Fragile X syndrome is due to a trinucleotide expansion of more than 200 CGG repeats in the fragile X messenger ribonucleoprotein 1 gene (
FMR1) on the X chromosome. It is the most common inherited cause of intellectual disability (ID) (
1) and has a well-established association with psychiatric phenomena, such as anxiety disorders (
2). Fragile X premutation, defined as 55–200 CGG repeats, is associated with conditions such as primary ovarian insufficiency (FXPOI) and a tremor/ataxia syndrome (FXTAS) (
3). FXTAS is a neurodegenerative disease that manifests mostly in men over 50 years of age with an intention tremor, cerebellar gait ataxia, parkinsonism, and neuropathy (
4). Symptomatic FXTAS is also associated with deterioration in cognition, often leading to dementia, and an increase in neuropsychiatric symptoms such as apathy (
5). Of the premutation carriers who do not have FXTAS (predominantly women and younger men), there remains an increased prevalence of psychiatric disorders (
3,
6). There is debate whether psychiatric conditions in premutation carriers are prodromal to FXTAS or independent of FXTAS pathogenesis (
7). Accordingly, the term fragile X–associated neuropsychiatric disorders (FXANDs) was proposed in 2018 to recognize these neuropsychiatric manifestations among fragile X premutation carriers without FXTAS (
6). The term fragile X-associated neuropsychiatric conditions (FXANCs) has also been proposed to distinguish neuropsychiatric conditions in premutation carriers that do not meet the threshold of a disorder and to distinguish these neuropsychiatric phenomena from other fragile X–associated conditions, such as FXTAS and FXPOI (
8).
The neuropathology of fragile X syndrome is characterized by a deficiency of fragile X protein (FMRP), which is required for normal brain development (
9). As the
FMR1 gene is not completely silenced with less than 200 CGG trinucleotide repeats, it was originally proposed that fragile X premutation was not associated with the fragile X phenotype (
10). It is now known that fragile X premutation carriers have increased
FMR1 mRNA, decreased FMRP, and polyglycine-containing protein (FMRpolyG) and ubiquitin-positive intranuclear inclusions. Toxic polypeptides are produced from
FMR1 mRNA, and protein sequestration occurs due to interactions with the expanded CGG-repeat RNA. These changes are associated with neuronal cell death and dysfunction (
11). The neuropathology of premutation carriers with or without FXTAS is similar in that both have mitochondrial dysfunction; those without FXTAS, however, have fewer intranuclear inclusions in astrocytes and lack white matter disease (
11,
12). Structural neuroimaging of premutation carriers without FXTAS has shown generalized cerebral atrophy, increased ventricular size, and regional changes such as decreased grey matter in the dorsomedial frontal regions. These neuroimaging changes in premutation carriers are milder and less frequent than in those with FXTAS (
13).
Despite these established neuropathological and radiological abnormalities in premutation carriers, the neuropsychiatric phenotype of premutation carriers without FXTAS is not clearly defined. The rate of psychiatric disorders in premutation carriers without FXTAS reported in previous reviews varies significantly. For example, rates of developmental delay have been reported to range from 6% to 32% (
3), rates of depression from 20% to 43% (
14), and rates of anxiety from 12% to 41% (
15). In contrast, the prevalence of neuropsychiatric phenomena in premutation carriers with FXTAS has been described in prior reviews with a clear phenotype of apathy, irritability, depression, anxiety, and a neurodegenerative cognitive impairment that progresses to dementia (
4,
16,
17). Accordingly, there is a consensus on the clinical presentation of FXTAS with established diagnostic criteria (
4). This systematic review thus aimed to define a consensus on the rate of psychiatric disorders in premutation carriers without FXTAS. Also, as fragile X syndrome is predominately associated with neurodevelopmental disorders, the prevalence of the premutation in neurodevelopmental disorders was also reviewed to strengthen the association between the
FMR1 gene premutation and FXAND phenotype.
