Mania, characterized by elevated, expansive, or irritable mood with inflated self-esteem or grandiosity, decreased need for sleep, pressure of speech, flight of ideas, distractibility, general overactivity, and agitation, usually occurs as part of a bipolar affective disorder (BAD) and is regarded as a disorder of unknown etiology.
1 This condition is classified as primary or idiopathic mania. By contrast, secondary mania is due to the direct physiological effects of medical conditions, metabolic disturbances, infections, or cerebral neoplasms, or to pharmacological antecedents including illicit drugs.
2–6 Secondary mania differs from BAD in having a later age of onset and no family history of the illness.
7Several authors have described mania in patients with human immunodeficiency virus (HIV) infection. Most reports,
6–12 but not all,
6,12,13 have documented an association with the development of cognitive impairment and evidence of structural brain damage, demonstrable by CT or MRI scan. Family and personal history of mania have been examined as potential contributory factors. Some case reports have noted an association between mania and zidovudine
8,14,15 or didanosine (ddI)
16 therapy. Both ethambutol
17 and clarithromycin
18 have been reported to be associated with manic episodes in the setting of therapy for
Mycobacterium avium complex in individuals with advanced acquired immunodeficiency syndrome (AIDS).
Lyketsos et al.
19 have described a mania syndrome in association with advanced HIV disease. Compared with people in whom mania occurs as part of BAD, patients with AIDS-associated mania were less likely to have a personal or past history of mood disorder. These patients had a different symptom profile (more irritability and increased talkativeness) and higher rates of HIV-associated neurocognitive disorders (dementia and cognitive slowing as measured by performance on Grooved Pegboard). These authors have proposed that this entity, which they label “AIDS mania,” is directly related to the pathophysiology of HIV brain infection.
We hypothesized that if this is so, then antiretroviral agents that penetrate the cerebrospinal fluid (CSF) may offer some protection from incident mania, and AIDS dementia complex will occur more frequently in patients with mania secondary to HIV infection. In order to test our hypothesis and examine the contribution of other factors reported to be associated with mania, we undertook a case-control study in a population of HIV-infected individuals.
METHODS
Fairfield Hospital, Melbourne, a 138-bed infectious diseases hospital, established an HIV treatment service in 1984. Of 2,135 HIV-infected patients managed, 1,553 attended between October 1992 and June 1995. The Consultation-Liaison Psychiatry Service established in October 1992 provided treatment for inpatients, ambulatory patients, and those referred by community medical practitioners. All patients referred to the HIV psychiatry service over 33 months were screened for the presence of manic symptoms. A consultant psychiatrist (F.K.J.) confirmed the diagnosis of mania (DSM-III-R criteria) by clinical review of symptomatic patients.
Secondary mania was diagnosed according to a modified form of the criteria of Krauthammer and Klerman.
7 Secondary mania was diagnosed in patients with 1) no clear prior personal or 2) family history of affective disorder (depression or mania) in whom the syndrome 3) postdated the diagnosis of HIV infection (the best available approximation of the Krauthammer and Klerman criteria of “close temporal proximity to injury/illness”). The fourth criterion, late age of onset, was not applied. Patients with confusional symptoms (acute brain syndrome) were excluded.
During this period, antiretroviral therapy was prescribed for patients with CD4 cell counts below normal (<500/ml); ddI or zalcitabine (ddC) was added if the patient showed recurrent symptoms and/or a 50% fall in CD4 count.
Twenty-three patients with first-episode mania were identified. Of these, 19 had secondary mania, 2 had long-standing histories of BAD (manic symptoms in each antedating HIV infection), and 2 had depression predating this manic episode. No patient had a prior diagnosis of AIDS dementia complex.
For the manic patients' data regarding current illness, past personal and family psychiatric history were elicited by interview with the treating psychiatrist, and routine screening was performed for organic pathology in addition to HIV infection (thyroid screen, illicit drug screen, cerebral CT scan). For both patients with mania and control subjects, sociodemographic data, details of medical history, current CD4 count, current treatment, current and past antiretroviral therapies, head CT/MRI scan, serological results for cytomegalovirus (CMV), Toxoplasma gondii, and Treponema pallidum were obtained from review of the medical record.
Control patients were selected from patients with HIV infection attending the hospital over the same period of study. They were identified by computer search of CD4 cell count results matching control subjects to patients with mania by age (year of birth), CD4 count (±30/ml), and date of treatment (±6 months). For each case, a potential list of control subjects was established according to the above parameters. Three control subjects were identified by selecting from the list of consecutive patients attending the hospital at the time of interest. If two duplicate control patients were selected, they were replaced by the next potential control on the list. In all, 39 of 57 control patients (68.4%) were found to have undergone prior review by the Consultation-Liaison Psychiatry Service. This was not unlikely, since 16.7% of all patients hospitalized during this period were referred to the C-L Psychiatry Service each admission and patients with AIDS had the highest referral rate.
