The association of institutional deprivation and reactive attachment disorder has been noted in the literature since the mid-20th century (
1–
4). Both types of the disorder—the emotionally withdrawn (inhibited) and the indiscriminately social (disinhibited) types—have been described in young children who have been maltreated or were raised in conditions of deprivation (
2–
4). Interest in the effects of institutional care persists to the present day because many children throughout the world are raised in institutions as a result of abuse or neglect, abandonment, or parental incapacity or death (
5–
7). Often, these institutions are large group settings with multiple caregivers whose rotating schedules do not support the development of a focused attachment relationship between a child and a given caregiver (
8,
9). Significant numbers of children living in institutions show signs of attachment disorders (
10). For children adopted from institutions, rates of attachment disorders are elevated but are lower than those for children living in institutions (
11).
To our knowledge, there have been no previous planned intervention studies of attachment disorders, although some natural experiments have provided valuable data. Tizard and colleagues (
12,
13) first systematically observed the development of what are now known as attachment disorders in groups of institutionally reared children. These children were placed in institutions, mostly at birth, and remained there at least until age 2. Between ages 2 and 4, some were adopted, some were returned to their parents, and some remained in institutions. At the initial follow-up assessment when the children were 4 years old, the majority of those who had remained in institutions exhibited signs of reactive attachment disorder, either the inhibited or the disinhibited type. Of those who had been returned to their parents or been adopted, none exhibited signs of the inhibited type, and a minority continued to exhibit signs of the disinhibited type (
13).
These findings were replicated in two longitudinal studies of young children adopted out of institutions in Romania. In a study of children adopted into Canada, signs of indiscriminate behavior persisted in a minority of children for several years after they had been adopted (
3,
11). Similarly, Rutter and colleagues (
4,
14–
16) found no signs of the inhibited type of reactive attachment disorder in children adopted before age 4, but a minority of children showed signs of indiscriminate behavior. Furthermore, the authors observed a linear relationship between duration of deprivation and signs of disinhibited reactive attachment disorder through age 6.
Since studies of children currently living in institutions have demonstrated that both types of the disorder are readily identifiable (
9,
13), the absence of the inhibited type and the persistence of the disinhibited type in children after they are placed in more favorable caregiving environments are notable. These findings suggest that the inhibited type may be more responsive to enhanced caregiving than the disinhibited type.
These adoption studies have inherent limitations, however. First, the studies did not include assessments of the children prior to adoption. Second, because children adopted out of institutions are not selected at random, the results of these naturalistic studies may not be representative. For example, one study (
12) found that redheaded children and children of mothers with mental health problems typically were not released for adoption. Third, the comparison groups for two recent studies (
11,
15) were Canadian and British children, respectively, rather than ethnically matched children, introducing the possibility that cultural differences may affect outcomes.
The Bucharest Early Intervention Project, which was designed as a randomized controlled trial of foster care as an alternative to care as usual among institutionalized young children, addressed many of the limitations of previous studies (
17). Despite 60 years of research comparing young children in foster care and those in institutional care, no randomized trial had been conducted until the Bucharest Early Intervention Project was initiated in 2001. Children in the study had been abandoned at or soon after birth and placed in institutional care in the custody of the government. They were assessed comprehensively at baseline and then randomly assigned to care as usual (including continued institutional care) or to placement in foster care, which was created as part of the project.
By including assessments of reactive attachment disorder prior to removal from institutions and by using well-validated measures administered longitudinally, this randomized controlled trial reduces selection bias and directly addresses questions about the responsiveness of children with reactive attachment disorder to enhanced caregiving. Elsewhere, we have demonstrated the positive impact of this intervention on brain functioning (
18), language development (
19), cognitive abilities (
20), attachment security (
21), physical growth (
22), and psychiatric disorders (
23). No previous studies have examined the impact of the intervention on attachment disorders. In this study, we addressed the following questions. First, did removing young children from institutions and placing them in foster care reduce signs of both the inhibited and the disinhibited types of reactive attachment disorder? Second, was the timing of the intervention (age at placement in foster care) related to signs of attachment disorder? And finally, did demographic factors (gender, ethnicity) or cognitive ability at baseline have an impact on the effect of placement on change in signs of reactive attachment disorder?
