Incarceration of people with mental illness is a major social, clinical, and economic concern. Much research has focused on the high prevalence of mental illness among persons in the criminal justice system. In 2007, an estimated 2,161,705 people with severe mental illness were incarcerated in the United States (
1). A U.S. Bureau of Justice Statistics special report found that 64% of jail inmates had mental illness symptoms (
2). A 2007 study found that 15% of male and 31% of female inmates in five jails (N=822) had severe mental illness (
1). A retrospective study of a random sample of inmates (N=104) found that 76% had severe mental illness (
3). A national survey of jail inmates (N=6,953) reported high prevalence of mental illness, substance abuse, previous arrests, and prior episodes of homelessness (
4). As far back as 1996, the U.S. Department of Justice estimated an annual cost of $14 billion to treat incarcerated people who had a diagnosis of schizophrenia or bipolar disorder (
5).
Studies and statistics in regard to incarcerated persons with mental illness have generally been reported from the correctional system's perspective. Less is known about rates of and risk factors for incarceration and reincarceration of people in public mental health systems. This is important because most public mental health patients live in the community and a key goal is to help them live in the least restrictive settings possible. In a 2003 National Alliance on Mental Illness survey, 40% (N=2,300) of mental health consumers reported having been arrested because of their psychiatric symptoms (
6). Among a random sample of Los Angeles public mental health system patients (N=6,624), 24% had been incarcerated over a ten-year period (
7). Although methods and results vary, the reported numbers of incarcerated patients raise serious concerns. Reducing criminalization of persons with mental illness has thus become an important concern for both criminal justice systems and mental health systems (
3).
Another closely related focus has been on improving mental health services during and after incarceration. Whereas contextual stressors inherent to the criminal justice system may increase risk of psychiatric decompensation (
8), major impediments to systemic improvement in care are the different cultures and objectives of the mental health and criminal justice systems (
9). These differences result in a delicate balance between concerns for public safety and individual rights (
10). Although jails are legally obligated to provide mental health care for inmates (
11), their primary purpose is protecting public safety. Nonetheless, jails are frequently the de facto mental health system for many individuals (
3), leading to calls for additional resources in both the criminal justice and mental health systems (
3,
12).
Given the substantial prevalence of mental illness among incarcerated individuals, more research is needed to identify mechanisms that reduce the flow of patients into the criminal justice system and minimize reincarceration and other adverse outcomes after release. Our research contributes to this goal through its assessment of the prevalence of and risk factors for incarceration, reincarceration, and short-term outcomes after release from incarceration.
Our hypotheses were informed by studies that investigated factors associated with increased incarceration risk for persons with mental illness. Cuellar and colleagues (
7) found that patients who were younger, male, or African American were most likely to be arrested and that persons with bipolar disorder had higher arrest rates than those with depression. Similarly, a ten-year prospective investigation of 13,816 persons with severe mental illness in Massachusetts noted that male gender, younger age, and racial-ethnic minority status were associated with increased incarceration risk (
13). A cross-sectional study of 236 patients in San Francisco noted that substance use and homelessness, but not gender or race-ethnicity, were associated with history of incarceration (
14).
On the basis of this research, we developed and tested three hypotheses. First, incarceration will be associated with prior incarceration, younger age, male gender, racial-ethnic minority groups, co-occurring substance-related diagnoses, lack of Medicaid insurance, schizophrenia diagnosis, and homelessness. Although many of these measures have been included in previous studies, they have not been included together in one model, and we found no studies that included Medicaid as a measure. Second, reincarceration would be associated with the same demographic and clinical measures as incarceration and also with felony index arrest, longer index incarceration, and the first type of service received after release from incarceration.
