Electroconvulsive therapy (ECT) is considered to be a safe and highly effective antidepressant treatment.
1 However, in some patients, ECT also results in temporary cognitive impairment, including anterograde and retrograde amnesia.
2,3 Prior research suggests that adjunctive pharmacological treatment
4,5 and modification of treatment parameters
6,7 may reduce adverse cognitive effects. Yet, reduction in cognitive impairment may be at the expense of clinical efficacy. Limited research has examined how individual differences influence cognitive impairment following ECT.
8Findings from research on a variety of disorders, such as Alzheimer's disease, Parkinson's disease, schizophrenia, and human immunodeficiency virus (HIV), have shown support for CR theory. Case in point, Whalley et al.
11 found that lower intellectual ability in childhood was associated with higher rates of late-onset dementia. The authors used data from a 1932 survey measuring the mental ability of the 1921 Scottish birth cohort. They determined that while early-onset dementia was not associated with lower childhood mental ability when compared with matched control subjects, the mental ability scores in children who eventually developed late-onset dementia were significantly lower than those of other Scottish children that were tested in 1932. Snowdon and colleagues
12 found evidence suggesting that higher verbal functioning in early life may protect against the clinical manifestation of Alzheimer's disease in middle and late life. Specifically, the authors found a correlation between the grammatical complexity of autobiographies written in early life and lower incidence of Alzheimer's disease in late life among a large group of nuns. Y. Stern and colleagues
13 uncovered evidence suggesting that in Alzheimer's disease, individuals with higher levels of education and higher occupational status were protected against earlier onset of memory impairment. According to Glatt and colleagues,
14 educational attainment may modify the risk of cognitive decline in Parkinson's disease. In patients with schizophrenia, Dwork and colleagues
15 proposed that increased sensitivity to the effects of aging could be related to decreased CR. R. Stern and colleagues
16 demonstrated that HIV seropositive individuals with lower CR (as operationalized by educational and occupational attainment and an estimate of premorbid IQ) had greater neuropsychological deficits than HIV seropositive individuals with higher CR. A limited number of studies have examined the effect of bilateral ECT on subtests of the Wechsler memory test.
17 Some have found that less educated individuals are more apt to develop a euphoric-hypomanic adaptation.
18 To date, no empirical investigation has examined the potential influence of CR on memory functioning following ECT.
Individuals who undergo ECT exhibit variable disruption of memory functioning, despite similar treatments.
2,3,6 This study examined the possibility that CR influences the variability in memory dysfunction that is associated with ECT treatment. The current context provides a rare opportunity to examine the same individuals before and after a treatment that may disrupt CNS functioning. Thus, the present study was a pseudoexperiment of the possible mediating effect of CR on acquired memory impairment. The construct of CR was operationalized using measures of educational and occupational attainment, two factors that likely contribute to CR.
13,19,20 We hypothesized that, on the basis of findings in other conditions with neuropsychological consequences, individuals with high CR would exhibit less memory impairment than individuals with low CR after the same number of ECT treatments.
METHODS
Subjects
Subjects for the present study were 50 patients who were treated with ECT at either a private psychiatric hospital or a university-affiliated medical center. Data from a portion of these subjects (
n = 21) were obtained from the database of a previously conducted study that involved a double-blind, placebo-controlled trial of thyroid hormone in the reduction of the cognitive side effects of ECT.
21 The 21 subjects from the study were assigned to the placebo condition; that is, subjects in the active thyroid hormone treatment group of that investigation were not included in the current investigation.
In addition to the existing data for the 21 subjects described above, data were collected prospectively for the present study from 29 consecutive patients scheduled to receive ECT at the same two facilities but were not participating in any other research study. All subjects from both sources (i.e., previous and prospective data) met DSM-IV
22 criteria for either major depressive disorder (
n = 44), bipolar disorder (depressed) (
n = 4), or schizoaffective disorder (depressed) (
n = 2). All were between the ages of 18 and 75 and had at least 6 years of education. Subjects were excluded if they had a history of head injury, neurodegenerative disease, other CNS disorders with associated cognitive impairment, or a score on the Hamilton Depression Rating Scale (HDRS, 17-item)
23 of less than 16.
All participants were treated with ECT three times per week following routine ECT procedures as suggested by the American Psychiatric Association (APA) Task Force on Electroconvulsive Therapy.