Method
Sample
Study subjects were three groups of young Romanian children enrolled in the Bucharest Early Intervention Project and repeatedly assessed over time; assessments were conducted at baseline (ages 6–30 months) and at ages 30, 42, and 54 months and 8 years (
17,
20).
All children under age 31 months (N=187) at study initiation (April 2001) who were cared for in the six study institutions in Bucharest were assessed for participation in the study. Children were screened for signs of exclusion criteria, which included genetic syndromes, fetal alcohol syndrome, and head circumference more than two standard deviations from normal. Fifty-one children met exclusion criteria, resulting in an initial study population of 136 children. Baseline comprehensive evaluations (
20,
24), which included assessments for signs of reactive attachment disorder, were conducted (
10). The children were then randomly assigned either to continued institutional care (the usual care group; N=68) or to placement in newly created foster care (the foster care group; N=68). One child in the foster care group was subsequently found to meet exclusion criteria and was excluded from further analyses.
A third group of never-institutionalized children, raised in families, was recruited from pediatric clinics in Bucharest (N=72). These children, who were born at the same maternity hospitals and whose families were from the same sectors as the children in the two study groups, served as a typically developing Romanian comparison group.
Over the course of the study, there was some movement of children from their original group assignment. All decisions regarding placement of institutionalized children were made by Romanian child protection officials with no interference from study personnel. We did, however, ensure that no child, once placed in foster care through the Bucharest Early Intervention Project, would be returned to an institutional setting, either during or after the study. A CONSORT diagram is available in the data supplement that accompanies the online edition of this article. We followed an intent-to-treat approach in all analyses so that original group assignment was maintained.
Foster Care Intervention
A foster care network consisting of 56 foster homes was created for the Bucharest Early Intervention Project, designed to ameliorate the effects of early institutionalization on young children, including reducing signs of attachment disorders. A description of this child-centered foster care intervention has been published elsewhere (
25). Project social workers supported foster parents in establishing warm, nurturing relationships with their foster children and assisted them in managing difficult child behavior. Foster parents were encouraged to view their foster children as members of the family and to become committed “psychological parents” (
25).
Measures
Reactive attachment disorder.
Signs of reactive attachment disorder were assessed with the Disturbances of Attachment Interview (A.T. Smyke and C.H. Zeanah, unpublished instrument), a semistructured interview that has been used to assess children raised in institutions (
9,
25,
26), young foster children (
27,
28), and young children exposed to domestic violence (
29). The instrument has shown strong convergent (
9,
30) and discriminant (
29) validity. The first five items of the interview assess signs of inhibited reactive attachment disorder, asking about whether the child has developed a preference for a specific caregiver, approaches the caregiver for comfort, responds to comfort when offered, engages in reciprocal social interaction, and regulates emotions well. Scores on these five items are rated 0 (often/clearly demonstrates the behavior), 1 (sometimes/somewhat demonstrates the behavior), or 2 (rarely/minimally demonstrates the behavior) (score range, 0–10). Three items assess signs of the disinhibited type, using the same ratings for questions about whether the child checks back with the caregiver when exploring, shows age-appropriate reticence around strangers, and demonstrates willingness to “go off” with a stranger (score range, 0–6). For children residing in foster or biological families, the foster or biological mother was interviewed. For institutionalized children, interviews were conducted with either the “favorite” caregiver (as determined by staff) or, if the child did not have a favorite caregiver, a caregiver who knew the child well and cared for the child on a regular basis. Two Romanian-speaking research assistants who were trained to reliability on the interview (
10) coded each interview. Discrepancies were resolved by conferencing, and a consensus code was recorded for each item.
Cognitive abilities.
Children's cognitive abilities at baseline were examined using the Bayley Scales of Infant Development–II (
31). A developmental quotient was derived because some children had scores below the basal score for the Bayley Scales and could be included in analyses only if a developmental quotient was computed. The developmental quotient at baseline for the children in the two study groups was dichotomized (median split at 77) for the analyses (
24).
Procedure
After baseline assessments, children were randomly assigned to care as usual or to foster care. Each child was given a number (siblings were placed together), and numbers were drawn from a hat and alternately assigned to the two groups. Subsequently, all decisions regarding children's placements were made by Romanian child protection officials. Thus, for example, children were sometimes returned to their biological families or placed in government-sponsored foster care that did not exist at the time the study began.