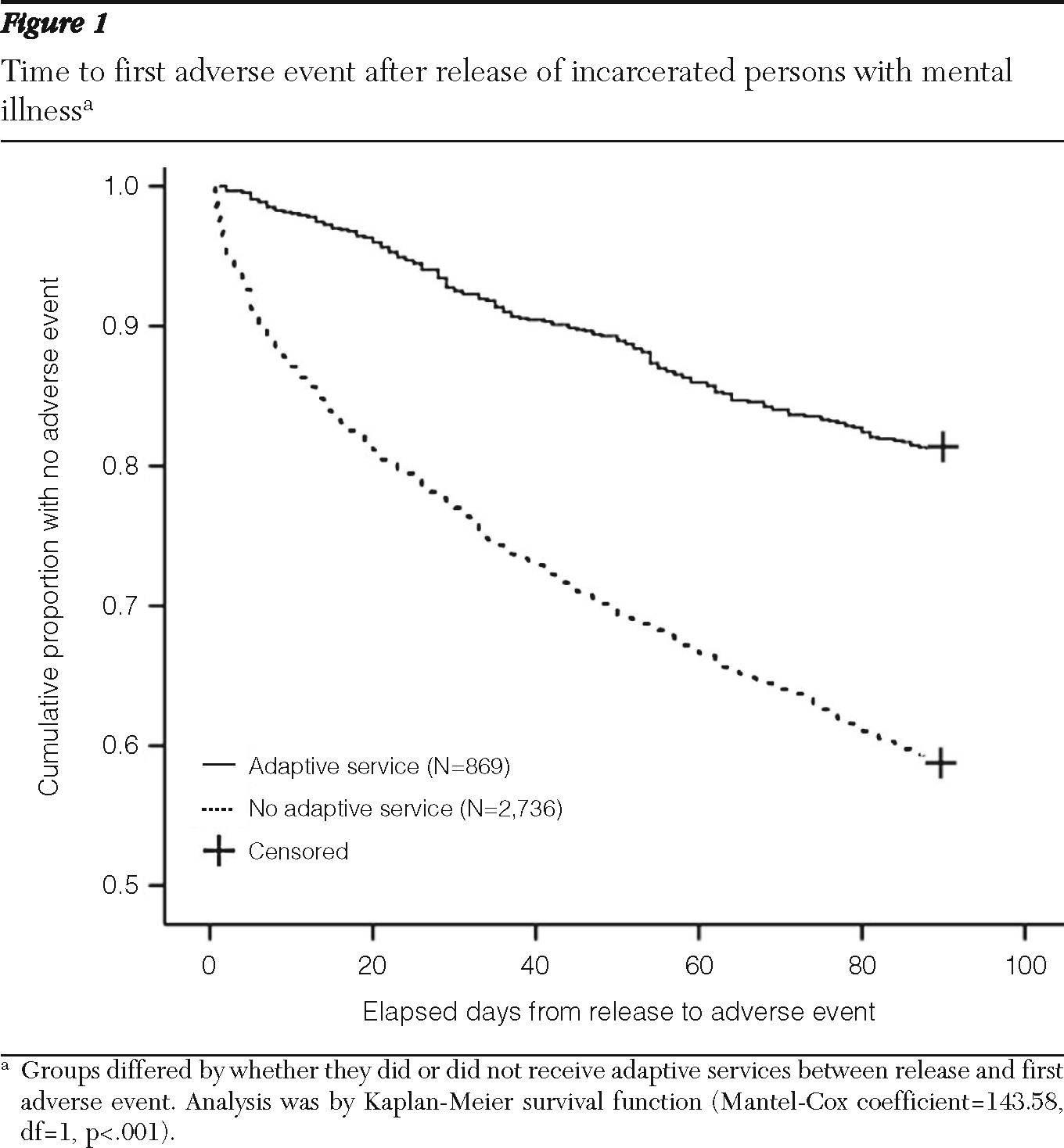
The third hypothesis posited that among patients who were incarcerated, those who received adaptive services (such as outpatient services or case management) after release would have more days in the community before the occurrence of an adverse event (such as emergency mental health services or reincarceration) and would have fewer adverse events during a 90-day follow-up period compared with those who did not receive an adaptive service after release. Because we found no studies reporting risk factors for reincarceration or using survival analysis to evaluate short-term outcomes after incarceration, the measures in the second and third hypotheses were included on the basis of preliminary bivariate analyses.
Methods
San Diego County, the fifth most populous county in the United States, is on the border between the United States and Mexico and has a diverse racial-ethnic composition. According to the 2009 U.S. Census, non-Hispanic Caucasians constitute 50.4%, Latinos 31.3%, African Americans 5.6%, and Asians 10.4% of the San Diego adult population (
15). Each year, the San Diego County Sheriff's Department books about 100,000 people into six county jails.
This study used data from the San Diego County Adult and Older Adult Mental Health Services (AMHS) system and the San Diego County Sheriff's Department. This data set linked adult psychiatric patients who received at least one AMHS service in fiscal year (FY) 2005–2006 with incarceration records from the Sheriff's Department Jail Information Management System (JIMS). Limited data were also extracted from the AMHS and JIMS databases from FY 2004–2005 and FY 2006–2007 in order to retrieve service use data before and after incarceration and for incarceration records one year before and after the first incarceration in FY 2005–2006.
