A growing body of research has begun to assess the effectiveness of various outreach, housing, and treatment approaches in meeting the complex needs of persons with mental illness who are homeless or residentially unstable. However, there have been very few randomized trials of carefully documented models intended to reduce the incidence of homelessness among persons with severe mental illness. The period after hospital discharge is one in which persons with severe mental illness are at high risk of either first-episode or recurrent homelessness (
1,
2). This is also a high-risk period for other adverse outcomes, including suicide (
3–
5), psychiatric rehospitalization (
6,
7), and violence against others (
8). Reasons for this may include the impact of enduring psychiatric symptoms that preceded the inpatient episode plus difficulties in establishing effective connections to sources of treatment, housing, and support in the community. Furthermore, like many transitional periods, the time after institutional treatment is commonly one of significant personal disequilibrium.
Critical time intervention (CTI) aims to prevent recurrent homelessness and other adverse outcomes after discharge in two ways: by strengthening the individual's long-term ties to services, family, and friends and by providing emotional and practical support during this critical transition period. An important aspect of CTI is that postdischarge services are delivered by a worker who has established a relationship with the client before discharge. CTI shares with long-term assertive community treatment models a focus on promoting development of independent living skills and building effective support networks in the community (
9). The emphasis, however, is on maintaining continuity of care during the critical period of transition while primary responsibility gradually passes to existing community supports that will remain in place after the intervention ends. Such an approach, we believe, increases the likelihood that the impact of a time-limited intervention will persist beyond its actual endpoint, which is the primary goal of CTI.
Previous studies provide evidence of CTI's effectiveness in producing an enduring positive effect on housing outcomes among homeless adults with severe mental illness. The first was a randomized trial among 96 homeless men with severe mental illness who were placed into housing from a large shelter in New York City (
10). In that study, a nine-month CTI produced a significant reduction in postdischarge homelessness, which, crucially, remained evident up to the end of an 18-month follow-up period. Subsequently, a six-month version of CTI was tested at eight U.S. Department of Veterans Affairs medical centers (
11). A quasi-experimental study compared the outcomes of two cohorts of homeless persons with severe mental illness after discharge from inpatient psychiatric treatment. One cohort (N=278) received standard case management, and the other (N=206) received CTI. Controlling for baseline differences, the investigators found that the CTI cohort had significantly more days housed than did the comparison cohort over the one-year follow-up period and that this effect also persisted after the intervention ended (
11).
In this article, we report the results of a single-blind randomized trial that tested whether nine months of CTI would produce an enduring effect in preventing homelessness among formerly homeless men and women with severe mental illness after discharge from inpatient psychiatric treatment. The trial was approved by the discharging hospital's institutional review board (IRB) under a multisite collaborative agreement overseen by the New York State Office of Mental Health.
Methods
Our original design called for participants to be recruited during their inpatient stay at a state-operated psychiatric hospital located in the New York City metropolitan area. However, before recruitment began, policy changes in the mental health system led most patients with housing difficulties to be discharged to transitional residences located on the grounds of that hospital and a second nearby hospital. We therefore altered our design to recruit participants at these two residences rather than from the inpatient wards. Persons were considered eligible if they met the following criteria: currently living in one of the two designated transitional residences after hospitalization during the four-year recruitment period (2002–2006) and discharged from the residence before the end of this period, had a lifetime DSM-IV diagnosis of a psychotic disorder (codes 295.xx, 296.xx, and 298.9), homeless at the index hospitalization or had had an episode of homelessness within 18 months before this admission, and spent their first night after leaving the transitional residence in New York City in a place other than a jail or a hospital (so that all eligible participants were at equal risk of homelessness during the observation period and those assigned to the CTI condition would be accessible to the CTI worker).
We excluded those who were unable to provide informed consent for the screening interview or who did not speak sufficient English to participate. We also excluded those who did not stay more than three weeknights in the transitional residence or whose employment schedule made them unavailable to project staff during regular work hours. [A figure summarizing screening, accrual, and retention of the sample is available as an online supplement to this article at
ps.psychiatryonline.org.]
Research staff approached individuals identified by clinical staff as having a plan for discharge to New York City. After obtaining written consent for the screening interview, research staff determined whether individuals had been homeless (defined as staying overnight in a shelter, on the streets, in a park, on a subway train, or in any other public space) during the 18 months before hospitalization. Those who met this criterion were then provided with the study description, and their written informed consent for participation in the trial was obtained. Eligible participants completed a baseline interview, including the Structured Clinical Interview for DSM-IV (
12); this was used to verify that the participants met our diagnostic eligibility criterion. Those not meeting this criterion were excluded at this point.
