An Empirically Derived Taxonomy for Personality Diagnosis: Bridging Science and Practice in Conceptualizing Personality
Abstract
Objective:
Method:
Results:
Conclusions:
Describing Personality Syndromes
Assigning Diagnoses in Day-to-Day Practice
Method
Measures
The Shedler-Westen Assessment Procedure–II (SWAP-II).
Clinical data form.
Axis II criterion checklist.
Data Analysis
Results
Deriving Diagnostic Prototypes
| Personality Spectrum and Diagnosis | Number of Items | Cronbach's Alpha |
|---|---|---|
| Internalizing | 20 | 0.85 |
| Depressive | 17 | 0.82 |
| Anxious-avoidant | 15 | 0.78 |
| Dependent-victimized | 16 | 0.78 |
| Schizoid-schizotypal | 19 | 0.77 |
| Externalizing | 21 | 0.87 |
| Antisocial-psychopathic | 18 | 0.89 |
| Narcissistic | 21 | 0.72 |
| Paranoid | 15 | 0.79 |
| Borderline-dysregulated | 24 | 0.81 |
| Neurotic styles | ||
| Obsessional | 21 | 0.73 |
| Hysteric-histrionic | 20 | 0.72 |
| Personality health | 23 | 0.94 |
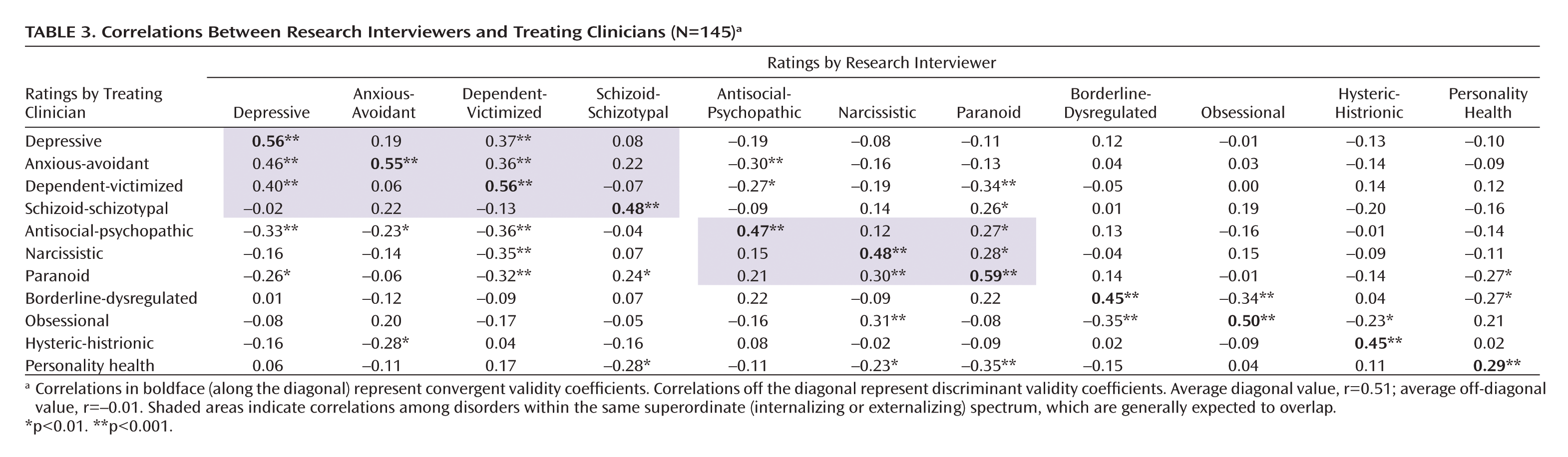
Validity Across Independent Observers and Assessment Methods
Discussion
Continuities and Discontinuities With DSM-IV
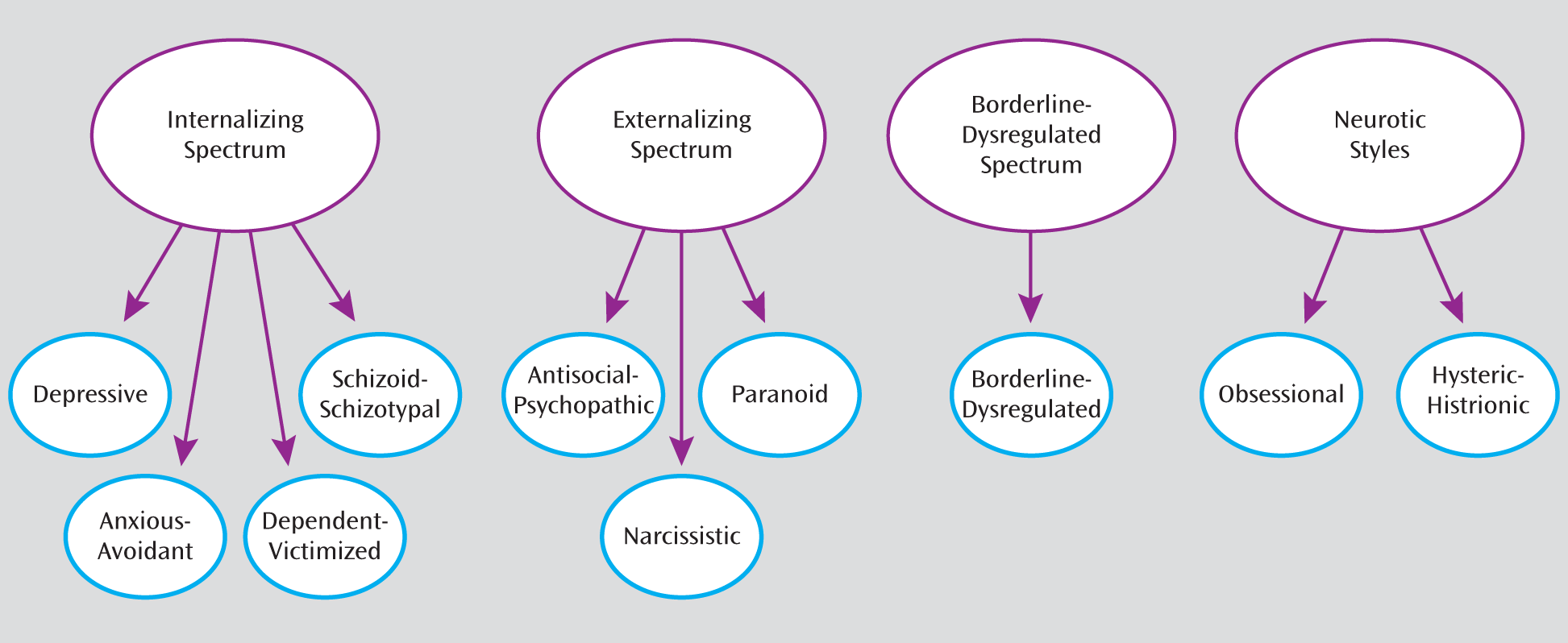
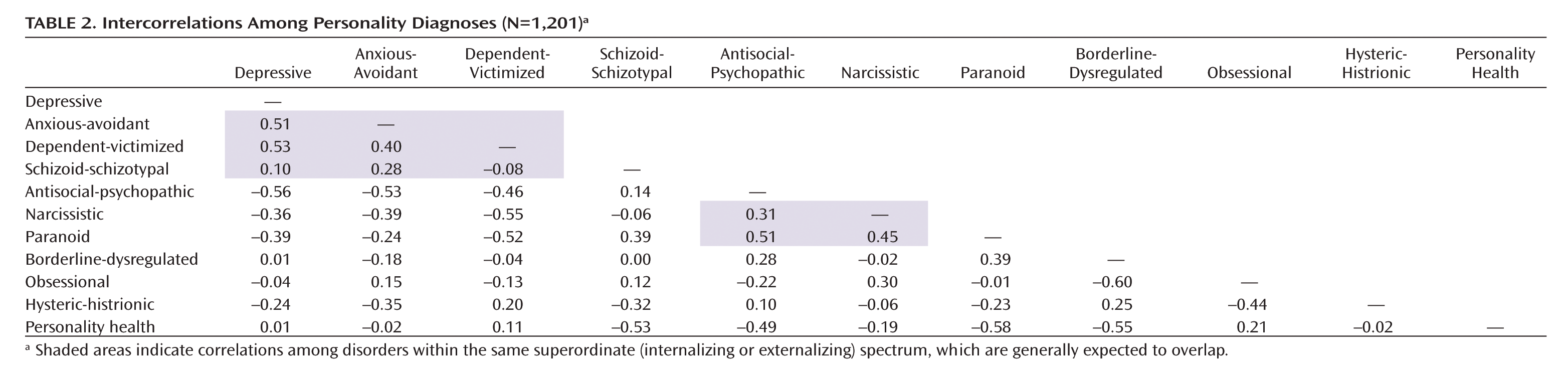
Hierarchical Organization of Personality Syndromes
Personality Health Prototype
Conclusions
Footnote
APPENDIX. Empirically Derived Prototypes for Personality Disorder Diagnosis Based on the Shedler-Westen Assessment Procedurea
| For each diagnosis, please form an overall impression of the type of person described, then rate the extent to which your patient matches or resembles the prototype. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 5 | Very good match (patient exemplifies this disorder; prototypical case) | Diagnosis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 4 | Good match (patient has this disorder; diagnosis applies) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 3 | Moderate match (patient has significant features of this disorder) | Features | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2 | Slight match (patient has minor features of this disorder) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1 | No match (description does not apply) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Internalizing Spectrum |
| The internalizing spectrum subsumes four personality disorders: Depressive, Anxious-Avoidant, Dependent-Victimized, and Schizoid-Schizotypal. Individuals with disorders in the internalizing spectrum experience chronic painful emotions, especially depression and anxiety, tend to be emotionally inhibited and socially avoidant, and tend to blame themselves for their difficulties. |
| Individuals with disorders in the internalizing spectrum are chronically susceptible to a range of painful emotions, including depression, anxiety, guilt, shame, and embarrassment. They tend to be self-critical and to feel inadequate. They tend to be inhibited and constricted and have difficulty allowing themselves to express their wishes and impulses. They tend to be passive and unassertive, and to feel helpless, powerless, or at the mercy of forces outside their control. They tend to ruminate over problems. They have trouble acknowledging or expressing anger and instead become depressed, self-critical, or self-punitive (turning their anger on themselves rather than getting angry at others). They often fear rejection or abandonment and may suffer from painful feelings of emptiness. They tend to be shy or self-conscious and may avoid social situations because of fear of embarrassment. They tend to feel like outcasts or outsiders and may lack close friendships and relationships. |