Interviews and assessments were conducted in the study laboratory.
Consent
After institutional review board approval was obtained from the universities of each of the principal investigators, approval was obtained from the local child protection commissions in Bucharest. The commissioner for child protection in each sector in which a child resided signed consent for individual children. The study was conducted in collaboration with the Institute of Maternal and Child Health and the Romanian Ministry of Health. In addition, assent for each procedure was obtained from each caregiver or parent who accompanied a child to a visit. The ethical considerations for study of this vulnerable group have been discussed in detail elsewhere (
32–
34).
Statistical Analysis
The effects of foster care intervention and of usual care on signs of reactive attachment disorder were measured across time (at baseline and at ages 30, 42, and 54 months and 8 years) and analyzed using repeated-measures analysis of variance (ANOVA; likelihood model, data missing at random, SAS PROC MIXED, two groups and five assessments), with post hoc comparisons based on least squares means. Age at placement in foster care was dichotomized at 24 months (median split) to examine the timing effects of the intervention. Gender, ethnicity (Romanian compared with Roma or other), and cognitive ability at baseline (higher compared with lower developmental quotient) were entered separately as between-subject factors to examine their impact on change in signs of reactive attachment disorder. All p values were based on two-tailed tests.
Results
Table 1 presents basic demographic information (gender and ethnicity) and lists the mean total scores for signs of inhibited and disinhibited reactive attachment disorder for the two study groups and the never-institutionalized comparison group. There were fewer Roma children in the never-institutionalized group. On average, children in the never-institutionalized group were younger at the baseline assessment than children in the study groups (data not shown). Preliminary analyses revealed no significant effect of gender or ethnicity, and these variables were excluded from further analyses.