Methods
Search Strategy
This review was completed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (
18). Search methods, selection criteria, and data collection were prospectively planned. Keywords included “fragile X–associated neuropsychiatric disorder,” “fragile X–associated neuropsychiatric condition,” “FXAND,” “fragile X premutation,” and “
FMR1 premutation.” For each study, the title and abstract were reviewed for reference to psychiatric disorders in patients with fragile X premutation and fragile X genetic testing in probands with neurodevelopmental disorders. The full text was then reviewed for eligibility criteria. Finally, the reference lists from the included studies were searched for further citations.
Information Sources
Literature was reviewed from two main medical databases: PubMed and Web of Science. There was no time limitation set for the published literature. The databases were accessed on July 31, 2021.
Eligibility Criteria
Studies were included if they met all of the following criteria:
•
Observational studies were published in a peer-reviewed journal and in English.
•
Studies reported the prevalence of either psychiatric disorders in patients with fragile X premutation without FXTAS or fragile X premutation in probands diagnosed with a neurodevelopmental disorder.
•
Studies reported psychiatric disorders recognized by standardized diagnostic criteria (e.g., the Diagnostic Statistical Manual [DSM] criteria, International Classification of Diseases [ICD] criteria, or Research Diagnostic Criteria [RDC]).
•
For studies that assessed for ID, studies used an assessment measure of both intellect and adaptive functioning (e.g., studies that just used an assessment of intellect to diagnose ID were not included).
Intervention studies (e.g., studies that assessed anxiety associated with genetic testing), studies that duplicated the cohort from another study (if this occurred, studies with the smaller sample size, studies other than the original if the cohorts were identical, studies with the least information, or studies with a less comprehensive psychiatric assessment method were excluded), and studies that skewed the prevalence of the psychiatric disorder(s) due to selection bias were excluded.
Data Extraction
The following data were extracted from each study: study characteristics, sample characteristics, and prevalence. Study characteristics included study design, psychiatric assessment method, inclusion of a control group, and genetic testing. Sample characteristics included the sample size, sex, age, and CGG repeat length (either as mean±SD or the study’s definition of a premutation range). All data were rounded to one decimal place.
Psychiatric Assessment Methods
Psychiatric disorders were separated into four categories based on the following assessment methods: diagnostic criteria, rating scales, subscales within larger instruments, and medical history.
Diagnostic criteria.
Studies that used diagnostic criteria were documented as those that used a semistructured or nonstructured clinical interview. The use of a semistructured clinical interview, in combination with the assessment of diagnostic criteria, is considered the gold standard to diagnose psychiatric disorders (
19). With the exception of studies assessing autism, all studies that used a semistructured interview used it in combination with an assessment of diagnostic criteria. The semistructured clinical interviews included the Structured Clinical Interview for DSM Disorders (SCID) (
20), Anxiety Disorders Interview Schedule (ADIS) (
21), Schedule for Affective Disorders and Schizophrenia (SADS) (
22), Diagnostic Interview for Genetic Studies (DIGS) (
23), Family Informant Schedule Criteria (FISC) (
24), Autism Diagnostic Observation Scale (
25), and Autistic Diagnostic Interview Revised (
26). Diagnostic criteria included the DSM criteria, ICD criteria, and RDC. The RDC was used in combination with the SADS, and the DSM criteria were used in combination with the SCID, ADIS, FISC, and DIGS.
Rating scales.
Studies that used rating scales or subscales were only included if they specified the name of the instrument used and the instrument mapped to ICD, DSM, or RDC criteria. For studies that used rating scales, the cutoff scores used to define the presence of the psychiatric disorder were documented. The rating scales included the Center for Epidemiologic Studies Depression Scale (CES-D) (
27), Depression Anxiety Stress Scales (
28), Hospital Anxiety and Depression Scale (HADS) (
29), Social Phobia and Anxiety Inventory (
30), Liebowitz Social Anxiety Scale (
31), Brown Attention-Deficit Disorder Scale for Adults (
32), Conners’ Parent Rating Scales–Revised: Short Form (CPRS-R:S) (
33), Autism Spectrum Quotient (AQ) (
34), Mullen Scales of Early Learning (
35), Vineland Adaptive Behavior Scale (
36), and Griffiths Mental Developmental Scale (
37).
Subscales.