1 Subjects who missed two consecutive treatments or one treatment on two or more occasions were not included in the analyses. All ECT treatments were administered using a Mecta SR-1 device (Mecta Corp., Portland, Oregon, U.S.A.). All subjects received bilateral ECT using a constant-current, brief-pulse, bidirectional square wave stimulus. Seizure threshold was estimated at the first treatment session, with successive stimulus dosing performed using a titration method aimed at providing moderate suprathreshold stimulation. Routine pharmacologic agents administered during the procedure included methohexital (a short-acting anesthetic) and succinylcholine (a short-acting muscle relaxant).
Instrumentation
Because most studies on the memory deficits associated with ECT have indicated problems with the storage and rapid forgetting of verbal information, the current study employed the short story subtest of the Rand Memory Test to assess immediate verbal recall, delayed verbal recall, and forgetting.
24 This task is an oral short story, with immediate and delayed (30-minute) recall conditions. The short story subtest has five alternate forms. For the present study, all five forms were used, with the order counterbalanced across subjects at each testing session. The validity and reliability of this measure is described by Lezak.
25In order to establish that memory performance was not influenced by depressive symptomatology, depression severity was rated at baseline and following three treatments using the HDRS (17-items). Occupational classification was made using the Hollingshead Occupation Rating Scale, an index derived from sociological data that categorizes occupations into nine categories.
26Procedure
All subjects provided informed, written consent prior to participating in either the thyroid hormone clinical trial or the prospective data collection for this study. Baseline measures were obtained on all subjects between 1 and 3 days prior to the first ECT treatment. Each participant was tested a second time on these measures 1 to 3 days following the third treatment (i.e., after the third treatment but before the fourth). At the time of testing, examiners were blind to the subjects' CR scores.
Cognitive Reserve Scores
In the present study, the construct of CR was operationalized by a combination of educational level and occupational attainment. This combination of education and occupation was chosen in an effort to reduce possible bias that could have resulted from using educational level alone, since education may be affected by cultural, social, or economic factors, such as socioeconomic status and educational opportunites.
Level of education was defined as the total number of years of formal education completed by the time of testing. Level of occupational attainment was scored on a 9-point scale, according to the nine occupational classifications of the Hollingshead Occupation Rating Scale. To calculate CR scores, years of education and occupational rating were transformed into standardized z scores based on the means and standard deviations of these variables for the entire sample. The rank value of each z score was calculated to result in a CR score for each subject. The median CR score was then determined. Subjects whose CR score was above the median were classified as having high CR and those whose scores were at or below the median were classified as having low CR. This procedure yielded a low CR group consisting of 23 subjects (14 female, 9 male) and a high CR group comprised of 27 subjects (15 female, 12 male). Chi-square analysis of gender distribution among the two CR groups was not significant, suggesting that gender was not unequally distributed among them. As seen in
