000/year) counterbalances the lack of detail and precision of the cause of death determinations. We compared the results from the local, high-resolution set to the large, low-detail national set to address whether the findings in the local data generalize to the larger population or are unique to Fulton County. Because there appeared to be no difference in the rates of mood disorders or in the ages at onset of mood disorders between blacks and whites and because race is considered to be a social construct, with little explanatory power in defining medical outcomes, the hypothesis for this study was that the patterns of suicide across the life cycle would essentially be identical in the two ethnic groups
(9,
10).
Method
The death investigation and autopsy records for all suicides declared by the Fulton County Medical Examiner from Jan. 1, 1994, through Dec. 31, 2002, were included. An experienced emergency psychiatrist (S.J.G. or D.P.) and a forensic pathologist (M.H.) examined these records and extracted information from them. The extracted information included age, sex, race, method of suicide, medical findings at autopsy, toxicology results, interval from self-inflicted wound to death, level of decomposition if present, and location of incident for each suicide victim. The information was entered into a computerized database. National suicide data for 1999 and 2000 were obtained from the National Center for Injury Prevention, through the Web-Based Injury Statistics Query and Reporting System (http://www.cdc.gov/ncipc/wisqars/default.htm)
(11). Demographic information for Fulton County and the United States was obtained from the U.S Census Bureau (http://quickfacts. census.gov/qfd/states/13/13121.html).
All statistical analyses were performed by means of the JMP 5 statistical package
(12), implemented on Macintosh G-4 computers. Contingency analysis of two-by-two tables was with two-tailed Fisher’s exact statistic. Continuous variables were analyzed with one-way analysis of variance, with post hoc pairwise comparisons of means by Tukey-Kramer honestly significant difference calculations
(13–
15). The distribution of ages was analyzed with the Kaplan-Meier product-limit analysis as implemented by JMP, and significance was determined with both log-rank and Wilcoxon chi-squares. This method allowed comparison of the age distribution curves in different demographic groups but was not denominated by a larger population or at-risk group, so no values were right-censored.