The included subscales were all subsections of larger instruments. They included the anxiety section of the Developmental Behavior Checklist (
38), the anxiety section of the Profile of Mood States (POMS) (
39), and the anxiety, depression, and obsessive-compulsive disorder (OCD) sections of the Symptom Checklist–90–Revised (
40).
Medical history.
The studies that reported psychiatric disorder based on medical history were separated into those that used medical records or self-reported history (e.g., psychiatric history was disclosed by the patient but not validated by their medical records).
Psychiatric Disorders
As the majority of studies used DSM-IV diagnostic criteria, psychiatric disorders were grouped into categories from the DSM-IV. This included neurodevelopmental, depressive, bipolar, anxiety, and psychotic disorders. Neurodevelopmental disorders included developmental delay (DD), ID, attention-deficit hyperactivity disorder (ADHD), and autism spectrum disorder (ASD). Depressive and bipolar disorders (mood disorders) included major depressive disorder, persistent depressive disorder (dysthymia), and bipolar disorders I and II. Anxiety disorders included generalized anxiety disorder (GAD), panic disorder, social phobia, specific phobia, agoraphobia, OCD, and posttraumatic stress disorder (PTSD). Psychotic disorders included schizophrenia, schizoaffective disorder, and psychotic disorder not otherwise specified. Studies that used differing terminologies for the same psychiatric disorder were grouped together under the same DSM diagnostic label (e.g., learning disability was grouped with ID).
Estimation of Prevalence
Overall current (point prevalence) and lifetime prevalence estimates of psychiatric disorders were calculated as a weighted average percentage.
Quality Appraisal
The quality of the studies was assessed using the Joanna Briggs Institute Prevalence Critical Appraisal (JBIPCA) Checklist for prevalence studies (
41). Each study was assessed by nine criteria. They were graded as one for meeting each criterion or zero for not meeting the criterion. A total score ranging from zero to nine was assigned to each study, with nine representing the highest quality. These data are available in the
online supplement accompanying the online version of this article.
Results
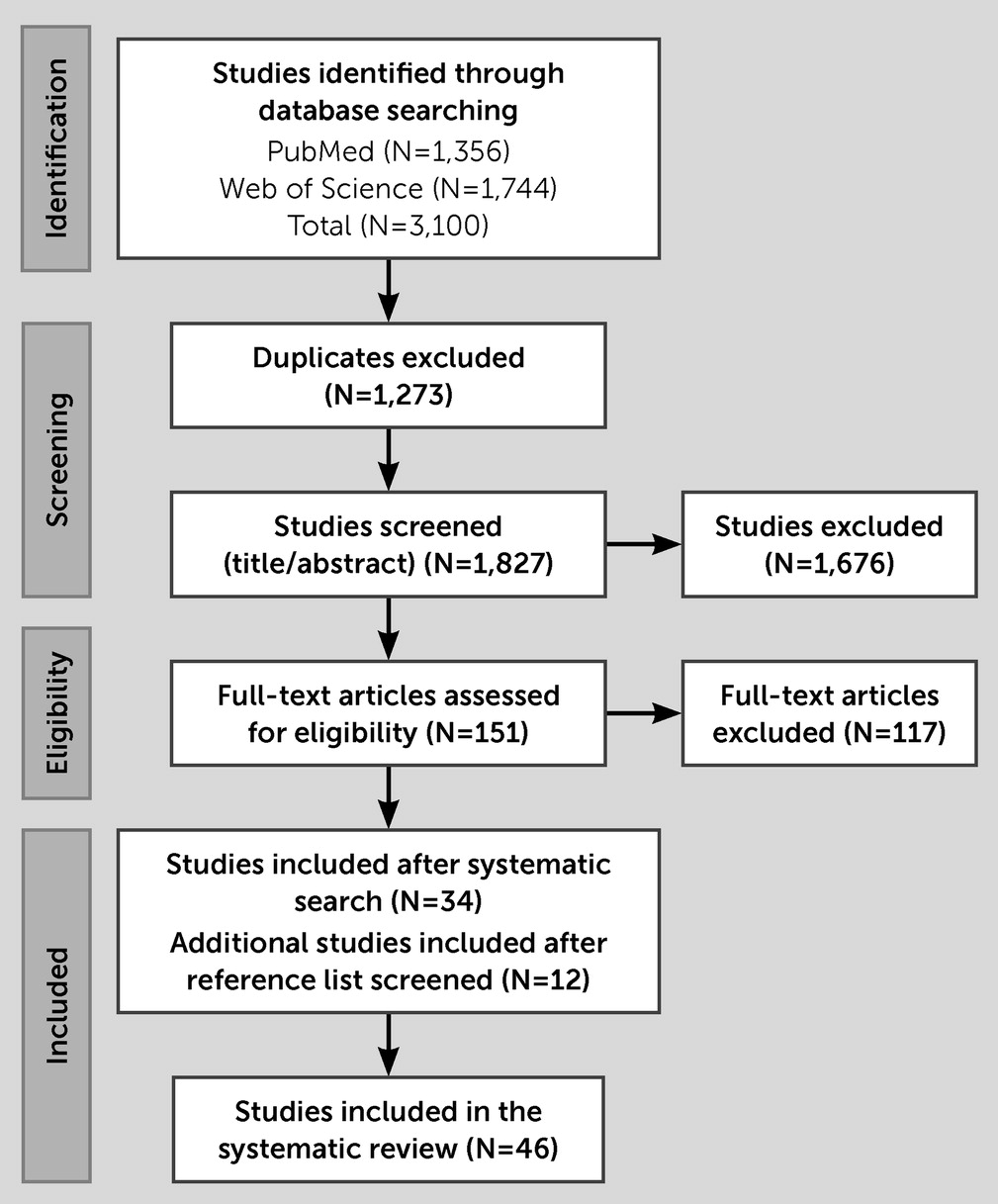
