I t is not uncommon for depressed patients to complain of problems concentrating or remembering. Their complaints, however, do not always correlate with the results of objective tests; in other words, they feel that they do worse than the results warrant. On the other hand, patients with mood disorders in general and depression in particular are known to have actual impairments that can be measured with neuropsychological tests in various cognitive domains. The more severe their condition, the more apt they are to be cognitively impaired.
1 Depressed individuals may have severe, global cognitive defects or focal, discrete cognitive deficits, or they may be cognitively intact. Their cognitive status is dependent on age, depression severity, premorbid cognitive state, or whether they have a comorbid condition, such as stroke or early dementia. However, even mildly depressed patients without complicating factors are more impaired, as a group, than normals.
2 As a rule, patients with bipolar disorder or psychotic depression are more impaired than patients with nonpsychotic unipolar depression.
3,
4Investigators have established that cognitive impairment is a concomitant of affective illness, and deficits have been elicited in every cognitive domain. The focus of recent research has been to discern a pattern of specific cognitive functions that might be selectively impaired in depressed patients. If this is found to be true, it might have a bearing on issues related to diagnosis and treatment.
Specific neurocognitive deficits have been demonstrated in tests of sustained and/or selective attention. Attentional problems have been demonstrated in mixed groups of depressed patients, including young patients who are drug-free.
5,
6 Impairments in working memory, a cognitive function that requires effortful attention, also occur in patients with depression.
7,
8 The attentional deficits of depressed patients are more likely to be evident in effortful tasks.
9Studies of attentional impairment in depressed patients highlight the fragility of their subjective responses and the interaction between cognition and emotional response. Depressed patients tend to overreact to the mistakes they make. In one study, depressed men made more errors on a sustained attention task than nondepressed men, but they reported much higher incidences of cognitive failures on a standardized questionnaire. It was concluded that depressed patients responded “catastrophically” to errors. Making mistakes, even on a simple task of sustained attention, seemed to heighten their subjective sense of failure.
1Another specific area of neurocognitive impairment in depressed patients is in tests of memory.
10,
11 Depressed patients are aware of memory impairment in their day-to-day lives.
12 Studies have suggested that memory systems reliant on medial temporal lobe structures are impaired in patients with depression. The relationship between depression and some specific component of the memory system, however, is ambiguous. To date, studies have demonstrated problems with encoding as well as retrieval, recall as well as recognition.
13,
14 Depressed patients have particular difficulties with memory tasks requiring sustained effort, such as list learning and free recall, which are qualitatively different from tasks carried out automatically (e.g., memory for spatial events).
15The memory deficits of depressed patients seem to be independent of the patients’ current mood state, but they are related to the past course of the patients’ illness; for example, the number of prior depressive episodes. Thus, memory impairment is at least to a degree trait-related, in contrast to attentional dysfunction, which appears to be state-dependent.
12Psychomotor retardation is not necessarily pathognomonic of depression. However, it is one of the most dramatic symptoms of major depression and one that should be demonstrable on neurocognitive tests. In fact, psychomotor slowing can be demonstrated in depressed patients in numerous ways, including reaction time measures, information processing speed, writing and drawing tasks, and other kinesthetic measures.
16 –
21 Younger depressives are less likely to evidence psychomotor slowing than older patients.
6Language functions tend to be preserved in various forms of depression, although impairments in fluency have been noted.
5,
22 Fossati et al.
23 found verbal fluency impairments in patients with depression to be associated with reduced ability to shift mental set on card sorting tests, suggesting that language deficits were not primary but reflective of general executive problems in depression.
Performance on measures of executive control functions tend to be impaired in depressed patients, although not to the degree they are compromised in schizophrenics.
4,
6,
27 Nevertheless, investigators have proposed that even if the impairment in brain function is global and diffuse, there is “particular involvement of the frontal lobes in nonpsychotic unipolar major depressive disorder.”