20 None of these control patients was diagnosed with mania or other psychiatric illness at or prior to assessment.
In May 1998, a follow-up review of the hospital database of AIDS-defining illness, including mortality data, was undertaken, and data were collected on patients with mania and control subjects. At this review, data were collected for both cases and control subjects relating to occurrence of mania or depression as well as diagnosis of AIDS dementia complex, date last reviewed, and date of death for those who had died.
Odds ratios and confidence intervals were estimated by McNemar method in order to test the strength of any apparent associations. Two-sided significance levels (P-values) against the null hypothesis of no association were obtained. Epiinfo6 (Centers for Disease Control and Prevention Database and Statistics Program for Public Health, version 6.02) and SPSS (Statistical Package for Social Sciences) were used for the multivariate analysis. Kaplan-Meier analysis and Cox proportional hazard estimates of dementia-free survival were undertaken. A power calculation based on an assumed difference of 15% between the groups and an estimated sample size of 15 showed that 2.5 control subjects were needed per case for an 80% power.
RESULTS
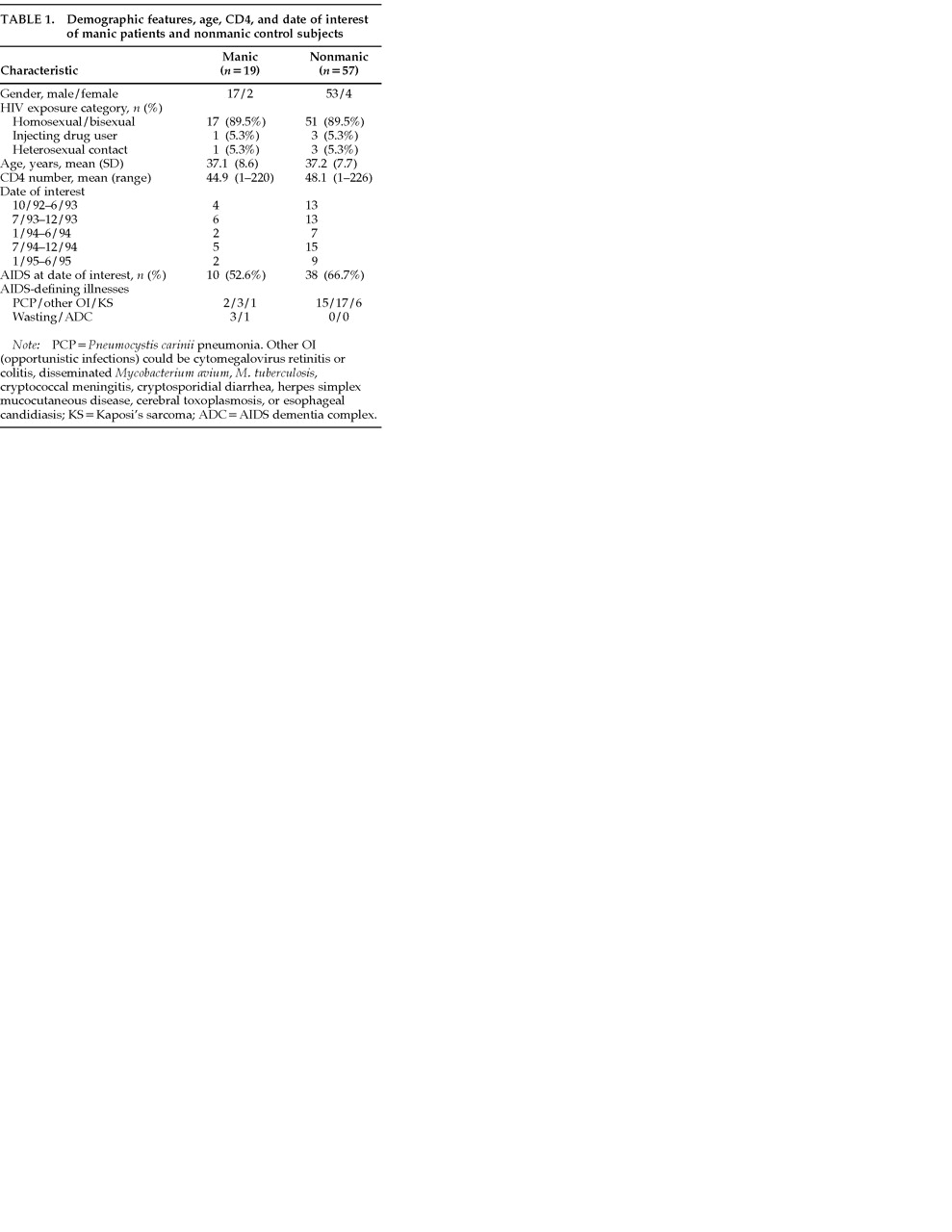
During the 33 months, 19 patients with secondary mania fulfilling the case definition were identified. Demographic features and factors upon which matching occurred are shown in
Table 1. These patients were significantly disabled, were ill for a mean of 20 days (4 to 60), and had a mean of 4.6 symptoms per patient; 18 required inpatient admission, 4 as involuntary patients; 7 of 19 patients experienced delusions, and 1 other patient without delusions required almost continual supervision because of behavioral disturbance. Thus, 8 had severe mania as defined by DSM-III-R.