The systematic literature search generated 3,100 articles, of which 1,827 articles remained after duplicate removal. One hundred fifty-one articles were reviewed in full, with 34 meeting eligibility criteria. An additional 12 articles were identified after reference list review (
Figure 1). The final 46 articles assessed neurodevelopmental (N=29) (
42–
70), mood (N=17) (
45–
47,
51,
71–
83), anxiety (N=21) (
45–
48,
51,
71–
74,
76–
87), and psychotic (N=3) (
48,
77,
83) disorders.
Prevalence of Fragile X Premutation in Those With Neurodevelopmental Disorders
Five studies were used to assess the prevalence of fragile X premutation in probands with neurodevelopmental disorders (
52–
56). Three studies used diagnostic criteria (
52–
54), one used a rating scale (
56), one used both a semistructured interview and rating scale (
55), none used subscales, and 15 used medical history (
56–
70). Three out of the five studies used for the prevalence estimates separated sexes (
53–
55), and no studies had a control group (
Table 1).
The average premutation prevalence in probands with DD/ID was 5.0% (
52,
55,
56); with ADHD, 6.3% (
52); and with ASD, 2.6% (
52–
55). Sex differences could only be assessed in ASD, with the fragile X premutation being more prevalent in males (1.5%) than females (0.0%) (
53–
55). However, these data were skewed with two studies reporting a prevalence of 0.0% for both sexes (
54,
55) and one study reporting a prevalence of 9.4% for males (
53).
Prevalence of Psychiatric Disorders in Fragile X Premutation Carriers
Neurodevelopmental disorders.
Five studies were used to assess the prevalence of neurodevelopmental disorders in premutation carriers (
42–
46). Three studies used a semistructured interview or diagnostic criteria (
42–
44), two studies used rating scales (
45,
46), no studies used subscales, and seven studies used medical history (
43,
45,
47–
51). Four of the five included studies separated sexes (
42,
43,
45,
46) (
Table 2). Three studies had a control group (
44–
46) (
Table 3).
DD/ID: No studies met criteria to evaluate the prevalence of DD or ID in premutation carriers.
ADHD: The average point prevalence of ADHD was 29.0% (
42,
45). The prevalence of ADHD was higher in males (38.0%) than females (25.7%) (
42,
45). ADHD was also more prevalent in premutation carriers (25.7%) than in those in the control group (8.6%) (
45).