5 Moreover, executive dysfunction can be demonstrated in young as well as old depressed patients.
28Unipolar depressed patients exhibit executive deficits in tests of inhibition, problem-solving and planning. Cognitive inhibition deficits in depressed patients can lead to inefficient allocation of cognitive resources. They can cause the depressed patient to process information that is either irrelevant or counterproductive and thus reduce his or her capacity to deal effectively with depressive thinking and mood control.
29,
30Several studies have found evidence of problem solving impairments in depressed patients. In card sorting tasks, depressed subjects have difficulty with hypothesis testing and cognitive flexibility. This state of cognitive rigidity can prevent patients from coping with life events, thus perpetuating depressed mood by prolonging stress exposure. Planning tasks, such as the Tower of London Test, also demonstrate that depressed patients fail to use negative feedback as a motivational boost to improve their performance.
29In addition, executive functioning deficits may predict a poorer outcome in depression. Thus initiation and perseveration scores—measures of cognitive flexibility—are associated with relapse and recurrence of depression and residual depressive symptoms.
29Brain imaging studies show that reduced blood flow, particularly in medial prefrontal cortex and dorsal anterior cingulate cortex, subserves executive impairments in depression. Neuroimaging studies also underscore the importance of mood-cognitive interactions in depression. A recent working model of depression
31 implicates failure of the coordinated interactions of distributed cortical-limbic pathways in the pathology of depression. According to this model, neocortical (prefrontal and parietal regions) and superior limbic elements (dorsal anterior cingulate) are postulated to mediate impaired attention and executive function, whereas ventral limbic regions (ventral anterior cingulate, subcortical structures) are postulated to mediate circadian and vegetative aspects of depression.
32Not everyone agrees, however, that executive dysfunction is central to neurocognition in depression. In 2003, Porter et al.
6 indicated that confounding factors, such as the effects of psychotropic medication, had rarely been controlled for in studies of neurocognition in depression. Porter et al. studied 44 medication-free major depressive disorder patients for at least 6 weeks. The patients were impaired significantly in a range of cognitive domains, including attention and executive function and visuospatial learning and memory, compared with healthy subjects. Motor and psychomotor functions were intact. The study found severity of depression to be correlated with learning and memory performance but not with executive function.
6HYPOTHESES OF NEUROCOGNITIVE IMPAIRMENT IN DEPRESSION
As research has broadened in recent years and more data have accrued, including data from neuroimaging technology, investigators have aimed to ascribe a pattern to the neurocognitive deficits that occur in depression.
24 There are at least three theories that ascribe a specific pattern to the neuropsychology of depression. One such theory is the effort hypothesis, which states that performance on effortful tasks is disproportionately impaired in depressives compared with the performance on automatic tasks. Above, we have alluded to several instances where effortful tests of attention and memory were more likely to reveal impairments in depressed patients. The second, the cognitive speed hypothesis, states that depression is characterized by cognitive slowness and that slowing may be at the root of other cognitive impairments. Research indicates that cognitive functioning in depression is characterized by a reduced speed of information processing. Researchers who favor the cognitive speed hypothesis tend to dismiss the effort hypothesis, although the two are by no means mutually exclusive.
26 The third hypothesis, also alluded to previously, is that impairment in executive control functions is central to the neurocognition in depressed patients. Because at least some degree of neuropsychological impairment is a trait marker for depression, “localizing” the deficits of depressed patients to one particular functional system would be a signal advance. Even though depressed patients have difficulty with effortful tasks and impairments in cognitive speed and executive function are reliably demonstrated, universal acceptance has not been given to the cognitive speed hypothesis or the executive function hypothesis. In contrast to theories of specific impairment is what could be referred to as the global impairment hypothesis: that depressed patients suffer from diffuse cognitive impairments—that their test performance is heterogeneous and that group analysis does not reveal any coherent pattern of dysfunction.