| Depressive Personality |
| Summary statement: Individuals with Depressive Personality are prone to feelings of depression and inadequacy, tend to be self-critical or self-punitive, and may be preoccupied with concerns about abandonment or loss. |
| Individuals who match this prototype tend to feel depressed or despondent and to feel inadequate, inferior, or a failure. They tend to find little pleasure or satisfaction in life's activities and to feel life has no meaning. They are insufficiently concerned with meeting their own needs, disavowing or squelching their hopes and desires to protect against disappointment. They appear conflicted about experiencing pleasure, inhibiting feelings of excitement, joy, or pride. They may likewise be conflicted or inhibited about achievement or success (e.g., failing to reach their potential or sabotaging themselves when success is at hand). Individuals who match this prototype are generally self-critical, holding themselves to unrealistic standards and feeling guilty and blaming themselves for bad things that happen. They appear to want to “punish” themselves by creating situations that lead to unhappiness or avoiding opportunities for pleasure and gratification. They have trouble acknowledging or expressing anger and instead become depressed, self-critical, or self-punitive. Individuals who match this prototype often fear that they will be rejected or abandoned, are prone to painful feeling of emptiness, and may feel bereft or abjectly alone even in the presence of others. They may have a pervasive sense that someone or something necessary for happiness has been lost forever (e.g., a relationship, youth, beauty, success). |
| Anxious-Avoidant Personality |
| Summary statement: Individuals with Anxious-Avoidant Personality are chronically prone to anxiety, are socially anxious and avoidant, and attempt to manage anxiety in ways that limit and constrict their lives. |
| Individuals who match this prototype are chronically anxious. They tend to ruminate, dwelling on problems or replaying conversations in their minds. They are more concerned with avoiding harm than pursuing desires, and their choices and actions are unduly influenced by efforts to avoid perceived dangers. They are prone to feelings of shame and embarrassment. Individuals who match this prototype tend to be shy and self-conscious in social situations and to feel like an outcast or outsider. They are often socially awkward and tend to avoid social situations because of fear of embarrassment or humiliation. They tend to be inhibited and constricted and to have difficulty acknowledging or expressing desires. They may adhere rigidly to daily routines, have trouble making decisions, or vacillate when faced with choices. Their anxiety may find expression through a variety of channels, including panic attacks, hypochondriacal concerns (e.g., excessive worry about normal aches and pains), or somatic symptoms in response to stress (e.g., headache, backache, abdominal pain, asthma). |
| Dependent-Victimized Personality |
| Summary statement: Individuals with Dependent-Victimized Personality are highly dependent and fearful of being alone, tend to show insufficient concern for their own well-being to the point of jeopardizing their welfare or safety, and have difficulty expressing anger directly. |