The first incarceration in the fiscal year was designated the index incarceration from which service use and incarceration events were measured forward and backward in time. Service utilization and reincarceration after release from the index incarceration were grouped into two broad categories: “adaptive” or “adverse.” Adaptive services included organizational and fee-for-service outpatient and intensive and traditional case management. Adverse service events included psychiatric hospitalization, crisis residential admission, contact with the Psychiatric Emergency Response Team or the county-operated psychiatric emergency department, and reincarceration. Although such adverse services may be helpful to patients, for the purposes of this study, admission to such intensive, crisis-oriented services after release from incarceration was considered an undesirable outcome. Persons with a mental illness who received an adaptive service before any adverse service events occurred after release from their index incarceration were coded into a dichotomous variable. Co-occurring substance-related diagnosis, homelessness, and Medicaid insurance were coded as present if recorded at any time during the fiscal year. The study was approved by the following institutional review boards: University of California, San Diego; AMHS; Veterans Affairs San Diego Healthcare System; and the Office of Human Research Protection of the U.S. Department of Health and Human Services.
We used bivariate analyses (t tests and chi square tests) to compare the demographic and clinical characteristics of incarcerated and nonincarcerated patients. We examined our first hypotheses about incarceration risks by using multivariate logistic regression. Variables (and reference group) included homelessness (domiciled), sex (female), race (Euro-American), diagnostic category (major depression), age group (18–29, 30–44, 45–65, and 65 and older, with 18–29 used as the reference group), Medicaid (uninsured), substance-related diagnosis (none), and prior incarceration (none).