25 Ravnkilde et al.
25 averred that “the large range of existing neuropsychological, neuropsychiatric, and, more recently, neuroimaging investigations have not yet given a consistent picture of the psychological… disturbances involved in depression.” Their research indicated that 1) depressed patients suffer from widespread cognitive impairments, 2) test performance was heterogeneous, and 3) group analysis did not allow any hypothesis on a possible pattern to the dysfunctions. The Danish Positron Emission Tomography/Depression Project attempted to clarify the relationship between cognitive functions and regional cerebral blood flow (rCBF) in a large group of depressed patients compared with healthy subjects. A set of principal components was extracted from scores of a battery of neuropsychological tests of 40 patients suffering from major depression and 49 healthy subjects. The components were correlated by multiple linear regression analyses to selected regions of interest in the brain obtained from positron emission tomography images. In contrast to findings in the healthy comparison subjects, cognitive functions in the depressed patients correlated significantly with rCBF in specified regions of interest in only a few instances. The authors concluded that disturbed cognitive functions in depression do not relate to specific areas of the brain in the same way as normal cognitive functioning, suggesting that the abnormalities of brain function in major depression may be qualitative rather than quantitative in nature. One of the only studies that addressed the “ecological validity” of neuropsychological testing in depressed patients was reported by McCall and Dunn.
33 They discovered that patients’ problems in instrumental activities of daily living were most closely associated with deficits in global cognition. The cognitive impairments of depression can be improved by effective antidepressant therapy, even in elderly patients.
34 However, there is little evidence to show that they actually normalize.
35 Residual deficits may persist, especially in older patients and in patients with unipolar and bipolar depression, dysthymia, and schizoaffective disorders.
36 –
38 In cases of late-onset major depressive disorder, resistance to treatment is associated with impaired executive function, which may involve subtle cerebrovascular pathology.
39Pertinent literature is compromised by studies of relatively small samples of heterogeneous patients. In many studies, the effects of psychotropic medications are not controlled; in other studies, patients’ clinical state is not controlled. Further, investigators use different tests that render comparisons across studies extremely difficult, or they administer limited test batteries that address performance in only one or two cognitive domains. Nevertheless, the literature is clear in showing that patients with depression are, as a group, subject to neuropsychological deficits in attention, memory, psychomotor speed, processing speed, and executive function. Their deficits are less severe than those of patients with psychotic depression or bipolar depression but similar in kind. Their deficits improve, at least to a degree, with effective treatment but never seem to normalize. Neurocognitive impairment is a trait marker for depression. Whether the cognitive impairments that characterized depressed patients are specific or general is not a trivial question. It is possible that appreciating the true nature of neurocognition in depression would have an impact on diagnosis, or subtyping, or even treatment, especially cognitive-based therapies. To address this question from a clinical perspective, we administered a computerized neurocognitive testing battery that addressed a range of cognitive domains to three groups of subjects: depressed patients who were not yet on medication, an equal number of depressed patients who had responded favorably to medication treatment, and matched healthy subjects.
METHODS AND MATERIALS
This was a retrospective cross-sectional study of neurocognitive performance in patients with depression and healthy subjects.