All of the data gathering and analytic procedures were reviewed and approved by the Emory University institutional review board. As this study involved public records and materials gathered in the course of routine public investigations, specific individual informed consent was not necessary.
Results
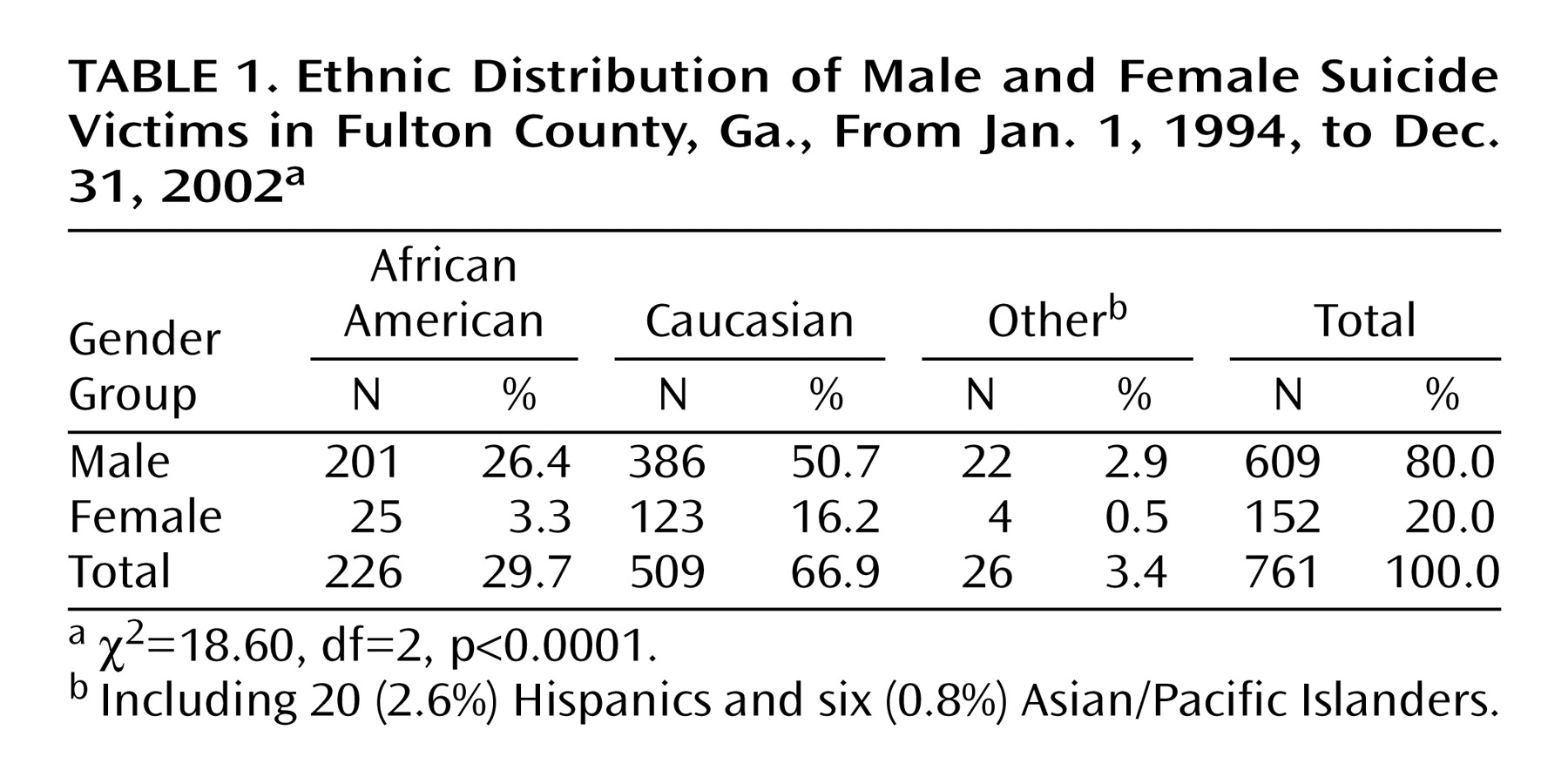
There were 761 suicides in Fulton County during the study interval, and the demographic characteristics of the victims are presented in
Table 1. Only 26 (3.4%) of the victims were nonwhite, nonblack minorities (Hispanic or Asian/Pacific Islander), and the main focus of the rest of the analysis was on the differences between blacks and whites. The group-specific population rates for suicides in Fulton County were 1.22 per 100,000 for black females, 10.74 per 100,000 for black males, 9.89 per 100,000 for white females, and 21.04 per 100,000 for white males. The dominant method of suicide was gunshot, with 455 victims (59.8%), followed by 107 victims who died by hanging (14.1%), 80 by overdose of medications (10.5%), 38 by carbon monoxide intoxication (5.0%), 33 by jumping from heights (4.3%), 11 by asphyxia (1.4%), 13 by cutting or stabbing (1.7%), 10 by blunt-force injuries (1.3%), eight by immolation (1.1%), and six by chemical poisoning (0.8%). The distribution of suicide methods in Fulton County is similar to that in the national data.
The age range of the Fulton County suicide victims was 13 to 99 years, with a mean age of 42.9 (SD=18.5, median=39). The mean ages of the ethnic groups differed, with blacks (mean=36.1 years, SD=17.0) and minorities of other races (mean=35.7, SD=14.3) being significantly younger than whites (mean=46.2, SD=18.5) (F=27.35, df=2, 757, p<0.0001). The demographic groups had distinctly different age distributions: females of “other” race were the youngest, with a mean age of 31.8 years (SD=13.4), followed by African American females at 34.3 (SD=13.4), African American males at 36.3 (SD=17.4), males of “other” races at 36.5 (SD=14.7), white males at 46.1 (SD=18.6), and white females, the oldest, at 46.7 (SD=18.1) (F=11.03, df=5, 754, p<0.0001). Comparison of the mean ages by the Tukey-Kramer honestly significant difference method (q*=2.86, p=0.05) revealed that the mean ages of both the African American females and males were significantly lower than those of the white females and males, respectively, while within each ethnic group the ages did not vary significantly by gender.