We examined our second hypothesis about risk of reincarceration by performing another multivariate logistic regression analysis. This analysis included the same variables listed above and added receiving (or not) postrelease adaptive services, felony arrest for index incarceration (or not), and length of index incarceration (four days or more). The dependent variable, reincarceration, included only reincarceration episodes in San Diego County jails within one year of release from the index incarceration.
Finally, we used multiple strategies to examine our third hypothesis, which focused on service use and adverse outcomes during the critical transition period after release from jail. We used the Kaplan-Meier survival function to examine unadjusted time to an adverse event during a 90-day follow-up period for persons with a mental illness who received an adaptive service after release from the index incarceration compared with those who did not. We then used Cox regression to evaluate the strength of the findings after adjustment for other variables in the model. Days in the community before an adverse event were compared with a median test. To ensure a 90-day postincarceration follow-up period, only persons with a mental illness and with index release dates during the first three quarters of the fiscal year were used in this analysis.
Results
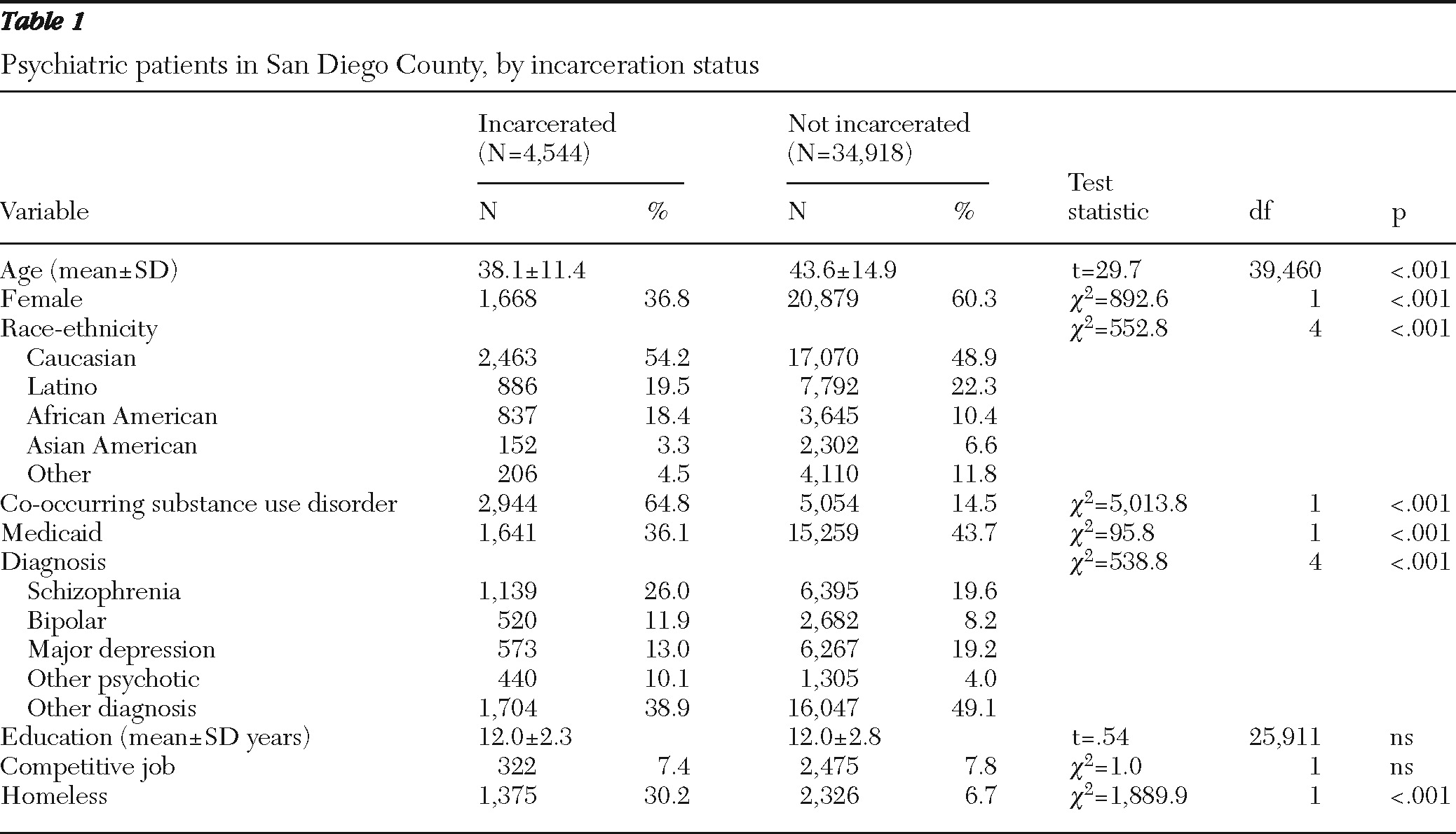
There were 39,463 unique adults with a mental illness in the data set, of whom 4,544 (11.5%) were incarcerated during the fiscal year. Of those incarcerated, 1,203 (26.5%) were reincarcerated within a year. Felony arrests accounted for 26.1% (N=1,184) of index incarcerations. The median length of incarceration was three days (mean±SD 21.0±46.7 days). Of the 4,544 incarcerated psychiatric patients, 280 (6.2%) received inpatient services and 2,733 (60.1%) received outpatient services while incarcerated.