Subjects
The subjects of this investigation were unipolar, nonpsychotic patients with major depressive disorder. They were all outpatients at the North Carolina Neuropsychiatry Clinics in Chapel Hill and Charlotte, private clinics specializing in neuropsychiatric evaluation and medication treatment. Every new patient at the Neuropsychiatry Clinics is administered a computerized neurocognitive test battery. Once patients achieve a satisfactory clinical response to treatment and medications are stable for at least 4 weeks, they are tested again. None of the patients whose data we studied were involved in clinical trials. Patients gave written informed consent to allow their de-identified data to be used for purposes of research and evaluation. One group was comprised of patients with major depression who were tested prior to initiating treatment. Patients were on no psychotropic drugs (major depressive disorder, N=38). The other patient group was comprised of major depressive disorder patients who had been successfully treated and were currently on antidepressant monotherapy for at least 4 weeks, with no other psychotropic medications (major depressive disorder-Rx, N=31). No comorbid diagnoses were permitted. Patients’ psychiatric diagnoses were conferred by a senior psychiatrist, using DSM-IV-TR criteria. The diagnoses were confirmed by a second psychiatrist. All patients completed the Central Nervous System (CNS) Vital Signs computerized screening battery (major depressive disorder patients, as part of their initial evaluation at the clinic, and major depressive disorder-Rx patients, after they had achieved a therapeutic response and been on a stable medication dose for at least 4 weeks). The 38 major depressive disorder patients had a mean score on the Beck Depression Inventory of 16.86 and a mean Hamilton score of 15. The 31 major depressive disorder-Rx patients had a mean score on the Beck Depression Inventory of 1.5 and a mean Hamilton score of 6. They were on the following medications and no other drugs: citalopram, 1; fluoxetine, 3; escitalopram, 8; paroxetine, 3; mirtazepine, 1; trazodone, 1; venlafaxine, 5; bupropion, 6; sertraline 3. Healthy comparison subjects were generated from the CNS Vital Signs database. They were drawn randomly from a database of more than 500 healthy people. (“Normals” were individuals who were in good health, medication-free, and free of any present or past neurological, medical or psychiatric disorder.) Sixty-nine normals were selected matched to the patient groups by age and race and gender (NML, N=69).
Cognitive Evaluation
Patients’ neurocognitive performance was measured on a computerized battery of tests, CNS Vital Signs. CNS Vital Signs is a PC-based neurocognitive screening battery, comprised of seven familiar neuropsychological tests: verbal and visual memory (verbal memory, visual memory);
49,
50 finger tapping test;
51 symbol-digit coding;
52 the Stroop test;
53 the shifting attention test;
54 and the continuous performance test.
55 The test battery is self-administered in the clinic on an ordinary PC and takes approximately 30 minutes to complete. The tests in the vital signs battery are highly reliable (test-retest, r = 0.65–0.88) (Gualtieri, Johnson & Benedict, 2004). Normative data from > 500 healthy subjects, age 10–89, indicate typical performance differences by age and gender (Gualtieri, Johnson & Benedict, 2004b). Concurrent validity was established in studies comparing the vital signs battery to conventional neuropsychological tests.
54 The tests in CNS Vital Signs are reported as raw test scores from the individual tests (15 primary variables, e.g., correct responses, errors, and reaction time). The seven tests in turn generate six domain scores, empirically derived by factor analysis. These are: memory (derived from verbal memory and visual memory); psychomotor speed (from finger tapping test and symbol-digit coding); reaction time (Stroop test); cognitive flexibility (Stroop test and shifting attention test); complex attention (Stroop test, shifting attention test, continuous performance test); and vigilance (continuous performance test). (Cognitive flexibility is an executive control function.) Domain scores are reported as standard scores (
z scores standardized to a mean of 100 and a standard deviation of 15). The average of the z scores for five of the domains generates a summary score, which is reported as a standard score (NeuroCognition Index [NCI]). (This is similar to an IQ score on the Wechsler Adult Intelligence Scale or the Stanford-Binet that is generated by averaging the z scores of the various subtests.)
Procedure
The CNS Vital Signs database contains records from more than 2000 patients with neurological and/or psychiatric disorders. The database contains data from all the patients who visited the clinic within a 14-month period (July 2003 through August 2004). The database was scanned for patients whose primary diagnosis was major depression and whose age was 18–65 years. Two hundred thirty-seven (237) patients were thus identified. Patients were deleted if they had comorbid neurological or medical conditions, cognitive disorders (e.g., dementia, brain injury, learning disabilities) or significant psychiatric disorders (e.g., attention deficit disorders, personality disorders, schizophrenia, obsessive-compulsive disorder). The data pool was thus reduced to 183. From this pool, two groups were extracted: 1) major depressive disorder patients on no medication, with scores on the Beck Depression Inventory >14 and/or on the Hamilton Depression Rating Scale >14; and 2) major depressive disorder patients who were on only one medication (one of the modern antidepressants) and who had been on a stable dose of medication for >4 weeks, and whose Beck and/or Ham-D scores were <10. Once patients were selected who met inclusion and exclusion criteria, the CNS Vital Signs database computer extracted healthy subjects randomly but matched for age, race, and gender.