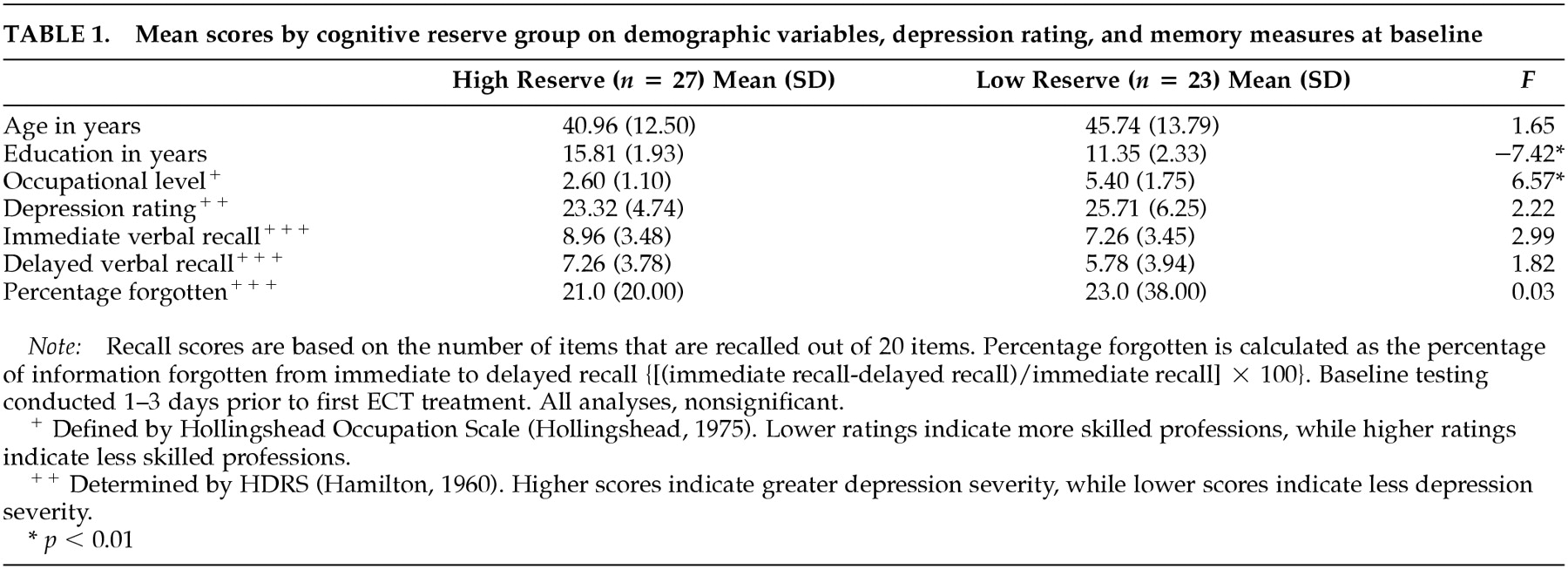
Table 1, the groups also did not differ significantly with regard to age or baseline depression severity, as measured by the HDRS.
Statistical Analyses
Between-group comparisons of the primary dependent variables at baseline were examined by one-way analyses of variance. Immediate verbal recall score, delayed verbal recall score, and forgetting [{(immediate recall − delayed recall)/immediate recall} × 100] of the Randt story were the dependent variables. To examine the potential impact of depression on memory performance at baseline, analyses of covariance with baseline depression score as a covariate were performed for each memory measure. Similarly, to examine the potential impact of age on baseline memory performance, analyses of covariance with age as a covariate were performed for each memory measure.
Between-group comparisons were conducted on memory scores following three ECT treatments (i.e., posttest) by one-way analyses of covariance, with the CR group as the independent variable, the three memory scores at posttest as the dependent variables, and the corresponding baseline memory scores as the covariates. In order to control for the potential impact of depression on memory performance at posttest, analyses of covariance for each memory measure were repeated with the corresponding baseline memory score and posttest HDRS score as covariates. To control for the potential impact of age on memory performance at posttest, the analyses of covariance for each memory measure were repeated, with the corresponding baseline memory score and age as covariates.
In addition, Pearson correlations were calculated at baseline and posttest to examine whether scores on each of the memory measures were associated with education, occupation, CR score, HDRS score, or age. To assess whether CR group membership influenced these correlations, these calculations were repeated for each CR group separately.
RESULTS
As seen in
Table 1, no significant group differences at baseline on immediate verbal recall, delayed verbal recall, or percentage of information forgotten were observed. Significant correlations were, however, found between baseline immediate verbal recall and years of education (
r = 0.32,
p < 0.05), occupation rating (
r = −0.32,
p < 0.05), and CR scores (
r = 0.35,
p < 0.05). Major correlations were also found between baseline delayed verbal recall and years of education (
r = 0.33,
p < 0.05), occupation rating (
r = −0.32,
p < 0.05), and CR scores (
r = 0.35,
p < 0.05). This suggests that the independent variables impacted the total amount of information that was initially encoded and recalled after a delay. However, no significant correlations were found between baseline
forgetting scores and years of education (
r = −0.21,
p = 0.15), occupation rating (
r = 0.17,
p = 0.23), or CR scores (
r = −0.21,
p = 0.15), suggesting that baseline
forgetting was not mediated by the independent variables.