Table 1 shows demographic characteristics for incarcerated and nonincarcerated patients.
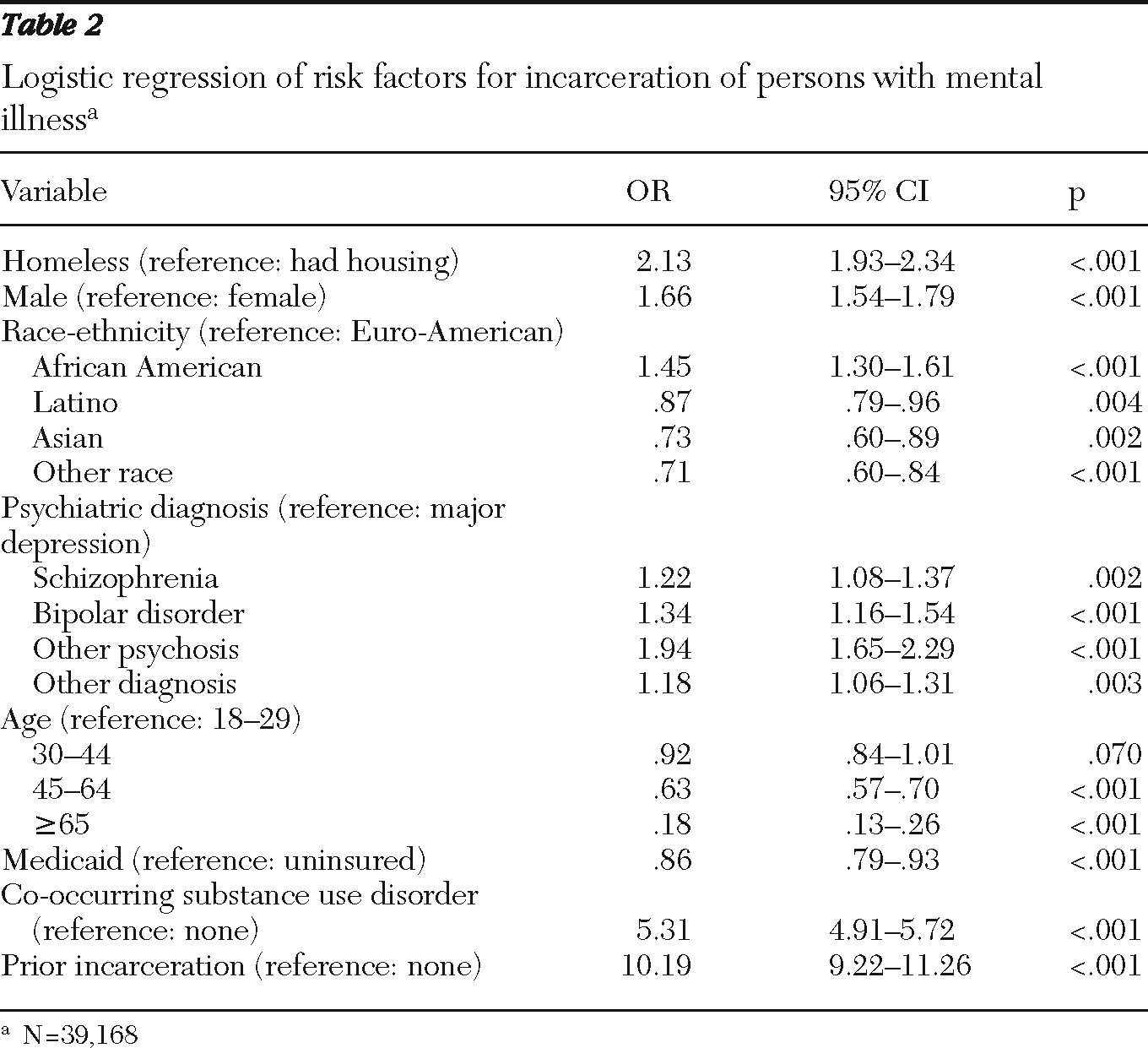
As shown in
Table 2, our first hypothesis was largely supported. Persons with a prior incarceration during the previous year had ten times greater odds of being incarcerated than those without prior incarceration. Patients with substance-related disorders in addition to their mental disorder had five times the odds of incarceration as patients without such co-occurring disorders. Homeless patients had twice the odds of being incarcerated as their domiciled counterparts. Compared with patients with major depression, patients in the “other psychosis” category had nearly twice the odds of incarceration, whereas those with schizophrenia or bipolar disorder had only somewhat elevated odds. Compared with Euro-Americans, African Americans were more likely to be incarcerated, whereas incarceration was less likely for Latinos, Asians, and other racial-ethnic minority groups. Compared with younger patients (ages 18–29), patients between 45 and 64 were less likely to be incarcerated and patients 65 and older were unlikely to be incarcerated. Men were more likely than women to be incarcerated. Medicaid beneficiaries were less likely than uninsured patients to be incarcerated.
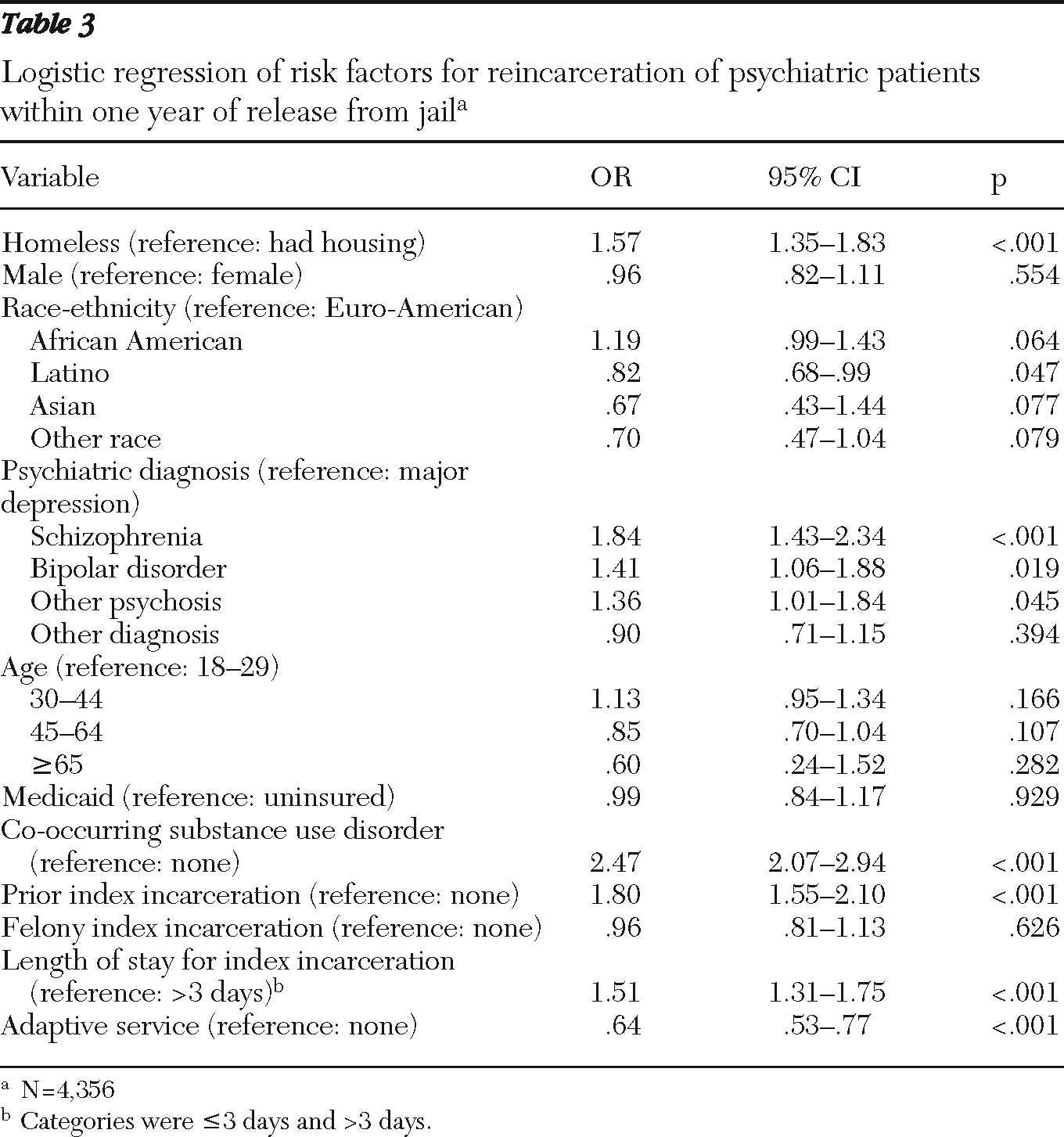
As shown in
Table 3, our second hypothesis, about reincarceration risks, was partially supported. Patients with co-occurring substance-related disorders had more than twice the odds of reincarceration within the following year as patients without substance disorders. Patients with prior incarcerations had nearly twice the odds of reincarceration as those without prior incarcerations. Homeless patients were more likely to be reincarcerated than their housed counterparts. Compared with patients with