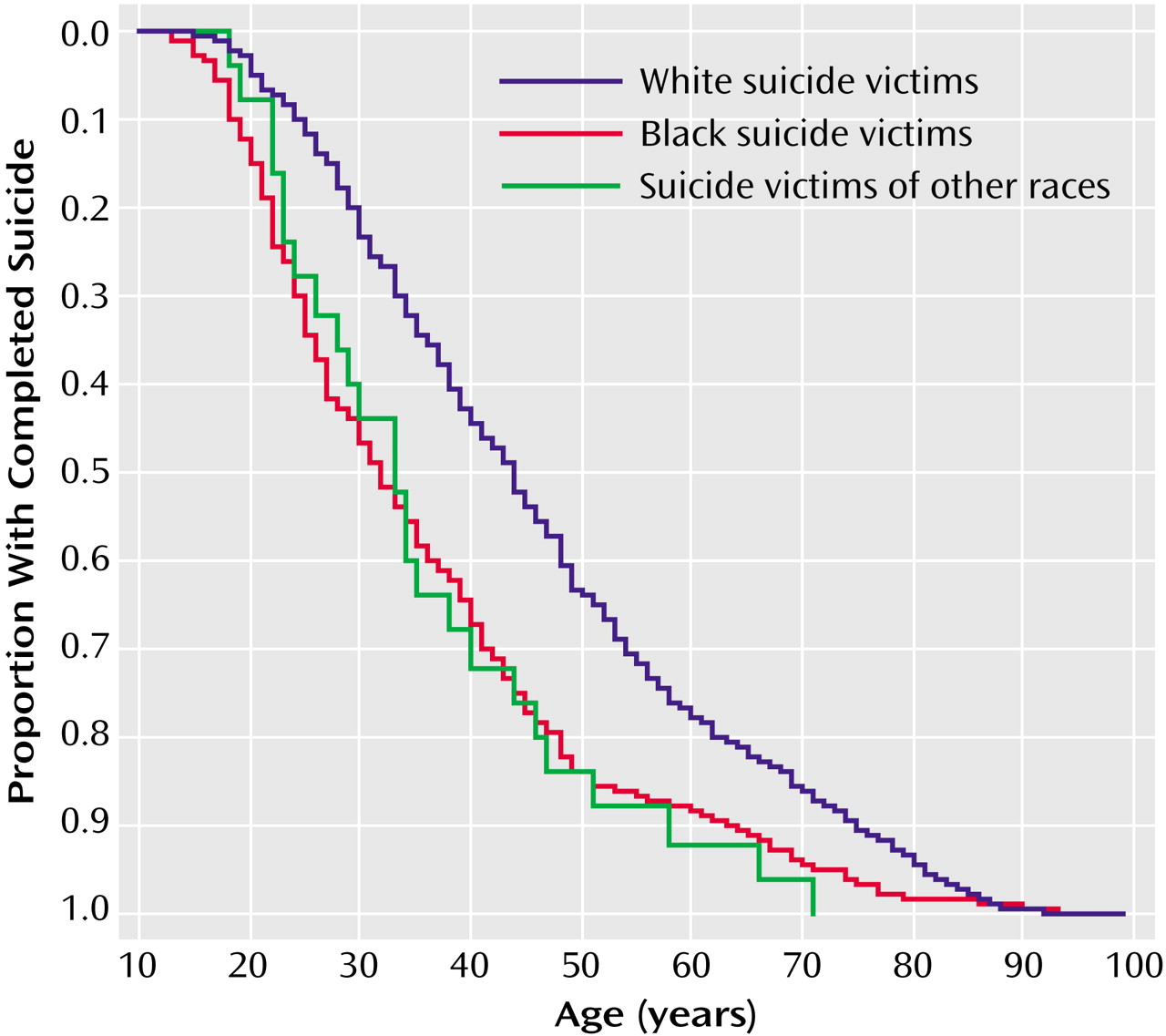
Comparison of the ages of the male and female suicide victims in Fulton County by means of Kaplan-Meier analysis revealed no significant differences between genders; the median age of the females was 42 years, with an interquartile range (IQR) of 30–54, and the median for males was 39 years (IQR=27–54). African Americans committed suicide on average more than a full decade earlier than did whites, and they did so in a narrow age window (
Figure 1). Within each ethnic group, the median age and interquartile range did not differ by gender, as the black females (median=32, IQR=25–42) overlapped the black males (median=32, IQR=23–45), but those values did differ substantially from those for white females (median=44, IQR=32–59) and white males (median=44, IQR=31–58) (χ
2=63.81, df=3, p<0.0001). The African American females had the narrowest age distribution, with the vast majority clustering between the early 20s and mid 40s, only two below 20, and only one above the age of 48.