| Individuals who match this prototype tend to be needy and dependent, fear being alone, and fear rejection or abandonment. They tend to be ingratiating or submissive, often consenting to things they find objectionable in an effort to maintain support or approval. They tend to be passive and unassertive and to feel helpless and powerless. They tend to be indecisive, suggestible or easily influenced, and naive or innocent, seeming to know less about the ways of the world than would be expected. They tend to become attached to people who are emotionally unavailable, and to create relationships in which they are in the role of caring for or rescuing the other person. Individuals who match this prototype tend to get drawn into or remain in relationships in which they are emotionally or physically abused, or needlessly put themselves in dangerous situations (e.g., walking alone or agreeing to meet strangers in unsafe places). They are insufficiently concerned with meeting their own needs and tend to feel unworthy or undeserving. Individuals who match this prototype have trouble acknowledging or expressing anger and instead become depressed, self-critical, or self-punitive. They tend to express anger in passive and indirect ways (e.g., making mistakes, procrastinating, forgetting) that may provoke or trigger anger or mistreatment from others. |
| Schizoid-Schizotypal Personality |
| Summary statement: Individuals with Schizoid-Schizotypal Personality are characterized by pervasive impoverishment of, and peculiarities in, interpersonal relationships, emotional experience, and thought processes. |
| Individuals who match this prototype lack close relationships and appear to have little need for human company or contact, often seeming detached or indifferent. They lack social skills and tend to be socially awkward or inappropriate. Their appearance or manner may be odd or peculiar (e.g., their grooming, posture, eye contact, or speech rhythms may seem strange or “off”), and their verbal statements may be incongruous with their accompanying emotion or non-verbal behavior. They have difficulty making sense of others' behavior and appear unable to describe important others in a way that conveys a sense of who they are as people. They likewise have little insight into their own motives and behavior, and have difficulty giving a coherent account of their lives. Individuals who match this prototype appear to have a limited or constricted range of emotions and tend to think in concrete terms, showing limited ability to appreciate metaphor, analogy, or nuance. Consequently, they tend to elicit boredom in others. Despite their apparent emotional detachment, they often suffer emotionally: They find little satisfaction or enjoyment in life's activities, tend to feel life has no meaning, and feel like outcasts or outsiders. A subset of individuals who match this prototype show substantial peculiarities in their thinking and perception. Their speech and thought processes may be circumstantial, rambling, or digressive, their reasoning processes or perceptual experiences may seem odd and idiosyncratic, and they may be suspicious of others, reading malevolent intent into others' words and actions. |
| Externalizing Spectrum |
| The externalizing spectrum subsumes three personality disorders: Antisocial-Psychopathic, Paranoid, and Narcissistic. Individuals with disorders in the externalizing spectrum are angry or hostile, self-centered and lacking in empathy, and blame others for their difficulties. |