Analysis
CNS Vital Signs generates 15 primary scores, six domain scores, and one summary score. Group differences were assayed by multivariate analysis and by rank-order analysis. Post hoc tests included the Bonferroni correction and pairwise t tests.
RESULTS
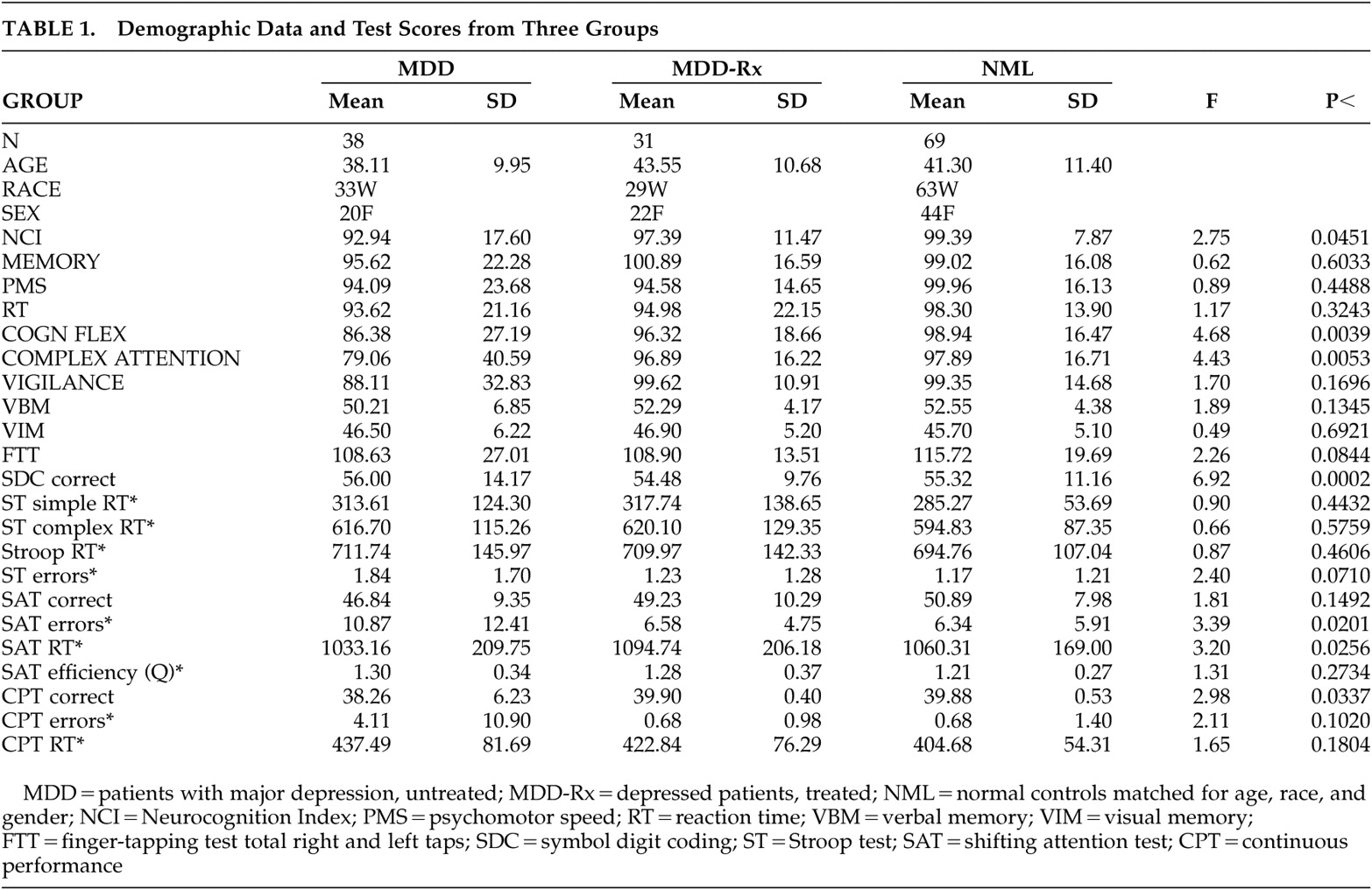
Clinical and neurocognitive data from the three groups are presented in
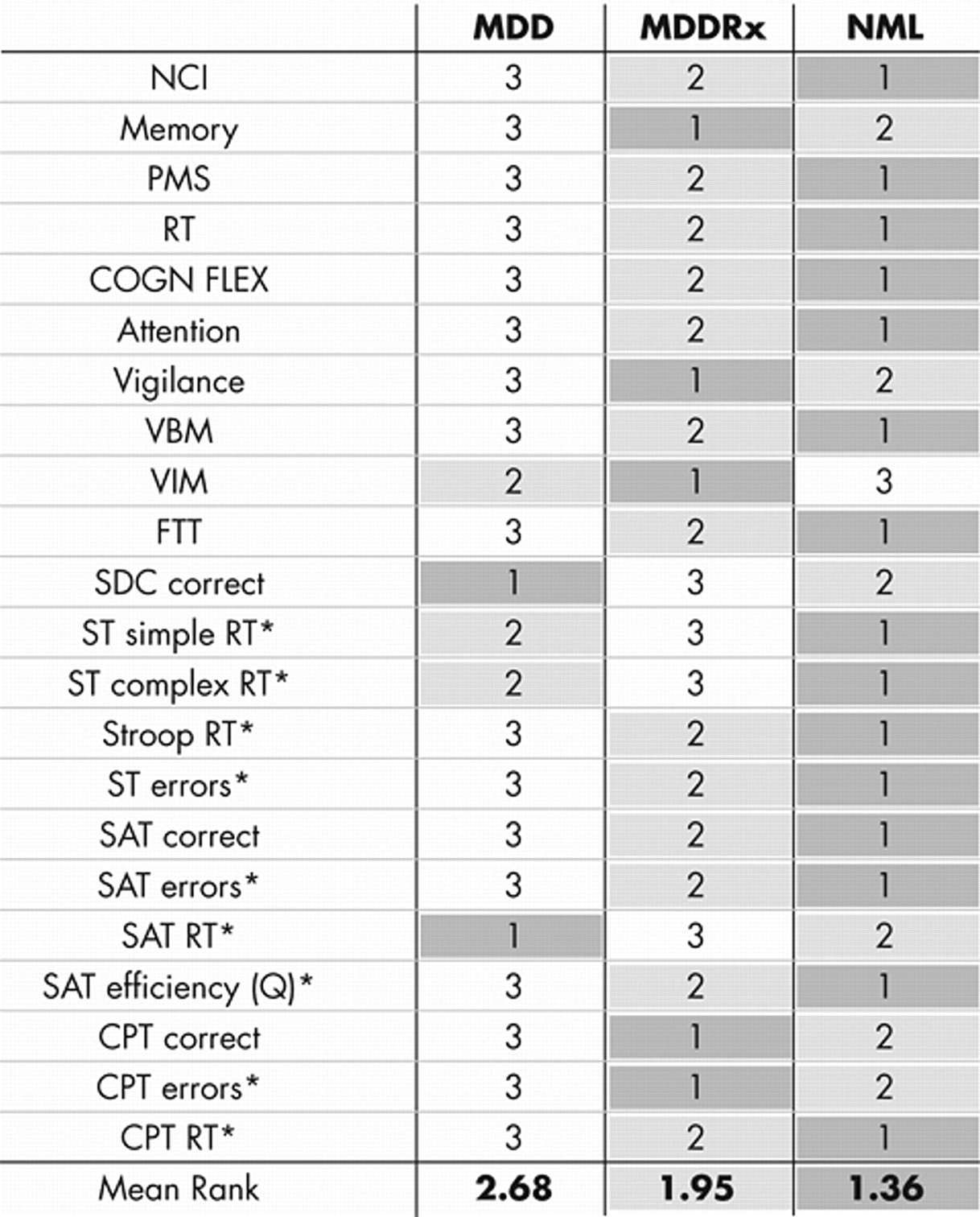
Table 1 . Multivariate analysis with age as a covariate indicated significant group differences for the Neurocognition Index and for the domain scores of cognitive flexibility and complex attention. Post hoc analysis (pairwise t tests) indicated significant differences between the major depressive disorder group and normals on the Stroop test (errors, t 2.13, p=0.04); the shifting attention test (correct, t 2.36, p=0.02; errors, t 2.12, p=0.04); and the continuous performance test (reaction time t 2.22, p=0.03). These differences were found in the domains of cognitive flexibility (t 2.60, p=0.01), complex attention (t 2.73, p=0.01), and vigilance (t 2.00, p=0.05) as well as in the Neurocognition Index (t 2.09, p=0.04). The major depressive disorder group differed from the major depressive disorder-Rx group in the domains of complex attention (t 2.48, p=0.02) and vigilance (t 2.03, p=0.05). There were no significant pairwise differences between