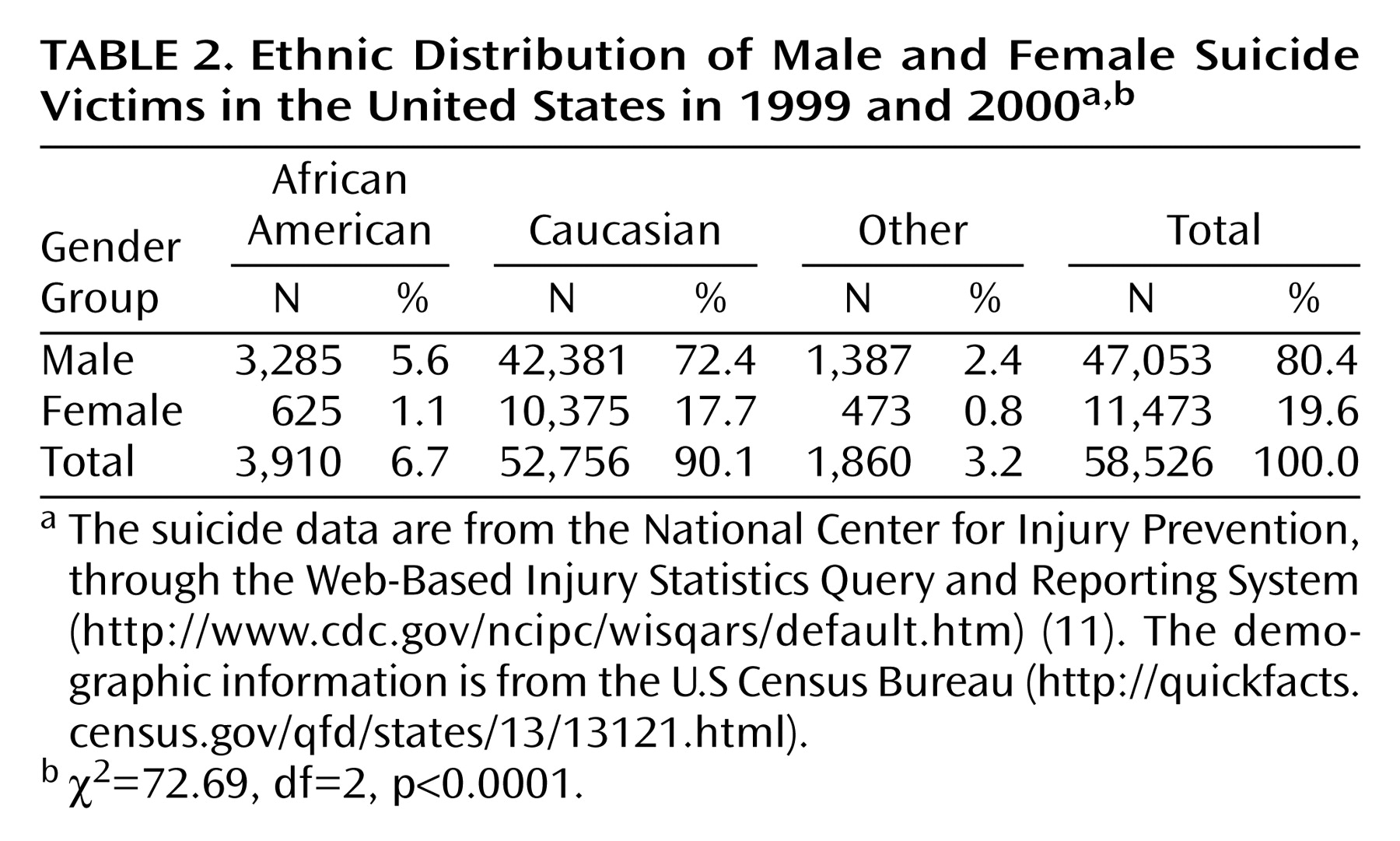
The national suicide statistics were similar to those from Fulton County, although Caucasians accounted for a much larger share of the total. There were 58,526 suicides in the United States in 1999 and 2000 combined (
Table 2). The mean age of the white victims was 46.2 years (SD=18.8), for blacks it was 36.8 (SD=16.1), and for victims of other races it was 38.4 (SD=17.3) (F=603.03, df=2, 585253, p<0.001), and within each group there was no age difference by gender. The mean ages for all males (45.5 years, SD=19.1) and females (45.6 years, SD=17.1) in the national set were indistinguishable from each other. The median age of African American victims was 34 years (IQR=24–45), for “other” ethnic groups it was 35 years (IQR=25–49), and for Caucasians it was 44 (IQR=32–58) (χ
2=1330.99, df=2, p<0.0001).
Discussion
The population of Fulton County, Ga., is divided in half along ethnic lines, but the numbers and rates of death by suicide differ substantially between African Americans and whites. African Americans commit suicide much less frequently than whites, but they do so at much earlier ages. African American females are remarkably resistant to suicide compared to other demographic groups, accounting for only 3.3% of all victims in Fulton County and 1.1% nationally. There were five times as many suicides by white females as by black females in Fulton County. This result is consistent with a recent report by Runyan et al.
(3). They reported that white females commit suicide at three times the rate of black females. The window of vulnerability for African American females is particularly narrow, with the vast majority occurring between ages 20 and 45 and virtually none above or below this age range. The median age of white female suicide victims was higher than the 75th percentile for the black females. The female population of Fulton County is divided almost equally in half between blacks (N=163,713) and whites (N=171,810), and above the age of 45 years, 45.3% of the female population is black (N=57,298) and 54.7% is white (N=69,067). So the difference in the numbers of suicides above the age of 45 between black and white females does not appear to be due to a difference in overall population distribution.