1Neither the proportion with AIDS
21 nor the type or frequency of AIDS-defining illnesses (ADIs) differed significantly between the cases and control subjects (
Table 1). At the diagnosis of mania no patient had cerebral toxoplasmosis, cerebral lymphoma, or cryptococcal meningitis. Disseminated
Mycobacterium avium complex disease had not been diagnosed in any patient with mania and was present in 2 control patients.
All patients with mania were questioned about recent drug use, and none was using illicit drugs prior to mania diagnosis. Two patients with mania (10.5%) and 8 control patients (14.8%) were recorded as ever having used illicit drugs. Examination for prescribed medications revealed that 2 patients with mania and 8 control subjects were receiving antidepressants. The patients with mania were taking amitriptyline 50 mg/day for treatment of peripheral neuropathy (one for 6 months, the other for 12 months). The prescription of other drugs with potential to cause mania did not differ significantly: cases/control subjects: acyclovir, 8/24; glucocorticoids, 1/6; isoniazid, 2/2; ethambutol, 0/2; clarithromycin, 0/0; benzodiazepines, 4/14.
Neuroimaging (CT and/or MRI) was performed within 6 weeks in all patients with mania. Nine were reported as normal, 5 showed mild cerebral atrophy, and 5 showed high T2 signal foci, of whom 1 also revealed a porencephalic cyst (of doubtful significance clinically). CT head scans within 3 months of the date of interest were available for 10 of 57 control subjects; 8 were normal, 1 showed mild cerebral atrophy, and 1 showed evidence of progressive multifocal leukoencephalopathy. All patients with mania underwent lumbar puncture, and no opportunistic infection or malignancy was diagnosed.
Four of 19 patients with mania (21.1%) and 46 of 54 nonmanic control subjects (80.7%) were recorded as receiving zidovudine therapy at the date of interest. “Any” prior zidovudine therapy was recorded in 13 of 19 manic patients (68.4%) and in 54 of 57 nonmanic control subjects (94.7%). The odds ratios and 95% confidence intervals (CI) for these associations are shown in
Table 2. For those receiving zidovudine, no difference in mean duration of zidovudine treatment was demonstrated between patients with mania and control subjects (
P=0.35). Among those in the manic group who had ceased zidovudine, the mean time since ceasing zidovudine was 1.5 years (median 1.1 years).
No significant difference in gender distribution (92.5%/88.8% male), mean age (36.3 years/38.2 years), median CD4 number/ml (16/26), or proportion with AIDS (80.3%/88.8%) between those 67 individuals ever receiving zidovudine and the 9 never treated with zidovudine was identified.
ddI therapy was used by 7 of 19 mania patients and 29 of 57 control subjects prior to or at the date of interest, and ddC was used by 3 and 16, respectively. No significant difference between patients with mania and control subjects was demonstrated.
Serological evidence of prior exposure to potential cerebral opportunistic infections did not differ significantly between manic patients and nonmanic control subjects (for T. gondii, 50% vs. 35%; CMV, 95% vs. 98%; and syphilis, 15.8% vs. 9.6%).
Mean corpuscular volume (MCV) as a surrogate marker of adherence to zidovudine therapy was recorded for 14 manic patients and 45 nonmanic control subjects within 3 weeks of date of interest. Mean MCV at the date of interest in manic patients was 90×10–15/l and in nonmanic patients 96.8×10–15/l (P=0.02). There was a significantly higher MCV among those recorded as taking zidovudine compared with those not taking it at the date of interest (98.3 vs. 89.1×10–15/l; P=0.008), suggesting that patients were compliant with zidovudine dosing.