ASD: The average prevalence of ASD was 4.7% (
42–
44,
46). The prevalence of ASD was higher in males (7.7%) than females (2.4%) (
42,
43,
46). ASD was also more prevalent among premutation carriers (10.3%) than among those in the control group (0.0%) in the studies that included a control group (
44,
46).
Mood disorders.
Thirteen studies were used to assess the prevalence of mood disorders (
45,
46,
71–
80,
83). Nine studies used a semistructured interview with diagnostic criteria (
71–
78,
83), four studies used a rating scale (
45,
46,
79,
80), one study used a subscale from a larger instrument (
81), and three studies used medical history (
47,
51,
82). Twelve of the 13 studies separated sexes (
45,
46,
72–
80,
83) (
Table 2). Eight studies had a control group (
45,
46,
73,
76–
79,
83) (
Table 3).
The average lifetime and point prevalence of any mood disorder was 48.3% and 5.4%, respectively (
71,
72,
77). All mood disorders were more common in premutation carriers than in those in the control group, with the exception of bipolar I disorder, which was 0.0% in both control and premutation carrier groups (
77).
Depressive disorders: The average lifetime and point prevalence of all depressive disorders was 40.7% and 24.5%, respectively (
45,
46,
73,
74,
77,
79,
80,
83). The average lifetime and point prevalence of major depressive disorder was 38.4% and 4.3%, respectively (
71–
77,
83). The average lifetime and point prevalence of dysthymia was 12.5% and 0.0%, respectively (
71–
74,
76–
78,
83). The point prevalence of depressive disorders was similar between males and females (26.9% vs. 24.4%); however, males had an almost threefold increase in lifetime dysthymia (33.3% vs. 11.2%) (
45,
46,
72–
74,
76,
78–
80,
83). No other sex differences could be assessed. Studies that included control groups reported only slightly higher lifetime prevalence (38.8% vs. 34.7%) but a clearly higher point prevalence (24.3% vs. 13.7%) of depressive disorders among those in the premutation carrier group than those in the control group (
45,
46,
73,
77,
79,
83).
Bipolar disorders: The average lifetime and point prevalence of any bipolar disorder was 8.7% and 1.1%, respectively (
71,
72,
74,
77,
83). There was variability in definition: one study (
83) included bipolar I, bipolar II, and subthreshold bipolar disorders (cyclothymic disorder); two studies (
72,
77) only included bipolar I and II; the final study (
71) did not specify the types of bipolar disorders included. The lifetime prevalence of bipolar I was 0.0% (
77), and lifetime prevalence of bipolar II was 11.3% (
74,
77). No evaluation of sex differences could be made. The lifetime prevalence of any bipolar disorder was slightly higher in premutation carriers than in those in the control groups (12.5% vs. 7.0%) (
77,
83).
Anxiety disorders.
Twelve studies were used to assessed the prevalence of anxiety disorders (
45,
46,
71–
74,
76–
79,
83,
84). Nine studies used a semistructured interview with diagnostic criteria (
71–
74,
76–
78,
83,
84), three studies used a rating scale (
45,
46,
79), four studies used a subscale (
80–
82,
85), and six studies used medical history (
45,
47,
48,
51,
86,
87). Ten out of the 12 studies separated sexes (
45,
46,
72–
74,
76–
79,
83) (
Table 2). Nine studies had a control group (
45,
46,
73,
76–
79,
83,
84) (
Table 3).
The average lifetime and point prevalence of any anxiety disorder was 40.0% and 33.4%, respectively (
46,
71–
74,
77,
83,
84). The average lifetime prevalence of anxiety disorders was higher among premutation carriers than among those in the control group (38.9% vs. 29.0%) as was the point prevalence (57.8% vs. 29.2%) (
46,
73,
77,
83,
84). Exceptions to this general tendency were that the point prevalence of PTSD was lower among premutation carriers than among those in the control groups (0.0% vs. 6.5%), as was that of specific phobia (6.7% vs. 12.9%) (
84).
GAD: The average lifetime and point prevalence of GAD was 7.2% and 7.4%, respectively (
71–
74,
76,
77,
83,
84). No evaluation of sex differences could be made.