Comparison of the findings for Fulton County to the national data suggests that the results observed in Fulton County reflect national trends. The race-specific suicide rates in Fulton County were 5.6 per 100,000 for blacks and 15.5 per 100,000 for whites, and nationally the rates were 5.6 per 100,000 for blacks, 12.5 per 100,000 for whites, and 2.0 per 100,000 for other ethnic groups. Overall, the group consisting of Hispanics, Asian/Pacific Islanders, and other ethnicities had the lowest population-specific suicide rate, both nationally and in Fulton County. Likewise, the Fulton County and national age distribution results were essentially identical to each other, indicating that the difference between ethnic groups in age at suicide in the local data set is an accurate representation of the national pattern.
Differential patterns of substance abuse among the younger suicide victims do not appear to account for the lower age at suicide of African Americans. Previously we reported that rates of ethanol and cocaine use preceding suicide differed by demographic group, with a larger proportion of whites than blacks having used alcohol before death and more blacks having used cocaine
(16). Within each ethnic group, the two genders were essentially identical in rates of presuicide alcohol or cocaine use. But despite these different patterns of substance use, more than 60% of all suicide victims had not used either intoxicant before death. In Fulton County, African Americans constituted the largest group of victims age 20 and below, but only 14.8% tested positive for alcohol or cocaine at autopsy, compared to 50.0% of white teenage suicide victims testing positive. The same pattern persisted in the 21–40-year-old age group, with 50.2% of white victims testing positive for an intoxicant, compared to 41.4% of blacks.