major depression, patients with schizophrenia or bipolar disorder were more likely to be reincarcerated. Patients who received an adaptive service after release were less likely to be reincarcerated than patients who did not. Contrary to our hypothesis, patients with a length of incarceration of three days or fewer had 1.5 times the odds of reincarceration compared with those incarcerated longer. Medicaid status, age, race-ethnicity, and gender also did not have the hypothesized association.
Our third hypothesis was supported.
Figure 1 shows the unadjusted results of the Kaplan-Meier survival function. Robust differences were found between patients receiving adaptive services between release from the index incarceration and an adverse event compared with those who did not. Overall, patients who received an adaptive service following release experienced proportionally fewer adverse events within 90 days compared with those who did not (adaptive service, N=164, 18.9%; no first adaptive service, N=1,134, 41.4%;
χ2=145.8, df=1, p<.001). A comparison of time to adverse events in each group found that the adaptive-services group demonstrated more time in the community before an adverse event occurred (median time to adverse event=36.5 days compared with 22.0 days for those not receiving an adaptive service: median test,
χ2=25.0, df=1, p<.001). For the adaptive service group, the median time between release from jail and receiving the first adaptive service was 17 days. To further examine the function of time, we focused on the steepest part of the curve, which fell into the first two weeks during which 38.7% (N=439) of patients who did not receive adaptive services following release experienced an adverse event, compared with 14.6% (N=24) of those who received an adaptive service (
χ2=36.2, df=1, p<.001). Adaptive services remained an important factor even after adjustment for variables associated with reincarceration.