Randomization
Participants were randomly assigned independently by gender and by diagnosis of lifetime substance use disorder. To reduce variation on key factors, we randomly assigned individuals in these four strata in permuted blocks of randomly varying size. The names of eligible participants and their respective randomization stratum were given to an administrator who did not need to be blind to treatment status. Working from a list of identification numbers with associated random treatment condition assignments produced by our statistician, the administrator assigned each participant the next available identification number within the designated stratum. For participants assigned to the CTI condition, the administrator then notified the CTI clinical supervisor, who added the participant to the CTI caseload. Thirty-two randomly assigned participants were subsequently dropped from the study because they were never discharged from the transitional residence during the recruitment period or because their first postdischarge night was spent either outside of New York City, in jail, or in a hospital. This procedure was approved a priori by the study's biostatistician.
Assessments
The Personal History Form, used extensively in our earlier research with this population, was used at baseline to identify demographic characteristics and collect personal history, including prior use of treatment services, residential history, and previous homeless episodes (
10). After discharge from the transitional residence, participants were interviewed every six weeks for 18 months in order to document where they had spent each night during the respective follow-up period. These assessments were carried out by trained interviewers blind to group assignments. In cases in which a participant had missed an interview, the interviewer documented where the participant had spent each night since the last completed assessment. We chose to collect data at six-week intervals for two reasons. First, we sought to minimize reporting inaccuracies on the part of study participants with respect to their housing experience. Furthermore, our previous experience with this population suggests that more frequent contact between research staff and participants reduces the likelihood that participants will be lost to follow-up. In some instances when participants could not be directly interviewed, we gathered residential data from a family member, caseworker, or another of the participant's close associates whom we had been granted permission to contact. We have reported previously on a test-retest study demonstrating that homelessness could be assessed with high reliability (
κ=.93) using this approach (
10). Participants received $20 for each of the baseline, nine-, and 18-month interviews and $10 for each six-week interview they completed.
Interventions
While living in the transitional residence, all participants received basic discharge planning services and access to psychiatric treatment. After discharge, participants in both conditions received a range of “usual” community-based services, depending on the individual's needs, preferences, and living situation. These services usually included various types of case management and clinical treatment. Twelve (8%) participants were assigned to mandatory outpatient treatment, assertive community treatment, or both programs.
In addition to these services, participants assigned to the experimental condition received nine months of CTI after discharge from the transitional residence. Those assigned to the control condition received usual services only. Postdischarge housing arrangements were typically coordinated by discharge planning staff located at the transitional residence. These arrangements ranged from community residences and other structured programs to supported apartments and independent housing, either alone or with family members. Neither CTI workers nor research staff members were involved in determining the initial housing arrangement for individuals in either condition. Some individuals left the transitional residence “against medical advice” and returned to shelters or the streets but were nonetheless retained in the study.