Despite the evidence that race defined as African American or Caucasian has little medical relevance, there was a dramatic difference in the occurrence of suicide between the two groups. The influence of race on age at suicide is more prominent than gender, as the age distribution of white males was superimposed on that of white females and likewise for African Americans. In both genders, African Americans committed suicide at much earlier ages than whites. Rates of affective and other psychiatric disorders have been reported to be similar in blacks and whites and to have similar clinical manifestations and ages at onset
(10,
17,
18). There are some differences between African Americans and whites in types of depressive symptoms reported, with blacks reporting more somatic complaints and more sleep and appetitive disturbances, while both groups report equally severe cognitive disturbance, anxiety, and core depressive feelings.
A disparity in the availability of mental health treatment resources has been reported in the United States, and African Americans have more limited access to treatment than whites
(19). African Americans have a greater unmet need for mental health and substance abuse treatment and receive care that is of lower quality than that provided to whites
(20–
22). In particular, African Americans residing in the southern United States have a higher likelihood of receiving psychiatric care that is not minimally adequate. African Americans have an ambivalent attitude toward psychiatric treatment, as blacks have been reported to find treatment with antidepressants less acceptable than do other groups and to have higher rates of attrition from psycho- and pharmacotherapy
(23). If suicide is considered to be an adverse outcome of untreated or inadequately treated psychiatric illness, then African Americans should be at greater risk than are Caucasians, but these data refute this conclusion.
The stress-diathesis hypothesis of suicide posits a state-dependent trigger domain, driven by depression and other psychiatric disorders in combination with psychosocial stressors, and a trait-dependent threshold domain
(7). Risk in both the trigger and threshold domains could be dramatically modified by the expression of protective and resilience factors
(8). While suicide risk factors include psychopathology, socioeconomic conditions, and psychosocial stressors, protective factors have been described more in cultural, religious, and familial domains.
Among African Americans, cultural factors have been proposed as buffers against suicide
(24–
27). Principal among these are religiosity, family support, and a community-held attitude that suicide is unacceptable
(28). Orthodox religious beliefs and devotion have been shown to be highly protective against suicide among African Americans
(29). Other cultural attributes that mitigate suicide risk among blacks are family cohesion and support and a tendency to seek support from friends and family
(24,
30). Seeking professional mental health care is correlated to increased suicidality among African Americans
(31). In the case of older black women, these protective factors may be particularly robust, dramatically diminishing the impact of trigger-domain risk factors such as major depression, socioeconomic conditions, and psychosocial stressors. In comparison, diminished expression of protective and resilience factors in whites with advancing age could account for the observation that completed suicide occurs more frequently in whites past the teenage years, especially among older white men. It is interesting that there appears to be no difference in the attitudes about suicide between older blacks and whites, with both groups reporting low levels of agreement with or empathy toward suicidal acts
(32).
A possible limitation of the Fulton County data is that specific psychiatric diagnoses, psychological autopsies, or case histories were not available. A countervailing strength is that professional forensic pathologists staff the Medical Examiner’s Office, so all of the included cases were investigated and analyzed with the same set of operational procedures and conventions. All suspicious deaths are investigated and receive a full autopsy, so that there is consistency and a high degree of certainty in assignments of cause of death. Comparison of the Fulton County and national data reveals that the local data largely mirror the national set, so conclusions from Fulton County may be generally applicable. The most significant weakness of the national data set is that it contains the reported cause of death. Cause of death is not assigned uniformly across the nation, and in many localities autopsies are not performed on all potential suicide victims. The consequence is that little detail is available for each case. The large number of cases included in the national set compensates for the lack of detail of any individual case. One limitation of the statistical analysis is in the use of the Kaplan-Meier calculation to define the age-at-death curves. This was done to compare the distributions of ages in the different demographic groups, so all cases were included and there were no cases censored for competing causes of death. As this was not a prospective study of a larger at-risk group, this analysis allows for conclusions only about the set of observed cases.
In conclusion, we have shown that there is a distinct difference in the patterns of suicide across the life cycle of African Americans and Caucasians. Many fewer blacks commit suicide than whites, but they do so much earlier in life. The age at completed suicide for blacks is more than a decade lower than that for whites. This has definite implications for understanding potential causes of suicide and for developing suicide prevention plans tailored to the needs of specific communities.