Panic disorder: The average lifetime and point prevalence of panic disorder was 13.5% and 5.9%, respectively (
71–
74,
77–
79,
84). The lifetime prevalence of panic disorder was similar in males and females (12.5% vs. 13.6%); however, the point prevalence of panic disorder was higher in males than females (11.5% vs. 5.8%) (
72–
74,
77–
79).
Phobias: The average lifetime and point prevalence of social phobia was 21.1% and 18.7%, respectively (
45,
71–
73,
76–
79,
83,
84). The average lifetime and point prevalence of specific phobia was 14.8% and 4.6% respectively (
71–
74,
84). The average lifetime and point prevalence of agoraphobia was 3.6% and 2.8%, respectively (
72,
73,
77,
84). The lifetime prevalence of social phobia was lower in males than females (8.3% vs. 20.4%); however, the point prevalence of social phobia was similar in males and females (19.2% vs. 18.9%) (
45,
72,
73,
76–
79,
83).
OCD: The average lifetime and point prevalence of OCD was 5.3% and 4.7%, respectively (
71–
74,
77,
78,
84). The lifetime prevalence of OCD was higher in males than females (25.0% vs. 4.1%) (
72–
74,
77,
78).
PTSD: The average lifetime and point prevalence of PTSD was 8.9% and 0.0%, respectively (
71–
74,
84). No evaluation of sex differences could be made.
Psychotic disorders.
Two studies were used to assess the prevalence of psychotic disorders (
77,
83). Two studies used a semistructured interview with diagnostic criteria (
77,
83), no studies used a rating scale or a subscale, and one study used medical history (
48). Both studies used to assess the prevalence of psychotic disorders included only females (
77,
83) (
Table 2). Both studies had a control group (
77,
83) (
Table 3).
The average lifetime prevalence of any psychotic disorder was 0.9% (
77,
83). The lifetime prevalence of both schizophrenia and schizoaffective disorder was 0.0% (
77,
83). No evaluation of sex differences could be made. The lifetime prevalence of psychotic disorders was lower among premutation carriers than among those in control groups (0.9% vs. 2.0%) (
77,
83).
Discussion
Summary of Results
This systematic review included 46 studies (
42–
87). For the prevalence of fragile X premutation in neurodevelopmental disorder probands, five studies were used (
52–
56). There was a prevalence of 5.0% for DD/ID, 6.3% for ADHD, and 2.6% for ASD. From these studies, probands with ASD were the least likely to have the fragile X premutation (2.6% vs. 5.0%–6.3%). The only sex difference assessed was for ASD, and the analysis revealed that males were more likely than females to have the fragile X premutation (1.5% vs. 0.0%).
For the prevalence of psychiatric disorders in premutation carriers, 17 studies were used (
42–
46,
71–
80,
83,
84). The disorders that were more prevalent in premutation carriers than in those in the control group were neurodevelopmental and anxiety disorders, specifically ADHD (25.7% vs. 8.6%), ASD (10.3% vs. 0.0%), social phobia (24.5% vs. 8.8%), and GAD (8.4% vs. 3.3%). Bipolar II disorder was also more prevalent in premutation carriers (11.6% vs. 3.4%); however, the lifetime prevalence of most other mood disorders was similar in the premutation carrier and control groups. Psychotic disorders were less prevalent in the premutation carrier group than the control group (0.9% vs. 2.0%). For the studies that differentiated between sexes, psychiatric disorders were generally more common in males or similar between sexes. The only disorder significantly more prevalent in women was lifetime social phobia, which could be explained by inconsistencies in the data.
Fragile X Premutation in Those With Neurodevelopmental Disorders Compared to Population Estimates
The rate of fragile X premutation in the general population varies from 0.39% to 0.77% in females and 0.12% to 0.4% in males (
88). The rates of fragile X premutation in the prevalence estimates included in this review were universally higher than the general population (2.6%–6.3% vs. 0.1%–0.8%). In contrast to the five studies used for these prevalence estimates (
52–
56), there were 15 studies with much larger cohorts that used medical history (
56–
70). These studies had rates of fragile X premutation generally similar to or less than the general population. Though this could be explained by a selection bias in the studies that used medical history with unknown assessment methods, thus increasing the risk of misclassification, these results are nonetheless important. Most of these studies that relied only on medical history suggested probands with neurodevelopmental disorders do not have higher rates of fragile X premutation.