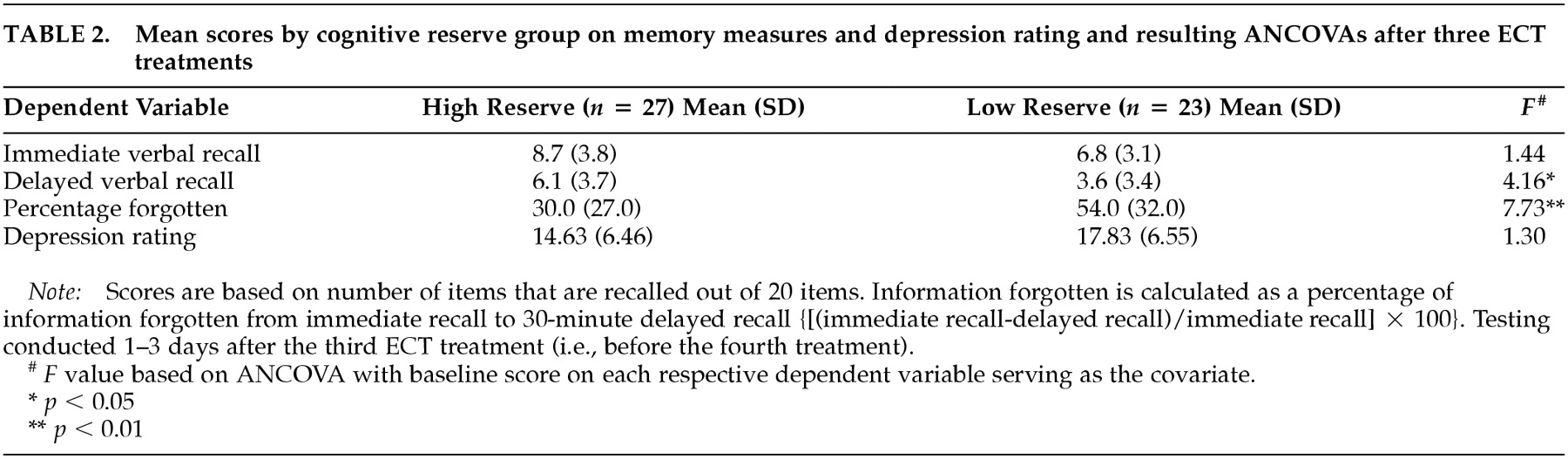
For delayed recall and percentage of information forgotten, significant between-group differences were observed at posttest between the two CR groups, as seen in
Table 2. The mean forgetting score of the low CR group was worse than the mean forgetting score of the high reserve group, indicating that after three treatments, the low CR group forgot considerably more verbal information than the high CR group after a 30-minute delay. The power achieved for this finding was 86%, assuming one-tailed analysis. In addition, no significant between-group differences were found between the two CR groups on immediate verbal recall after three ECT treatments, indicating that the high and low reserve groups initially encoded similar amounts of information from the short stories, further delineating this finding as a difference in retention rather than a difference in encoding.
Depression
The effect of depression (i.e., HDRS score) on memory measures was examined by way of a series of analyses. As reported above, analysis of variance (ANOVA) performed for the entire sample (
N = 50) at baseline revealed no significant differences between CR groups on HDRS scores. Analysis of covariance (ANCOVA) (with baseline HDRS score as covariate) performed for the total sample (
N = 50) at posttest also revealed no major differences between CR groups on HDRS scores (see
Table 2). This suggests that no significant effect of CR on depression scores at posttest occurred.
To assess whether depression influenced performance on memory measures at baseline, ANCOVAs with baseline HDRS score as a covariate were repeated for all memory measures. Results revealed the same pattern as originally reported. Specifically, no significant group differences on immediate recall (F = 1.43, df = 1,43, p = 0.24), delayed recall (F = 0.65, df = 1,48, p = 0.43), or forgetting (F = 0.02, df = 1,48, p = 0.90) were observed.
To assess whether treatment response influenced performance on memory measures at posttest, ANCOVA was repeated for all memory measures at posttest, with the posttest HDRS score added as a covariate (in addition to the respective baseline memory score). Results revealed the same pattern as originally reported. Specifically, no significant difference between groups on immediate recall (F = 1.25, df = 1,46, p = 0.27) was revealed, though substantial difference between groups on delayed recall (F = 4.66, df = 1,46, p < 0.05), and forgetting (F = 10.87, df = 1,46, p < 0.01) was found.
To further assess the relationship between HDRS score and memory performance, Pearson correlations were calculated for the entire sample at each time point. At baseline, immediate recall (
r = −0.43,
p < 0.01) and delayed recall (
r = −0.42,
p < 0.01), but not forgetting (
r = 0.20,
p = 0.16), were significantly correlated with HDRS score. This finding is consistent with previous research that has shown immediate learning and recall of information to be negatively affected by depression. Yet, depression may not significantly influence the amount of information forgotten over time.