Signs of Inhibited Reactive Attachment Disorder
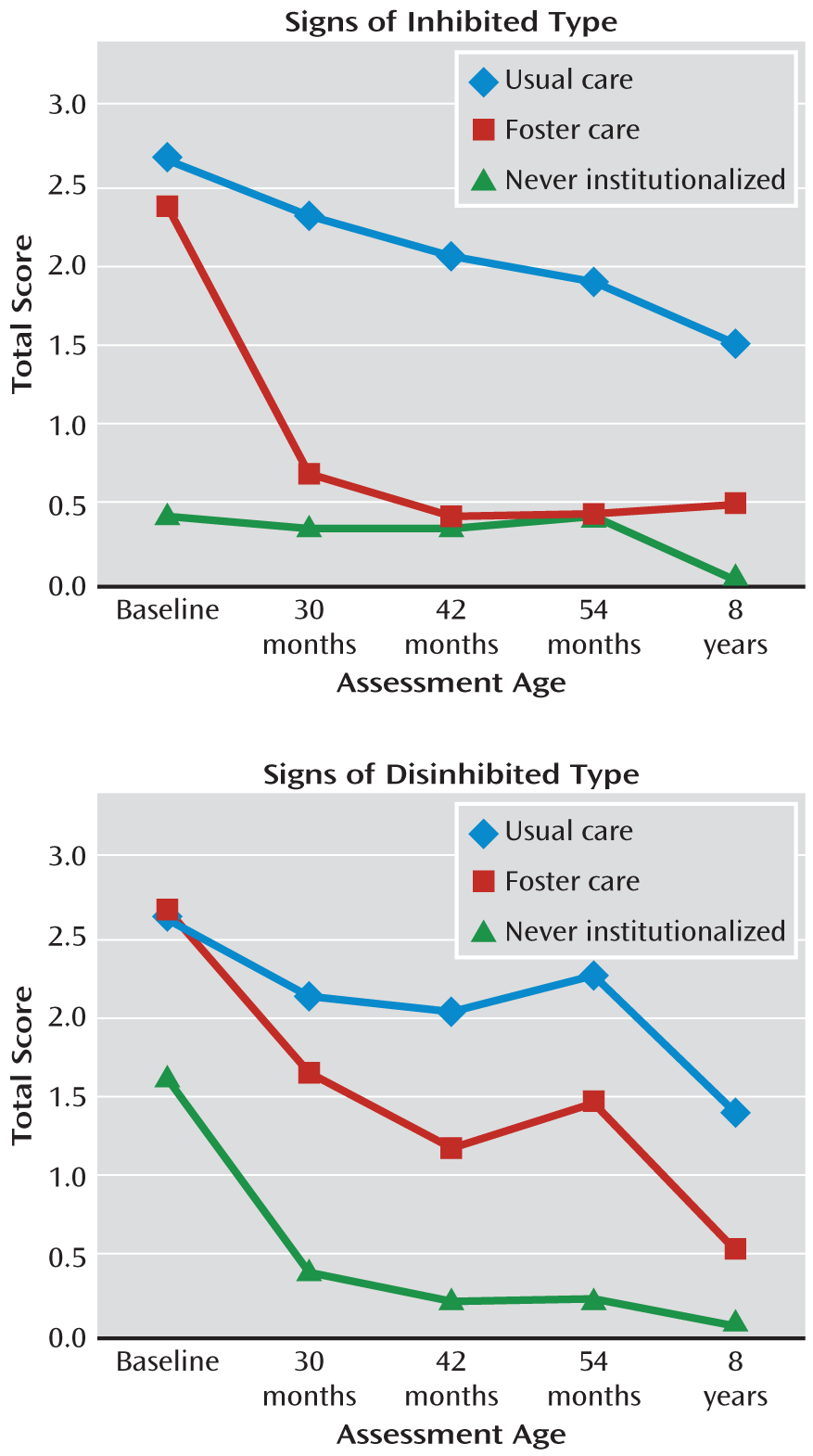
The repeated-measures analysis showed a significant group-by-time interaction (F=2.51, df=4, 475, p<0.05), indicating that scores decreased differentially for the usual care and foster care groups (
Figure 1). Post hoc comparisons at ages 30 months (t=4.51, df=475, p<0.001), 42 months (t=4.58, df=475, p<0.001), 54 months (t=4.07, df=475, p<0.001), and 8 years (t=2.70, df=475, p<0.01) all indicated fewer signs of inhibited reactive attachment disorder for children in the foster care group compared with those in the usual care group. Differences between the foster care group and the never-institutionalized group were evident at baseline and at ages 30 months and 8 years.
Signs of Disinhibited Reactive Attachment Disorder
The repeated-measures analysis showed significant main effects for change over time (F=12.72, df=4, 475, p<0.001) and for group (F=15.42, df=1, 133, p<0.001), but not for the group-by-time interaction, suggesting that scores did not decrease differentially for the usual care and foster care groups (
Figure 1). While respecting protection for multiple comparisons, we nevertheless decided that analyses of specific time points would be informative. Thus, we conducted post hoc comparisons and observed that at ages 42 months (t=2.61, df=475, p<0.01), 54 months (t=2.34, df=475, p<0.05), and 8 years (t=2.44, df=475, p<0.05), children in the foster care group had significantly fewer signs of disinhibited reactive attachment disorder relative to children in the usual care group. These findings may be attributed to the significant group main effect. There were significantly more signs in the foster care group than in the never-institutionalized group at each age measured after baseline.