the major depressive disorder-Rx group and healthy subjects. Significant differences in test scores were mainly between untreated depressives and the other two groups. However, rank order analysis indicates a somewhat different picture (
Figure 1 ). Rank ordering indicates that normals scored higher than treated depressed patients in the Neurocognition Index summary score in four of six domains and in 10 of the 15 primary scores. This difference was highly significant (Kendall’s W 0.44, Chi square 19.2, p<0.0001). If anything, this ordering understates the superiority of the healthy group. For example, on the shifting attention test, untreated major depressive disorder patients had the fastest reaction times. However, they also made the most errors and had the worst efficiency score. (Efficiency, or Q, is a speed-accuracy trade-off statistic
44 derived by dividing reaction time by percent correct.) In a speed-accuracy trade-off test, a fast reaction time is a good sign only if it is accompanied by a high rate of correct responses, a low rate of errors, and a low efficiency score (Q). For most variables, healthy subjects perform best, followed by major depressive disorder patients on antidepressants, and drug-free major depressive disorder patients perform worst. This pattern is illustrated in
Figure 1, where data are presented for the Neurocognition Index.
DISCUSSION
Our findings are consistent with the literature—that patients with depression are subject to multiple neuropsychological deficits. Patients whose depression is successfully treated with modern antidepressants are better cognitively than untreated patients, but they do not perform better than healthy comparison subjects. In our study, group differences were evident in measures of cognitive flexibility, complex attention, processing, and vigilance. It may be true, therefore, that the neurocognitive deficits of depressed patients are general in nature. However, our data also indicate that deficits in certain domains may be more important than others. In a more molecular analysis, pairwise analysis indicates differences between untreated major depressive disorder patients and healthy subjects in measures of cognitive flexibility (Stroop test errors and shifting attention test errors), processing speed (symbol-digit coding) and vigilance attention (continuous performance test correct responses). Treated depressed patients performed better than untreated patients in measures of cognitive flexibility and complex attention. It would appear, then, that these two measures of executive ability are central to the neurocognition of depression and that deficits in these areas are responsive, at least to a degree, to successful treatment.