| Individuals with disorders in the Externalizing spectrum tend to be angry or hostile, whether expressed through overt aggression, rage episodes, or critical, controlling, or oppositional behavior. They tend to be suspicious of others, conflicted about authority, and prone to getting into power struggles. They tend to hold grudges and to react to perceived slights with rage and humiliation. They lack empathy for others' needs and feelings, may feel privileged or entitled, and tend to have an exaggerated sense of self-importance. They tend to blame their failures on other people or circumstances. They have little psychological insight into their own motives and behavior and tend to feel mistreated or victimized rather than recognizing how their own behavior and attitudes affect other people. They tend to elicit dislike or animosity and to lack close friendships and relationships. |
| Antisocial-Psychopathic Personality |
| Summary statement: Individuals with Antisocial-Psychopathic Personality exploit others, experience little remorse for harm or injury caused to others, and have poor impulse control. |
| Individuals who match this prototype take advantage of others, tend to lie or deceive, and to be manipulative. They show a reckless disregard for the rights, property, or safety of others. They lack empathy for other people's needs and feelings. Individuals who match this prototype experience little remorse for harm or injury they cause. They appear impervious to consequences and seem unable or unwilling to modify their behavior in response to threats or consequences. They generally lack psychological insight and blame their difficulties on other people or circumstances. They often appear to gain pleasure by being sadistic or aggressive toward others, and they may attempt to dominate significant others through intimidation or violence. Individuals who match this prototype tend to be impulsive, to seek thrills, novelty, and excitement, and to require high levels of stimulation. They tend to be unreliable and irresponsible and may fail to meet work obligations or honor financial commitments. They may engage in antisocial behavior, including unlawful activities, substance abuse, or interpersonal violence. They may repeatedly convince others of their commitment to change, leading others to think “this time is really different,” only to revert to their previous maladaptive behavior. |
| Paranoid Personality |
| Summary statement: Individuals with Paranoid Personality are chronically suspicious, angry and hostile, and may show disturbed thinking. |
| Individuals who match this prototype are chronically suspicious, expecting that others will harm, deceive, conspire against, or betray them. They tend to blame their problems on other people or circumstances, and to attribute their difficulties to external factors. Rather than recognizing their own role in interpersonal conflicts, they tend to feel misunderstood, mistreated, or victimized. Individuals who match this prototype tend to be angry or hostile and prone to rage episodes. They tend to see their own unacceptable impulses in other people instead of in themselves, and are therefore prone to misattribute hostility to other people. They tend to be controlling, to be oppositional, contrary, or quick to disagree, and to hold grudges. They tend to elicit dislike or animosity and to lack close friendships and relationships. Individuals who match this prototype tend to show disturbances in their thinking, above and beyond paranoid ideas. Their perceptions and reasoning can be odd and idiosyncratic, and they may become irrational when strong emotions are stirred up, to the point of seeming delusional. |