Psychiatric Disorders in Premutation Carriers Compared to Population Estimates
The National Comorbidity Survey Replication (NCS-R) is one of the few studies to use a semistructured interview to assess psychiatric disorders in a large population-based cohort (
89). Compared to NCS-R results (
90–
94), the lifetime rates of all psychiatric disorders except bipolar I disorder and psychotic disorders appeared to be higher in premutation carriers than the general population. The NCS-R study did not assess for ASD; however, the prevalence of ASD was also higher in premutation carriers than other general population estimates (4.7% vs. 0.2%) (
95). The lifetime rates of psychiatric disorders in the control groups included in the reviewed studies were generally consistent with the NCS-R results, with the exception of depressive disorders and specific phobias. The control groups had much higher rates of major depressive disorder (30.1% vs. 16.6%), dysthymia (15.5% vs. 2.5%), and specific phobia (41.7% vs. 12.5%) in the reviewed studies than in the NCR-R population estimates (
Table 4).
Limitations
Study quality.
The majority of studies identified by this review scored below six on the JBIPCA quality appraisal checklist; only five studies scored six or more (
43,
47,
51,
55,
79). The most common reasons for low quality scores were cohort selection, assessment method, and response rate. Most studies had small sample sizes; they recruited from cascade genetic testing, and their demographics were not documented or did not represent the general population. The age of the cohort was not reported in 30.4% (14/46) of studies. This is important, as fragile X is an X-linked condition, and psychiatric disorders are known to have different ages of onset (
96). Thus, younger cohorts would likely underestimate the lifetime prevalence for some diagnoses. Regarding sex, 22.7% (10/46) of studies did not separate sexes; 34.8% (16/46) included only females; and 13.0% (6/46) included only males. We propose that this represents a major limitation in the literature to date. X-linked genetic mutations characteristically manifest differently in males and females, as is already established for fragile X syndrome and FXTAS. Accordingly, grouping sexes together could potentially give rise to clinically spurious conclusions; for instance, if a disorder were common in males but rare in females, reporting an overall mean would misinform risks in both sexes. To account for demographic variations, studies should have a control group. Unfortunately, 41.2% (7/17) of the studies used for the psychiatric prevalence estimates did not include a control group. Finally, 60.9% (28/46) of studies used medical history or subscales. There is thus a need for future research to clearly document demographics, include a control group, and use valid assessment methods.
Assessment methods.
Psychiatric disorders were assessed by a variety of methods, and prevalence varied among these studies. Although the gold standard to assess psychiatric disorders is a semistructured clinical interview in conjunction with the assessment of diagnostic criteria, there was variation between studies even when this method was used. Different semistructured clinical interviews were used between studies, and importantly, the diagnostic criteria used also varied. Although the majority of studies used DSM-IV diagnostic criteria, there have been significant changes in the classification and illness terminology in the DSM-5. For example, the DSM-5 reclassified anxiety disorders to anxiety, obsessive-compulsive and related, and trauma- and stressor-related disorders.
It can sometimes be impractical to use the gold-standard method to assess psychiatric disorders in research; thus, rating scales are often used instead. Rating scales generally assess only point prevalence; thus, the lifetime estimates did not include studies that used rating scales. For example, someone may not meet the cutoff score for GAD on the HADS at one point in time but may at another point. The use of different methodologies to calculate lifetime and point prevalence rates may explain inconsistencies in the results. For example, the average point prevalence of social phobia in males was much higher than the lifetime prevalence (19.2% vs. 8.3%). This is impossible, but it could be explained by the use of rating scales compared to semistructured interviews. Accordingly, the exact prevalence rates identified by this review should be interpreted with caution. Instead, the general themes of this review are likely to be more meaningful—for example, the phenotype and sex distribution of FXANDs was similar to those observed with fragile X syndrome itself.