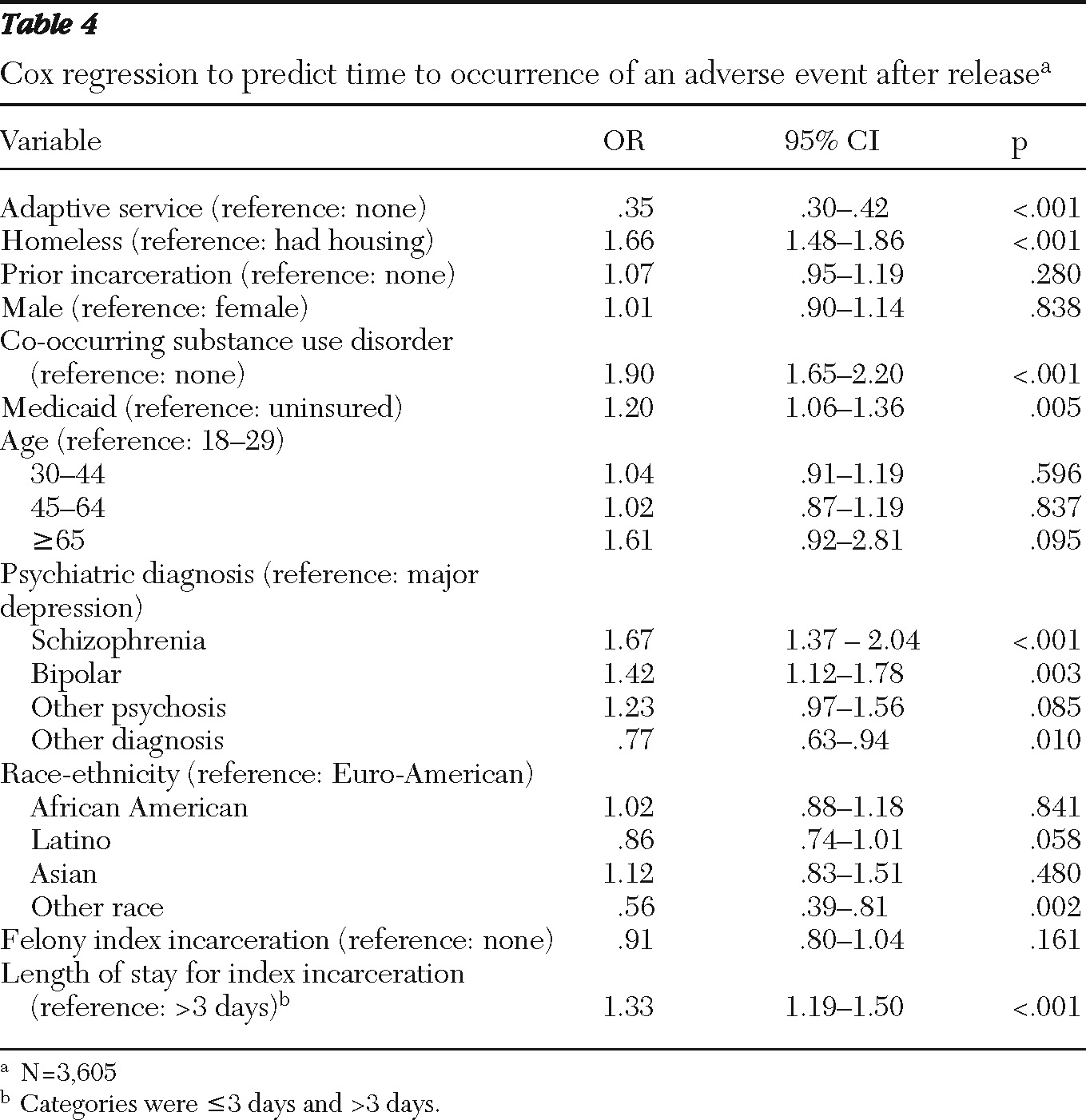
Table 4 shows the Cox regression results. Patients who received an adaptive service after release were less likely to experience subsequent adverse events compared with patients who did not. Patients with co-occurring substance-related disorders had nearly twice the odds of having an adverse event as those without substance use disorders. Compared with Euro-Americans, racial-ethnic minority groups other than Latino, African American, or Asian were less likely to experience an adverse event. Homeless patients were more likely to experience an adverse event than their housed counterparts. Compared with patients with major depression, patients with schizophrenia or bipolar disorder were more likely, and patients with other diagnoses less likely, to experience an adverse event. Patients with index incarcerations of three days or fewer were more likely to experience an adverse event than patients incarcerated longer. Although it is contrary to our hypothesis, this finding is consistent with the findings of our reincarceration analyses.
Discussion
This study found that 11.5% of public mental health patients were incarcerated during a one-year period. Our finding is difficult to compare with the aggregate 24% reported by Cuellar and colleagues (
7) for a ten-year period. Their study used a relatively small random sample (N=6624) and examined arrests across a ten-year period, whereas our study examined incarcerations and included all patients over a one-year period. Nonetheless, both studies suggest a substantial overlap between the public mental health and jail systems. We also found that 26.5% of incarcerated patients were reincarcerated within a year. We found no studies in the literature reporting the proportion of public mental health patients reincarcerated with which to compare our findings.