| Narcissistic Personality |
| Summary statement: Individuals with Narcissistic Personality are grandiose and entitled, dismissive and critical of others, and often show underlying signs of vulnerability beneath a grandiose façade. |
| Individuals who match this prototype have an exaggerated sense of self-importance. They feel privileged and entitled, expect preferential treatment, and seek to be the center of attention. They have fantasies of unlimited success, power, beauty, or talent, and tend to treat others primarily as an audience to witness their importance or brilliance. They tend to believe they can only be appreciated by, or should only associate with, people who are high-status, superior, or “special.” They have little empathy and seem unable to understand or respond to others' needs and feelings unless they coincide with their own. Individuals who match this prototype tend to be dismissive, haughty, and arrogant. They tend to be critical, envious, competitive with others, and prone to get into power struggles. They attempt to avoid feeling helpless or depressed by becoming angry instead, and tend to react to perceived slights or criticism with rage and humiliation. Their overt grandiosity may mask underlying vulnerability: Individuals who match this prototype are invested in seeing and portraying themselves as emotionally strong, untroubled, and emotionally in control, often despite clear evidence of underlying insecurity or distress. A substantial subset of narcissistic individuals tend to feel inadequate or inferior, to feel that life has no meaning, and to be self-critical and intolerant of their own human defects, holding themselves to unrealistic standards of perfection. |
| Borderline-Dysregulated Spectrum |
| Borderline-Dysregulated Personality |
| Summary Statement: Individuals with Borderline-Dysregulated Personality have impaired ability to regulate their emotions, have unstable perceptions of self and others that lead to intense and chaotic relationships, and are prone to act on impulses, including self-destructive impulses. |
| Individuals who match this prototype have emotions that can change rapidly and spiral out of control, leading to extremes of sadness, anxiety, and rage. They tend to “catastrophize,” seeing problems as disastrous or unsolvable, and are often unable to soothe or comfort themselves without the help of another person. They tend to become irrational when strong emotions are stirred up, showing a significant decline from their usual level of functioning. Individuals who match this prototype lack a stable sense of self: Their attitudes, values, goals, and feelings about themselves may seem unstable or ever-changing, and they are prone to painful feelings of emptiness. They similarly have difficulty maintaining stable, balanced views of others: When upset, they have trouble perceiving positive and negative qualities in the same person at the same time, seeing others in extreme, black-or-white terms. Consequently, their relationships tend to be unstable, chaotic, and rapidly changing. They fear rejection and abandonment, fear being alone, and tend to become attached quickly and intensely. They are prone to feeling misunderstood, mistreated, or victimized. They often elicit intense emotions in other people and may draw them into roles or “scripts” that feel alien and unfamiliar (e.g., being uncharacteristically cruel, or making “heroic” efforts to rescue them). They may likewise stir up conflict or animosity between other people. Individuals who match this prototype tend to act impulsively. Their work life or living arrangements may be chaotic and unstable. They may act on self-destructive impulses, including self-mutilating behavior, suicidal threats or gestures, and genuine suicidality, especially when an attachment relationship is disrupted or threatened. |