27,28 At posttest, HDRS scores were not greatly correlated with any of the memory measures (
r = −0.20,
p = 0.17;
r = −0.09,
p = 0.53;
r = −0.15,
p = 0.29 for immediate recall, delayed recall, and forgetting, respectively) as one might expect, given a decrease in depression and the increased variance in memory accounted for by ECT.
Correlations between depression and memory performance were examined separately for each CR group at every time point on all memory measures. In the high reserve group, the HDRS scores were not correlated with any memory measures at baseline (r = −0.27, p = 0.17; r = −0.34, p = 0.09; r = −0.36, p = 0.06 for immediate recall, delayed recall, and forgetting, respectively), nor were HDRS scores notably correlated with any memory measures at posttest (r = −0.16, p = 0.43; r = −0.09, p = 0.67; r = −0.30, p = 0.13 for immediate recall, delayed recall, and forgetting, respectively). This was also the case for the low reserve group at posttest (r = −0.13, p = 0.56; r = 0.09, p = 0.70; r = −0.25, p = 0.26 for immediate recall, delayed recall, and forgetting, respectively). Interestingly, however, in the low CR group, baseline HDRS scores were significantly correlated with immediate recall (r = −0.52, p = 0.01) and delayed recall (r = −0.45, p < 0.05) but not with forgetting (r = 0.13, p = 0.55), suggesting that memory encoding in the low CR group may have been more negatively affected by depression severity to a greater degree.
Age
To examine the potential impact of age on memory performance, a succession of analyses were performed. As reported above, the ANOVA conducted for the entire sample (
N = 50) at baseline revealed no significant age difference between CR groups (see
Table 1). To assess whether age influenced performance on memory measures at baseline, ANCOVAs with age as a covariate were repeated for all memory measures. Results revealed the same pattern of results as originally reported. Specifically, no major group differences on immediate recall (
F = 2.99, df = 1,47,
p = 0.09), delayed recall (
F = 1.55, df = 1,47,
p = 0.22), or forgetting (
F = 0.00, df = 1,47,
p = 0.96) were found.
To assess whether age influenced performance on memory measures at posttest, ANCOVAs were repeated for all memory measures at posttest with age as a covariate (in addition to the respective baseline memory score as a covariate). Results revealed no significant differences between groups on immediate recall (F = 0.66, df = 1,46, p = 0.42), as originally found, and a major group difference in delayed recall was no longer evident (F = 3.08, df = 1,46, p = 0.09). As initially reported, a significant difference between groups on forgetting was observed (F = 6.48, df = 1,46, p = 0.01).
To further assess whether age influenced memory performance, correlations were performed for the entire sample at each time point on all memory measures. At baseline, age was not significantly correlated with any of the memory measures (r = −0.01, p = 0.95; r = −0.09, p = 0.53; r = 0.17, p = 0.23 for immediate recall, delayed recall, and forgetting, respectively). Posttest immediate recall (r = −0.30, p < 0.05) and delayed recall (r = −0.29, p < 0.05) were significantly correlated with age, but forgetting (r = 0.24, p = 0.16) was not.
Correlations between age and memory performance were also calculated separately for each CR group at each time point on all memory measures. In the high reserve group, age was not significantly correlated with any of the memory measures at baseline (r = 0.05, p = 0.79; r = −0.13, p = 0.53; r = 0.33, p = 0.91 for immediate recall, delayed recall, and forgetting, respectively) or at posttest (r = −0.19, p = 0.34; r = −0.15, p = 0.45; r = −0.05, p = 0.81 for immediate recall, delayed recall, and forgetting, respectively). Similarly, in the low reserve group, age was not significantly correlated with any of the memory measures at baseline (r = 0.02, p = 0.94; r = −0.01, p = 0.95; r = 0.09, p = 0.69 for immediate recall, delayed recall, and forgetting, respectively) or at post-test (r = −0.37, p = 0.08; r = −0.35, p = 0.10; r = 0.41, p = 0.06 for immediate recall, delayed recall, and forgetting, respectively).