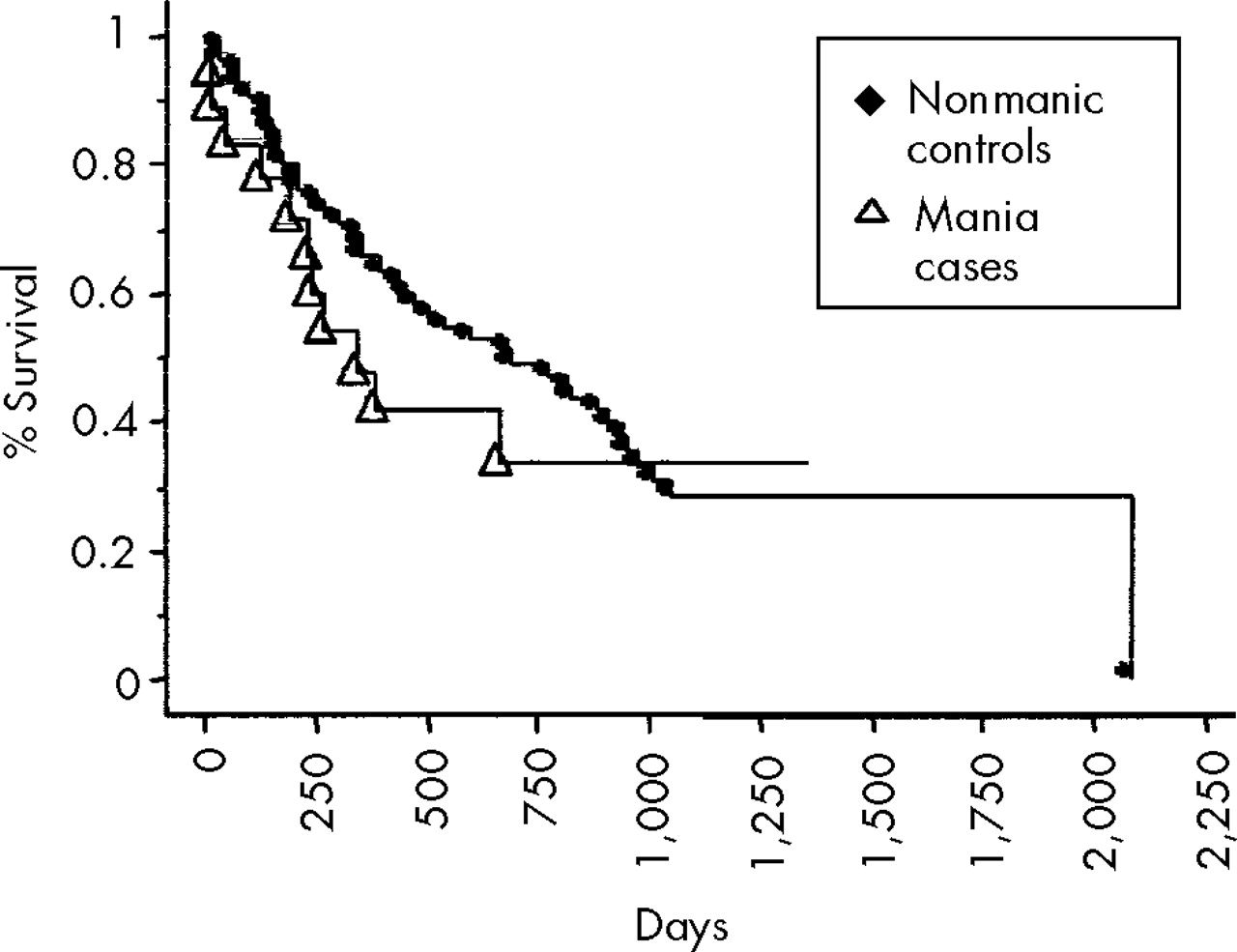
Follow-up in February 1998 showed that of 15 cases where information was available, 2 patients (13%) had experienced a recurrent episode of mania and 2 (13%) had been diagnosed with depression. Among the control group, 8 of 56 had been recorded as having developed depression (14.3%). No control patient was recorded as developing mania. AIDS dementia (as defined by Centers for Disease Control and Prevention criteria) was diagnosed in 2 of 15 patients with mania, at a median of 3.1 months, and in 1 of 56 control subjects, at a median of 2.7 months following diagnosis. Odds ratio was 27 (95% CI 6.7 to 108). Nine patients with mania and 19 control patients had died by February 1998. Median survival of the patients with mania was 7.9 months and of control subjects, 13.5 months. Kaplan-Meier analysis showed no significant survival difference between groups (
Figure 1).