The results of this investigation touch upon the several hypotheses of neurocognition in depression, which we discussed. We are clearly supportive of the executive function hypothesis. Patients’ performance in the shifting attention test, the Stroop test, and the domains of cognitive flexibility and complex attention reflects the importance of executive function deficits in depression. These results are also supportive of the effort hypothesis. Coding, the shifting attention, and continuous performance tests are the most effortful tests in the CNS Vital Signs battery. The tests of verbal and visual memory, which did not register at a significant level in any of the comparisons, are simple recognition tests and the least effortful tests on the battery. The cognitive speed hypothesis predicts that measures of processing speed, such as reaction time measures and symbol-digit coding, should be relatively more impaired in depressed patients. In the CNS Vital Signs battery, there are four reaction time measures. The coding test (symbol-digit coding) is another way to measure cognitive processing speed. Significant differences were apparent only in the coding test. Processing speed deficits may be central to the neurocognition of depression, but they are only manifest in complex and effortful tests, such as coding. It does appear, at least superficially, that depressed patients, untreated, have global cognitive impairments and that treated patients tend to perform better globally. This is manifest in the rank-order analysis and also by the NCI, a measure of general cognitive ability (
Figure 1 ). However, closer examination of the data suggests that there is specificity to the neurocognition of depression. Executive ability, processing speed, and effortful attention appear to be the most important elements in the neurocognition of depression. A naturalistic, cross-sectional study of a comparatively young patient group may not be the optimal environment for contending with all the implications of what is clearly a complex subject. In light of the variance in test scores, and the relatively small absolute differences, larger prospective studies will be necessary to generate unambiguous results. The severity of patients’ depression and the degree to which they have responded to treatment might have been calibrated with more precision than the authors have done. In addition, a comparison group treated with the entire gamut of “modern antidepressants” (i.e., not tricyclics or monoamine oxidase inhibitors) is actually not equal to the importance of the questions posed in this study. It is not unlikely, for example, that different antidepressants have different neurocognitive profiles.
45 While our findings are certainly suggestive, they are not as definitive as those of a larger prospective study might be. The use of a computerized battery of tests has both advantages and disadvantages. The performance of an unsupervised subject sitting in front of a console may not always represent an optimal testing environment. In a study of newly admitted psychiatric inpatients, Weber et al.
46 reported that patients’ negative attitude toward computers was associated with nervousness during testing and with poor results in certain tasks. This was especially true of depressed patients. The performance deficits, however, were only manifest in computerized tests of attention. On the other hand, Gur et al. reported that schizophrenic patients performed equally well (or poorly) on traditional neuropsychological batteries and computerized tests and that “the patients tolerated the computerized scan well. In contrast to the traditional battery, which taxes patients’ endurance, patients seemed to appreciate the brevity of the computerized scan. They did not have difficulties operating the computer and informally they appeared more relaxed being tested by a computer rather than a person.”
47 Indeed, computerized testing has clear advantages, compared to traditional paper-and-pencil testing. These include better standardization in administration and scoring, the ability to generate numerous alternative forms suitable for repeated testing, precise stimulus control, the ability to track various components of subjects’ responses, increased cost efficiency in testing, and the ability to develop large and accurate databases.
48 If it is true that treated depressives are functioning, cognitively 3% below healthy people and untreated depressives are functioning with a 7% decrement, then cognitive evaluation should probably be part of routine patient evaluation. The precise nature of patients’ cognitive deficits and the impact they have on patients’ day-to-day lives should be a focus of ongoing treatment. The wide availability of the new computerized test batteries, inexpensive and easy to use, makes this a feasible option for physicians in clinical practice.
Acknowledgments
Drs. Gualtieri and Johnson are two developers of the CNS Vital Signs screening battery.
Dr Gualtieri has conducted clinical trials on behalf of Astra-Zeneca, Bristol-Myers Squibb, Cephalon, Eli Lilly, Glaxo-Smith-Kline, Medeva, Organon, Shire, Wyeth-Ayerst, and UCB and has been a speaker and/or consultant to Eli Lilly, GSK, Pfizer, Shire and Wyeth.
Research for this study was supported by North Carolina Neuropsychiatry, PA, in Chapel Hill and Charlotte. No external support was sought or received.