Rating scales for anxiety and depressive disorders are normally given cutoff scores that correlate to “any depressive” or “any anxiety” disorder. For example, the CES-D has been shown to accurately predict the presence of any DSM depressive disorder at a cutoff score greater than 16 (
97). Some studies identified in this review, however, did not indicate the cutoff scores they used (
46,
55,
79). This is problematic as they may not have used the recommended cutoff scores, which would result in misrepresentation of the psychiatric disorder in their cohort. For instance, the only study that used an anxiety rating scale did not state a cutoff score and reported a far higher rate of anxiety (63.0%) than the pooled prevalence from the studies that used a semistructured interview (19.4%). Future studies should clarify the cutoff scores used.
The studies that used subscales of larger instruments also had rates that were inconsistent and varied significantly from the other studies. The study that assessed OCD with the SCL-90R showed that 61.1% of participants had clinically significant symptoms, compared to the semistructured interviews which showed that 4.7% of participants had OCD. The four studies that assessed anxiety disorders with subscales reported prevalence rates that varied between 17.1% and 65.4% (
80–
82,
85). These findings could be explained by the issues associated with using subscales from larger instruments. For example, the subscales on the SCL-90 have been shown to have significant overlap and are only slightly better than chance in predicting the relevant diagnosis (
98).
Although studies that used medical records were not included in the final results due to reporting bias, there were nonetheless some interesting insights. One study identified 98 premutation carriers from electronic health records who were unaware of their genetic status (
51). In this study, the lifetime prevalence of major depressive disorder was reported to be 4.2%–7.7%; ADHD, 15.4%; and anxiety disorders, 15.4%. These rates were much lower than those identified by this review, suggesting underdocumentation in medical records using a retrospective methodology. Nonetheless these results offer insight into the rate of psychiatric conditions unconfounded by personal concerns for genetic status, the stress associated with being a carer for someone with fragile X syndrome (
99), and the bias from clinicians assessing these patients. Future studies should either blind clinicians to genetic status or recruit premutation carriers from population-based screening.
Prevalence estimates.
This review calculated lifetime prevalence from all studies that met the inclusion criteria, yet some studies had much younger cohorts. For example, two studies that assessed mood and anxiety disorders had cohorts as young as 18 (
75,
76). As lifetime estimates of psychiatric conditions increase with age, studies with younger cohorts likely underestimated the lifetime rates (
90).
The number of studies that met the inclusion criteria for the prevalence estimates were not universally the same between psychiatric conditions. For instance, the prevalence of fragile X premutation in ADHD relied on only one study for each condition. In contrast, eight studies were used for the prevalence estimate of major depressive disorder in premutation carriers. The cohort sizes used for these estimates also varied. The prevalence estimates of fragile X premutation in probands with ADHD were based only on 16 people. In contrast, the estimates of psychiatric conditions in premutation carriers were based on larger cohorts, once again with the exception of ADHD which included only 48 people.
Genetic testing.
The definition of fragile X premutation range and testing methods varied. Some studies included patients with fragile X premutation without specifying the number of repeats or laboratory testing method (
49,
60,
62,
72,
86). This is important as some PCR testing methods fail to detect CGG repeats in the premutation range (
100). Other studies used a range that was lower than the currently established range of 55–200 CGG repeats. For example, studies included premutation carriers with CGG repeats of 50–80 (
61), 50–200 (
76), 52–200 (
64), 50–60 (
65), 52–200 (
63), and 45–198 (
85). Also, few studies assessed patients for genetic variables such as mosaicism.
Conclusions
This review found that the rates of fragile X premutation in those with neurodevelopmental disorders were universally higher than general population estimates. In addition, psychiatric conditions were generally more common in premutation carrier groups than in control groups and in general population estimates. The most prevalent psychiatric conditions were neurodevelopmental disorders, anxiety disorders, and bipolar II disorder. Psychiatric conditions were more prevalent in male premutation carriers. This neuropsychiatric phenotype and sex distribution are similar to those among individuals with fragile X syndrome. The studies included had significant methodical variation that could explain the variation in results. Accordingly, more detailed research is required on FXANDs moving forward; studies should identify cohorts from population-based sampling, describe the cohort demographics, include a demographically matched control group, stratify the sexes and prioritize the use of validated assessment methods.
Acknowledgments
The authors thank Dr. Carol Ann Flavell for providing grammatical assistance during the revision of the manuscript.