CTI is described in detail in our previous publications (
13,
14). In brief, it is a nine-month case management intervention delivered in three phases, each of which lasts approximately three months (see
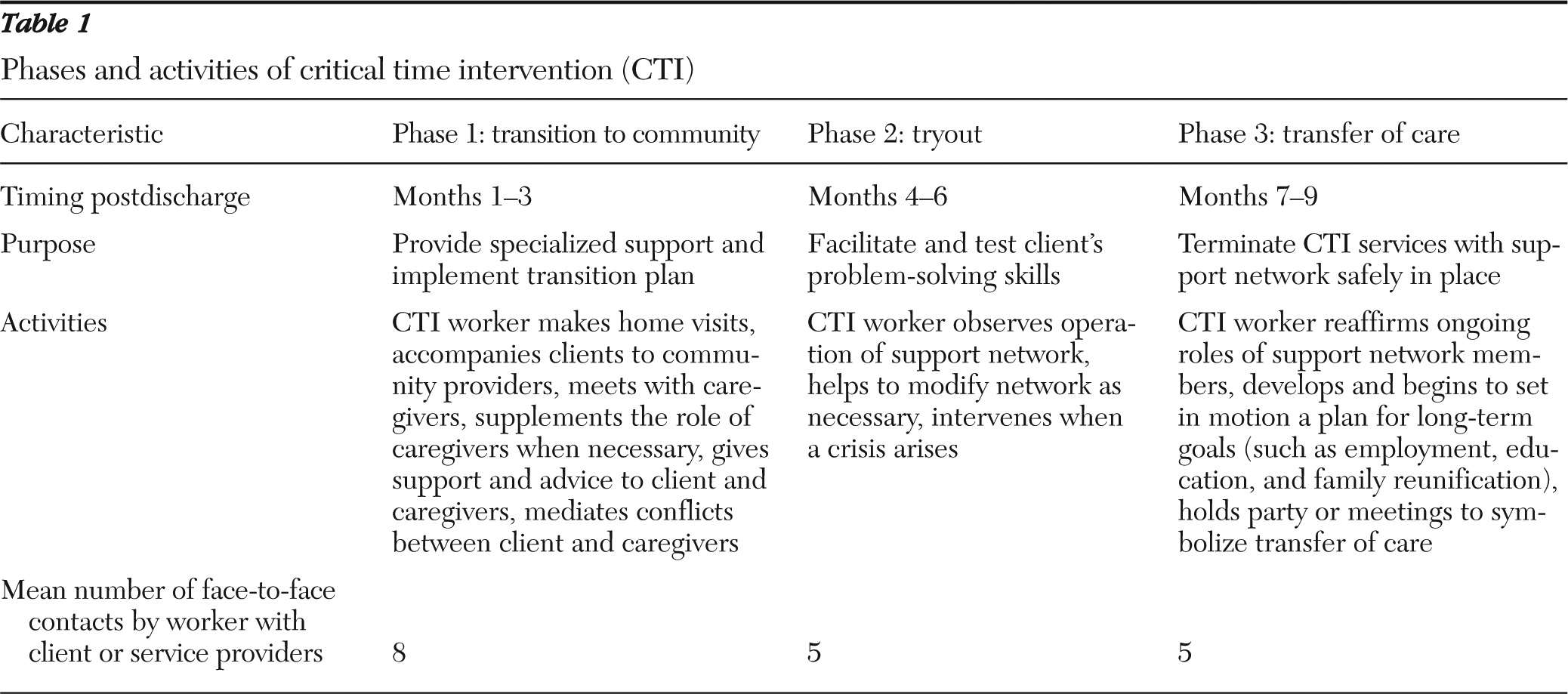
Table 1). Phase 1—transition to the community—focuses on providing intensive support and assessing the resources that exist for the transition from inpatient care to community providers. Ideally, the CTI worker will have already begun to engage the client in a working relationship before he or she moves into the community. This is important because the worker will build on this relationship to effectively support the client after discharge from the institution. The CTI worker generally makes detailed arrangements in only the handful of areas seen as most critical for community survival of that individual. Phase 2—tryout—is devoted to testing and adjusting the systems of support that were developed during phase 1. By now, community providers will have assumed primary responsibility for delivering support and services, and the CTI worker can focus on assessing the degree to which this support system is functioning as planned. In this phase the worker will intervene only when modification in the system is needed or when a crisis occurs. Phase 3—transfer of care—focuses on completing the transfer of responsibility to community resources that will provide long-term support. One way in which CTI differs from services typically available during transitional periods is that the transfer of care is not abrupt; instead, it is a process and represents the culmination of work occurring over the full nine months.
CTI was delivered by three workers trained by several of the model developers. Two were bachelor's-level employees of the New York State Office of Mental Health reassigned to this project from their regular duties. The third worker, who also performed some supervisory activities, was a more experienced worker who had delivered CTI in an earlier trial. Weekly supervision was carried out by clinically trained staff experienced in the model.
Study attrition and treatment receipt
Of the 150 participants, 77 (51%) were assigned to the experimental condition (CTI) and 73 (49%) were assigned to the control condition (usual care). Fifty-eight participants (75%) assigned to the experimental condition completed the 18-month follow-up period, and 59 participants (81%) assigned to the control condition completed the full follow-up period. [A flowchart is available as an online supplement at
ps.psychiatryonline.org.] Complete follow-up data were obtained for significantly more men than women (N=91, 85% of men; N=25, 58% of women;
χ2=12.7, df=1, p=.001). Participants with a substance dependence diagnosis were also more likely to have completed the follow-up (N=73, 91% of those with substance dependence; N=43, 61% of those without substance dependence;
χ2=18.9, df=1, p<.001). There were no other group differences in loss to follow-up that were related to baseline characteristics, including prior homelessness.