| Neurotic Styles |
| The neurotic styles grouping subsumes two personality syndromes: Obsessional and Hysteric-Histrionic. These syndromes generally do not entail the same level of impairment or dysfunction as the other personality syndromes, and may therefore be considered character styles rather than disorders. Their more extreme variants can, however, constitute bona fide personality disorders. |
| Obsessional Personality |
| Summary statement: Individuals with Obsessional Personality are intellectualized and overly “rational” in their approach to life, are emotionally constricted and rigid, and are critical of themselves and others and conflicted about anger, aggression, and authority. |
| Individuals who match this prototype tend to see themselves as logical and rational, uninfluenced by emotion. They tend to think in abstract and intellectualized terms, to become absorbed in details (often to the point of missing what is important), and prefer to operate as if emotions were irrelevant or inconsequential. They tend to be excessively devoted to work and productivity to the detriment of leisure and relationships. Individuals who match this prototype tend to be inhibited and constricted, and have difficulty acknowledging or expressing wishes, impulses, or anger. They are invested in seeing and portraying themselves as emotionally strong, untroubled, and in control, despite evidence of underlying insecurity, anxiety, or distress. They tend to deny or disavow their need for nurturance or comfort, often regarding such needs as weakness. They tend to adhere rigidly to daily routines, becoming anxious or uncomfortable when they are altered, and to be overly concerned with rules, procedures, order, organization, schedules, and so on. They may be preoccupied with concerns about dirt, cleanliness, or contamination. Rationality and regimentation generally mask underlying feelings of anxiety or anger. Individuals who match this prototype tend to be conflicted about anger, aggression, and authority. They tend to be self-critical, expecting themselves to be “perfect,” and to be equally critical of others, whether overtly or covertly. They tend to be controlling, oppositional, and self-righteous or moralistic. They are prone to being stingy and withholding (e.g., of time, money, affection). They are often conflicted about authority, struggling with contradictory impulses to submit versus defy. |
| Hysteric-Histrionic Personality |
| Summary statement: Individuals with Hysteric-Histrionic Personality are emotionally dramatic and cognitively impressionistic, sexually provocative, and interpersonally suggestible, idealizing of admired others, and paradoxically both intensely and superficially attached. |