Timing of Intervention
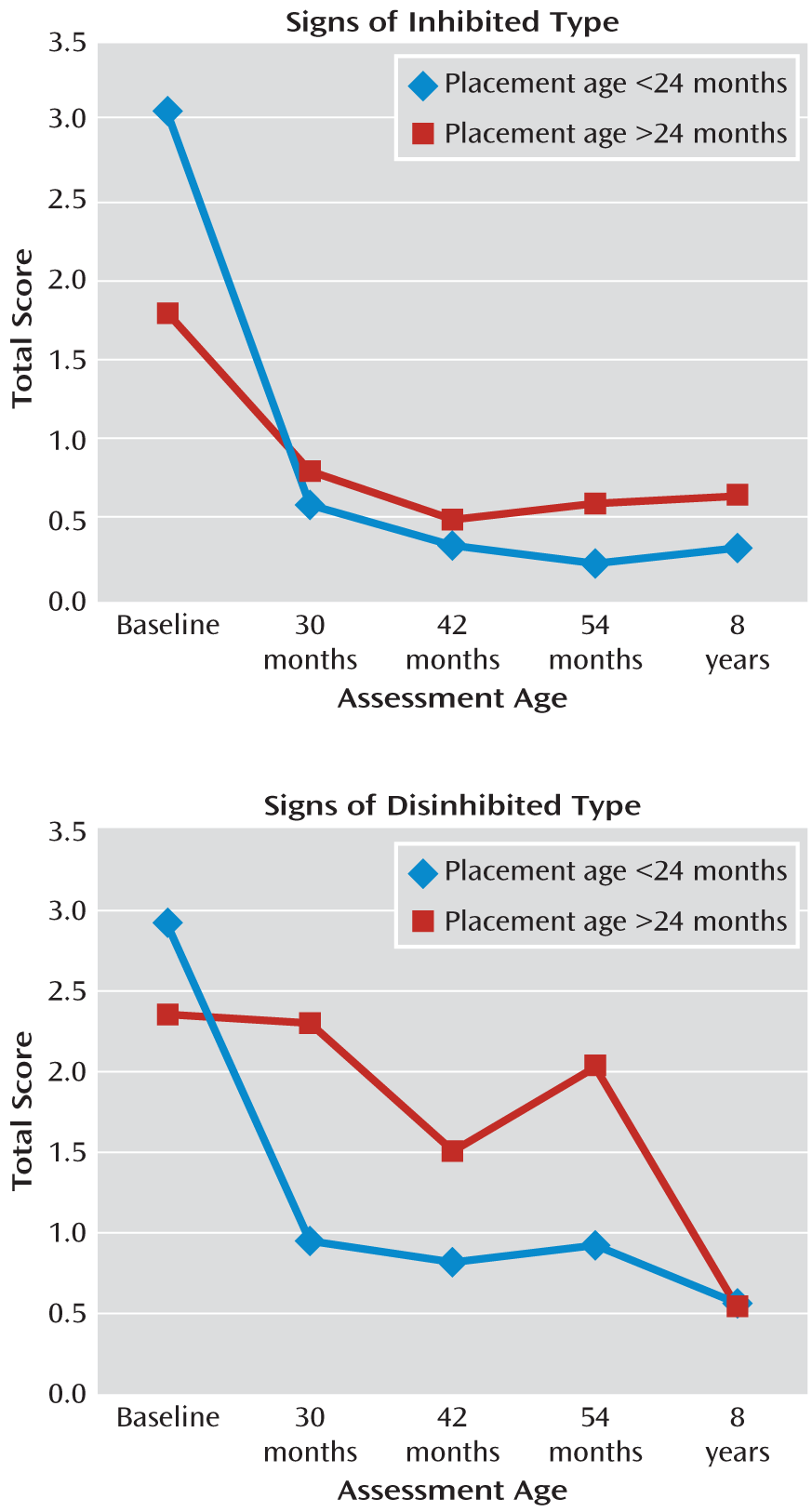
As shown in
Figure 2, children placed in foster care before age 24 months did not differ significantly from children placed after age 24 months across the course of the study through age 8 in signs of inhibited reactive attachment disorder.
With regard to signs of disinhibited reactive attachment disorder, repeated-measures analysis showed a significant interaction of age at placement by time (F=3.39, df=4, 239, p<0.05), indicating that scores decreased differentially for the children placed in foster care before age 24 months compared with those placed after that age. Post hoc analyses indicated that children placed in foster care before age 24 months had fewer signs of disinhibited reactive attachment disorder at ages 30 months (t=3.11, df=239, p<0.01) and 54 months (t=2.62, df=239, p<0.01) than did those placed after age 24 months. Differences were not evident at ages 42 months or 8 years.
Factors Related to Change in Signs of Reactive Attachment Disorder
Results of repeated-measures ANOVA revealed a baseline cognitive ability-by-group interaction (F=5.89, df=1, 127, p<0.05), indicating a differential effect of baseline cognitive ability on signs of inhibited reactive attachment disorder. Post hoc comparisons revealed more signs of this type of reactive attachment disorder among children in the usual care group with lower baseline cognitive abilities, across the entire intervention period, compared with children in this group with higher baseline cognitive ability (t=–4.24, df=127, p<0.001). This difference was not observed for the children in the foster care group.