Some participants assigned to the experimental condition did not receive all components of the intervention. In particular, a key ingredient of the CTI model is that postdischarge services are provided by a worker who has established a relationship with the client before he or she is discharged from the institution to the community. Workers were instructed to develop this relationship via multiple face-to-face contacts with the participant during the predischarge period. In our previous work, we established a threshold of at least three such predischarge contacts as minimally sufficient for this purpose (
15). In this study, 42 participants (55%) received three or more such contacts, whereas 35 (45%) received two or fewer contacts. The failure to deliver the desired number of predischarge contacts was most often the result of limited time between random assignment and the participant's discharge from the transitional residence. As noted earlier, our original plan was to recruit participants during their inpatient stay where delivering multiple predischarge contacts would not have presented a problem. Instead, we recruited in the transitional residences (in response to policy changes described above) where time to make contact with participants was limited by various factors, including significantly greater unpredictability in participants' discharge dates.
Definition of primary outcome
We defined as our primary outcome a dichotomous measure of homelessness during the last three follow-up intervals (18 weeks) of the study. Because the primary goal of CTI is to produce a long-lasting effect on homelessness risk, the key test of its efficacy is whether the risk of homelessness is reduced at the end of the observation period. We chose the final three intervals because we felt that the final six-week observation interval itself was too short to generate a stable estimate of the treatment effect. Although we also measured the actual number of nights spent homeless reported by participants during each follow-up interval, the highly skewed distribution of homeless nights we anticipated (and observed) led us to use the dichotomous measure as our primary endpoint.
Loss to follow-up
Although the proportion of the sample for whom we were unable to obtain complete follow-up data was low compared with that of other studies, it was not insubstantial. In order to verify the robustness of our findings, we carried out a multiple-imputation procedure employing five imputations and repeated the analysis. Our findings remained virtually unchanged.
Statistical analysis
Our primary analysis was an intent-to-treat (ITT) comparison testing whether there was a between-groups difference in risk of homelessness during the last three follow-up intervals of the study. This analysis was carried out with logistic regression that adjusted for baseline homelessness (number of homeless nights during the three-month period before the index hospitalization). As noted above, we elected to use a dichotomous measure of homelessness (ever versus never homeless in the last three intervals) as our primary endpoint because the distribution of homeless nights was highly skewed. We chose not to use survival analysis because such models are best suited for questions in which the primary interest concerns the length of time to the occurrence of an event, and our main interest was whether the CTI and usual services groups differed at the end of the observation period.
We also conducted several secondary analyses. First, we tested whether there was a group-level difference between participants assigned to the two groups on total number of homeless nights during the final three intervals. We used a Poisson regression model and adjusted for baseline homelessness.
Second, we performed an as-treated analysis in order to obtain an unbiased estimate of receipt of a version of the intervention that included three or more predischarge contacts with the worker. This analysis used the same outcome as in our primary ITT analysis (ever versus never homeless in the last three intervals). The analysis was carried out via a two-stage instrumental variables regression in which assignment to condition was the instrument and receipt of the intervention, including three or more predischarge contacts with the worker, was the treatment indicator (
16). Again, we adjusted for baseline homelessness.
Third, we examined homelessness over the full 18-month follow-up period. Using logistic regression and adjusting for baseline homelessness, we first compared the two groups with respect to risk of homelessness (ever versus never homeless) over 18 months. Using Poisson regression and adjusting for baseline homelessness, we then compared the two groups with respect to number of nights homeless over 18 months.