Retrospective Versus Prospective Group Comparison
A portion of the subjects were drawn from the placebo condition of a study of the impact of a thyroid hormone on cognition in ECT-treated patients. A subanalysis of the placebo group and nonplacebo group (i.e., subjects not in the present study) was performed in order to ensure that a placebo effect was not a confounding factor in these data. A 2 (CR group, high versus low) × 2 (study group, placebo versus new sample) ANOVA was performed, with the forgetting score as the dependent variable. At baseline, the ANOVA revealed no significant main effect of the CR group (F = 0.04, df = 1, 46, p = 0.84) or study group (F = 0.16, df = 1, 46, p = 0.69). A significant interaction effect (F = 0.00, df = 1, 46, p = .97) was not observed. At posttest, ANCOVA (with baseline forgetting score serving as covariate) revealed a main effect for the CR group (F = 6.90, df = 1, 45, p = 0.01), but not the study group (F = 0.29, df = 1, 45, p = 0.59). A significant interaction effect was also not found (F = 0.84, df = 1, 45, p = 0.37). These data suggest that the placebo and new sample groups are similar, and that there is no artificial impact of the placebo group on the significant difference in forgetting at posttest between high and low CR groups. Furthermore, a chi-square analysis was also performed using all 50 subjects to examine the distribution of the placebo subjects within each of the cognitive reserve groups. The chi-square analysis was nonsignificant, indicating that the placebo subjects were evenly distributed between the high and low CR groups.
DISCUSSION
The results of the present study indicate that memory performance following three ECT treatments is considerably worse in patients with lower CR, as operationalized by fewer years of education and less occupational attainment. Data presented in this study support the CR theory, which posits that individuals with greater CR have a higher threshold for potential neurocognitive symptoms after CNS assaults, and that individuals with lower CR have a lower threshold and are, consequently, more vulnerable to dysfunction. The current findings are consistent with results from related studies of patients with Alzheimer's disease, Parkinson's disease, schizophrenia, and HIV that reveal significant differences in the neuropsychological performance of individuals with high versus low cognitive reserve. The present study extends CR theory to electroconvulsive therapy, an area in which CR had not previously been examined. The results of this study also provide evidence that cognitive reserve accounts for some of the individual differences in the cognitive side effects of ECT.
Whether individuals with greater education merely exhibit superior performance on standardized neuropsychological tests is an important issue in CR studies that consider factors involving educational attainment. The results of the present study argue against differential memory performance that is solely due to educational status. This is exemplified in the lack of significant difference in immediate recall, delayed recall, and the percentage of information forgotten between CR groups at baseline, along with the lack of significant difference in immediate recall and the presence of a significant difference in the percentage of information forgotten after three ECT treatments.
Future research should aim to examine possible shortcomings of the present investigation. The current findings do not provide evidence of the additive effect of educational and occupational attainment. Rather, it was found that education and occupational attainment were highly correlated with each other, and thus did not result in independent contributions to the presentation of memory dysfunction following ECT. Consideration of alternative occupational measures (i.e., measures which classify according to skills and repertoires rather than social factors inherent to particular employment positions) may prove useful in delineating the unique contributions of occupational status to CR. In addition, the findings of the current study were based on a patient sample consisting of individuals with a variety of clinical features, psychiatric histories, and medical histories. In particular, the patient sample included individuals who may have been taking an array of medicines (including psychotropics) that may have impacted memory performance. Thus, results may have been confounded. Because pharmacologic agents may affect performance on memory tests, this study should be replicated on a sample of patients with similar drug regimens or in patients who have undergone an adequate washout period prior to ECT. Future studies may also examine potential interaction among CR, psychiatric diagnosis, and/or comorbid conditions on memory functioning after ECT, given outcomes suggesting that diagnosis (i.e., psychosis) may influence response to ECT
29 and comorbid medical conditions (i.e., heart disease) may lower CR.
9The results of this preliminary study, if replicated, may have important applications and implications. Findings consistently reveal that ECT negatively effects memory performance in some patients. If the results of this study are replicated, and CR is found to be a true cofactor influencing memory performance after ECT, direct impact on clinical decision making with ECT treatment procedures could potentially result. For example, if low CR truly does serve as a vulnerability factor for memory impairment after ECT, individuals with low cognitive reserve may be treated under conditions that have been shown to reduce the impact of ECT on memory, such as unilateral ECT or twice weekly versus thrice weekly schedules. Data from this study may have important implications for CR theory; these data elucidate potential factors that contribute to CR, and they suggest that CR influences neuropsychological performance in numerous conditions or after specific treatments.