DISCUSSION
We found, as previously reported, that mania developed in patients with advanced HIV disease, a mean CD4 count of 44.9 cells/ml, and prior AIDS-defining illnesses (52.6%). Any of the patients seen could have been experiencing first-episode BAD, but use of the Krauthammer-Klerman criteria makes this less likely.
No association between mania and progression to AIDS, type of ADI, or structural CNS lesions on CT/MRI scan was found. Indeed, CNS opportunistic infections were only recorded among control subjects, reducing the likelihood of these causing mania. No drugs other than antiretrovirals were significantly more common among mania patients than among control subjects without mania. The demographic data showed intravenous drug use as an HIV exposure category equally represented in patients with mania and control subjects, but “any prior illicit drug use” was more commonly recorded among control subjects. This difference did not reach statistical significance, and any associated bias would act against access among control subjects to treatment for HIV.
Examining treatment for HIV infection revealed a significant difference between the control patients and the cases with mania. The patients with mania were significantly less likely to be receiving concurrent zidovudine or to have previously received treatment with zidovudine. For zidovudine therapy used at the time of interest, the protection against mania was 14.3-fold (95% CI: 3.7 to 100-fold). For “any prior zidovudine therapy,” the protection was 5.9-fold (95% CI: 1.5 to 33-fold). This effect was not present with ddI or ddC, neither of which penetrates the cerebrospinal fluid well. The apparent protective effect of zidovudine existed despite a lack of any demonstrable association of mania with concurrent or previous AIDS illness. Zidovudine is not known to exert any direct antipsychotic activity; in fact, the opposite has been suggested.
8,14,15Follow-up showed that significantly more patients with mania, compared with control patients, were recorded as having ADC. This difference was present despite no significant difference in overall survival.
We acknowledge a number of potential biases and limitations of this case-control study. Misclassification bias because of the differential examination rates of mania patients and control subjects by the Consultation-Liaison Psychiatry Department is possible (all patients with mania, but only 68% of control subjects, were examined) and could have resulted in control subjects having undiagnosed mania. However, we believe the condition to be difficult to miss; moreover, such a misclassification (undiagnosed mania among the control subjects), even if present, would have reduced rather than increased the demonstrated protective effect of the zidovudine.
Selection of control subjects from the same hospitalized patient population might have been inappropriate if the manic patients had been referred to the hospital because of their mania and control subjects were already recorded as patients. However, we examined the referral source of mania patients and control subjects and found that, with one exception, all patients with mania were attending the service prior to the diagnosis and that the same referring primary care doctors were represented among both groups.
The review of medical records was undertaken with prior knowledge of the mania status of the cases and control subjects. Differential recording of antiretroviral therapy in the medical record, either because the investigators recalled the patient's status or because of their specific interest in the association, would have likely increased the proportion of mania patients rather than control subjects with antiviral therapy details. This should have weakened the association rather than increased it.
The association of mania with absence of zidovudine therapy could be due to some undiagnosed prior factor that made the patients at risk of mania less likely to accept zidovudine therapy. However, mania was an acute event occurring late in the course of HIV disease, a considerable time after zidovudine therapy was first indicated for treatment (CD4 count <500 cells/ml.). Furthermore, no specific personality type or coping style has been associated with mania. The presence of this type of confounder therefore seems unlikely.
The observed association between the development of mania and the absence of zidovudine therapy may indicate that mania occurs as a result of the neurotoxic effects of HIV, which are to some extent ameliorated in the zidovudine-treated group. Mean corpuscular volume analysis appeared to corroborate recorded zidovudine therapy, with higher MCVs in those recorded as receiving treatment. We found no evidence of concurrent opportunistic infection as a cause of mania, but other possible etiologic factors, including other undiagnosed infections or the effects of cytokines, cannot be excluded. Our study cannot distinguish mechanisms of this association between mania and zidovudine, and the possibility that zidovudine has a direct antimanic effect cannot be eliminated. However, considering that other authors have described the initiation of antiretroviral therapy as the precipitant for mania, this seems unlikely.
8,14–16 The apparent increase in ADC among the patients with mania further suggests some enhanced HIV neuropathology in this group and is in accord with the findings of Lyketsos et al.
19Prospective studies are required to examine further this association between the development of mania, evidence of active HIV replication (in CSF and periphery), and the use of antiretroviral medications, seeking possible etiological explanations and improved therapies for this condition.