With regard to signs of disinhibited reactive attachment disorder, repeated-measures ANOVA revealed a main effect for baseline cognitive ability (F=18.14, df=1, 127, p<0.001), suggesting that children with better cognitive abilities at baseline had fewer signs of this type of reactive attachment disorder across the entire intervention period. There was no significant effect of baseline cognitive ability on change over time in scores for reactive attachment disorder of either the inhibited or the disinhibited type.
Discussion
We report results of a randomized controlled trial of the effects of foster care as an intervention—to our knowledge, the first such trial—to address directly the effects of institutionalization, focusing on signs of reactive attachment disorder and its treatment. Our findings have important implications for children living in conditions of social deprivation and other forms of neglect.
The most important finding was that placement of young institutionalized children in quality foster care resulted in a marked reduction of signs of inhibited reactive attachment disorder and compellingly demonstrated resolution of the disorder, since signs were indistinguishable between children in the foster care group and those in the never-institutionalized group after age 30 months. The children had been with families an average of 8 months at the 30-month assessment, which may explain why adoption studies with follow-up periods of 1 year or more after adoption have not detected signs of this disorder (
3,
35).
Responsiveness of disinhibited reactive attachment disorder to intervention was less straightforward. Children in the foster care intervention arm had lower scores than those in the usual care arm at some test ages but higher scores than children who had never been institutionalized. Factors beyond an adequate family caregiving environment seem relevant to understanding how to reduce signs of disinhibited reactive attachment disorder (
36).
The timing of placement in foster care has been shown to have an impact on cognitive recovery for children who experienced institutional care (
20) and has some bearing on the question of whether there are sensitive periods during which children are more likely to recover from early deprivation. In the present study, we observed no effects of timing of placement in foster care on signs of inhibited reactive attachment disorder. The lack of a timing effect suggests that children raised in institutional settings retain a capacity for forming attachments, with no obvious sensitive period. When placed with families, children form new attachments (
21) and signs of inhibited reactive attachment disorder disappear. Results for disinhibited reactive attachment disorder with regard to age at placement in foster care were mixed. Scores decreased differentially for children placed before age 24 months, with scores noted to be lower at ages 30 and 54 months for this group.
These findings indicate that placement in families clearly eliminates signs of the inhibited type of reactive attachment disorder, as measured by the Disturbances of Attachment Interview, among young children raised in institutions, but it has a more attenuated effect on the disinhibited type. This raises the question of what additional components should be included in interventions for indiscriminate behavior, which can be a risk factor for subsequent psychiatric impairment and interpersonal difficulties. For example, training in reading and responding to social cues might lead to reductions in disinhibited social behavior. Such training would be enhanced by better characterization of the social cognitive abnormalities that presumably underlie indiscriminate behavior.
Regarding factors influencing intervention effects, gender and ethnicity appear to be unrelated to the recovery of young children from reactive attachment disorders. Among children in the usual care group, those with lower cognitive ability at baseline had more signs of the inhibited type over the course of the study than did children with higher cognitive ability. This effect was not evident among children in the foster care group, suggesting that the intervention of foster care was beneficial to children regardless of their cognitive abilities. Lower cognitive ability at baseline was also related to higher scores for signs of disinhibited reactive attachment disorder for both groups. Taken together, these findings highlight the increased risk for children with lower cognitive ability exposed to early adversity.
One limitation of the study may be that because of its longitudinal nature and the detailed questioning of caregivers during the interview, interviewers were not always blind to group status. Another limitation may be the use of caregiver report, a method often used in studies of early childhood psychopathology. Nevertheless, our confidence in the caregiver reports for this sample is high because they converge with observer ratings (
29).
Results from this study have implications not only for young children raised in institutions but also for those who have experienced maltreatment (
29,
37,
38) and other forms of neglect. Changing children's experiences by placement in child-centered foster care demonstrably reduced signs of an impairing disorder. This is the strongest evidence to date on what interventions are needed to treat attachment disorders in young children. Future studies should examine the long-term effects of such interventions, more carefully identify which components are critical to successful adaptation, and provide a greater understanding of the nature of both types of reactive attachment disorder as children mature.