Fisher and colleagues (
13) reported that ethnic minorities had an increased incarceration risk, whereas White and colleagues (
14) found no association between ethnicity and incarceration. Our results suggest that compared with Euro-Americans, persons from Latino, Asian, and other racial-ethnic minority groups were less likely to be incarcerated, whereas African Americans were at greater risk. As hypothesized, schizophrenia was a risk factor compared with major depression. Inconsistent with our hypotheses, bipolar disorder and other psychoses were also found to be risk factors, although the finding for bipolar disorder is consistent with Cuellar and colleagues' findings (
7).
As we hypothesized, patients who received an adaptive service after the index incarceration were less likely to experience an adverse event, including reincarceration, within 90 days. In addition, patients who received an adaptive service and then had an adverse event spent more days in the community before the event occurred. This finding suggests that receiving timely outpatient and case management services after release may help lower the risk of adverse events such as emergency services or reincarceration.
Contrary to our hypothesis, patients with a one- to three-day index incarceration were more likely to be reincarcerated than those incarcerated longer. This finding could be due to the overrepresentation of homeless and substance-abusing patients, who are at high risk of reincarceration, among those with a shorter index incarceration.
Several of these findings have implications for factors that are potentially modifiable, including homelessness, substance abuse or dependence, lack of medical insurance, and time to adaptive services after incarceration. Most of these factors could be at least partially addressed by changes in priorities and procedures within public mental health and jail systems. The overrepresentation of homelessness and co-occurring substance use disorders among incarcerated and reincarcerated patients underscores the need to better address these major public health challenges.
The strengths of our study include reporting from the perspective of a large public mental health care system and county jail system with a large sample, including patients with a range of diagnoses; estimating risk factors for incarceration and reincarceration on the basis of demographic, clinical, service use, and incarceration measures over a one-year period; and including survival analyses that examined elapsed time from release from the index incarceration to receipt of services.
There are also limitations that should be kept in mind when interpreting our results. Our study design allows only associations, from which no interpretation of causation can be reported. We used an administrative database that did not include medication adherence, physical illnesses, housing status, employment status, significant relationships, and other potentially important patient-level measures that may have influenced outcomes. Therefore, although we included available patient characteristics in the analyses, a portion of the beneficial association found for patients who had a timely outpatient visit after incarceration may be due to other patient-level factors.
In addition, it should be recognized that part of the association between adaptive service use and time to an adverse event may be structural, rather than causal. Persons who received adaptive services, by definition, had not experienced an adverse event up until that point. In this observational study, adaptive service use was in part a marker of having been in the community for a longer period without an adverse event, so adaptive service use may be considered a proxy for greater time without an adverse event. Because the dichotomous measures of homelessness, co-occurring substance-related diagnoses, and Medicaid insurance did not include dates of occurrence, these events may have preceded or followed the index incarceration, which could have affected results. In addition, substance-related diagnoses were likely understated in the data. However, findings reported were consistent with other studies documenting the high proportion of substance use disorders among incarcerated patients (
4).
Also, diagnoses were made by community clinicians and thus may not be as accurate as those derived from diagnostic research instruments. Personality disorders were not included because of missing data, which may have influenced results. Our data did not include state or federal prison system records. Finally, because San Diego County did not have diversion programs during the time of our study, we were not able to explore the influence of such programs, which have demonstrated success in reducing incarceration (
16,
17).
Conclusions
In conclusion, incarceration is a serious problem among patients treated in public mental health systems and is associated with some potentially modifiable factors. On the basis of this study, we offer two recommendations for consideration by public mental health and criminal justice systems. First, experiment with an expedited access policy for released patients to understand whether early adaptive service use leads to reductions in reincarceration, and second, reduce risks of incarceration by focusing on modifiable risk factors, such as homelessness, lack of Medicaid insurance, and substance use problems. As a result of these findings, policy makers for San Diego County AMHS implemented an expedited access procedure so that any public mental health patient released from jail must be seen within 72 hours at any AMHS-funded outpatient program in the county. This demonstrates the responsiveness of this county's mental health system and jail system to the needs of patients.
Patients in the public mental health system represent one of the most vulnerable and disadvantaged segments of society. Additional prospective research is needed to further examine issues addressed in this study and to design, implement, and evaluate interventions to reduce incarceration and reincarceration in this at-risk population.
Acknowledgments and disclosures
This work was supported, in part, by grant MH080002 from the National Institute of Mental Health and by the Advanced Center for Innovation in Services and Intervention Research, University of California, San Diego.
The authors report no competing interests.