| Individuals who match this prototype are emotionally dramatic and prone to express emotion in exaggerated and theatrical ways. Their reactions tend to be based on emotion rather than reflection, and their cognitive style tends to be glib, global, and impressionistic (e.g., missing details, glossing over inconsistencies, mispronouncing names). Their beliefs and expectations seem cliché or stereotypical, as if taken from storybooks or movies, and they seem naive or innocent, seeming to know less about the ways of the world than would be expected. Individuals who match this prototype tend to be sexually seductive or provocative. They use their physical attractiveness to an excessive degree to gain attention and notice, and they behave in ways that seem to epitomize gender stereotypes. They may be flirtatious, preoccupied with sexual conquest, prone to lead people on, or promiscuous. They tend to become involved in romantic or sexual “triangles” and may be drawn to people who are already attached or sought by someone else. They appear to have difficulty directing both tender feelings and sexual feelings toward the same person, tending to view others as either virtuous or sexy, but not both. Individuals who match this prototype tend to be suggestible or easily influenced, and to idealize and identify with admired others to the point of taking on their attitudes or mannerisms. They fantasize about ideal, perfect love, yet tend to choose sexual or romantic partners who are emotionally unavailable, or who seem inappropriate (e.g., in terms of age or social or economic status). They may become attached quickly and intensely. Beneath the surface, they often fear being alone, rejected, or abandoned. |
| Personality Health |
| This prototype represents optimal personality health. Degree of match with this prototype provides a measure of adaptive psychological strengths. The more individuals match this prototype, the more they are able to engage in meaningful and mature relationships, find meaning and satisfaction in life's pursuits, and make effective use of their talents and abilities. |
| Individuals who match this prototype are capable of sustaining meaningful relationships characterized by genuine intimacy and caring. They are empathic and responsive to others' needs and feelings and have the capacity to recognize alternative viewpoints, even when emotions are strong. They have moral and ethical standards, strive to live up to them, and tend to be conscientious and responsible. They appear comfortable in social situations, are able to assert themselves effectively and appropriately when necessary, tend to be energetic and outgoing, and tend to be liked by others. They tend to have satisfying sex lives. They are psychologically insightful and able to understand themselves and others in nuanced ways. They are capable of hearing and making effective use of information that is emotionally threatening, and have generally come to terms with painful experiences from the past, finding meaning in the experiences and growing from them. Individuals who match this prototype tend to express emotion appropriate in quality and intensity to the situation at hand. They generally find contentment and happiness in life's activities. They find meaning and fulfillment in guiding or nurturing others, in belonging and contributing to a larger community, and in the pursuit of long-term goals and ambitions. Individuals who match this prototype are able to use their talents, abilities, and energy effectively and productively. They enjoy challenges and take pleasure in accomplishing things. They are able to express themselves verbally, have a sense of humor, and tend to see things and approach problems in creative ways. |
References
Information & Authors
Information
Published In


History
Authors
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).