Results
Baseline characteristics of the sample are summarized in
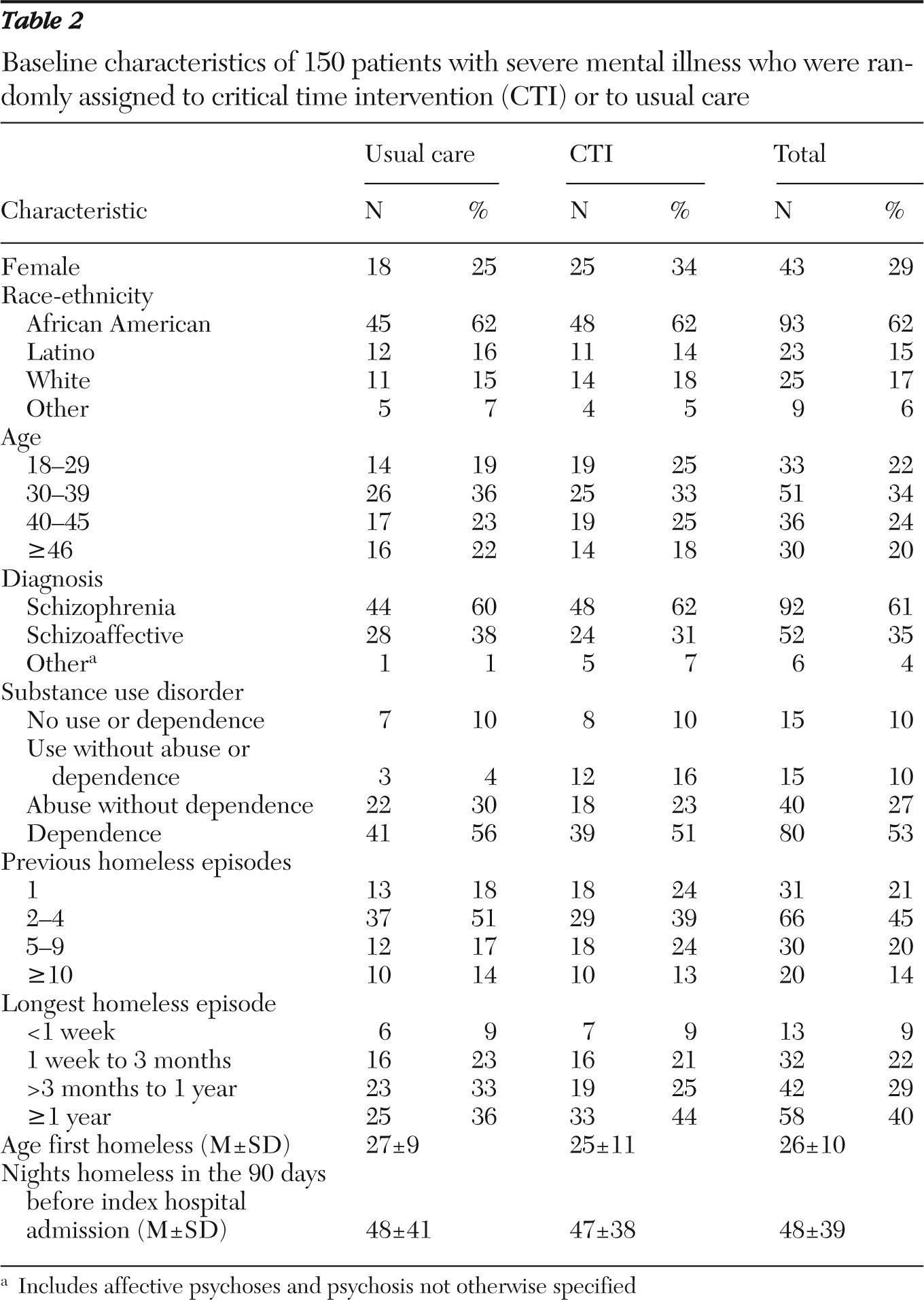
Table 2. There were 150 participants (71% men, and 29% women), with a mean±SD age of 37.5±9.5 years. Sixty-two percent of participants were African American. Sixty-one percent had a lifetime diagnosis of schizophrenia, and 35% had diagnoses of schizoaffective disorder. Comorbid substance use disorder was common, reflecting that the sample was drawn from persons who were previously homeless and difficult to place into housing; 53% met criteria for lifetime substance dependence, and another 27% met criteria for lifetime substance abuse without dependence. Most participants had extensive prior homelessness; 116 (79%) reported two or more previous homeless episodes, and 50 (34%) reported five or more such episodes. Forty percent of participants reported that the duration of their longest previous homeless episode was one year or longer. The mean length of stay in the transitional residences was 162±165 days (range of 6 to 937 days). There were no marked differences at baseline between the CTI and the usual care groups on any of these measures, and none was statistically significant according to chi square tests for categorical variables and t tests for continuous variables.
ITT analysis for homelessness in the last three intervals
Of the 117 participants with complete follow-up data, 31 (27%) experienced at least one homeless episode during the study.
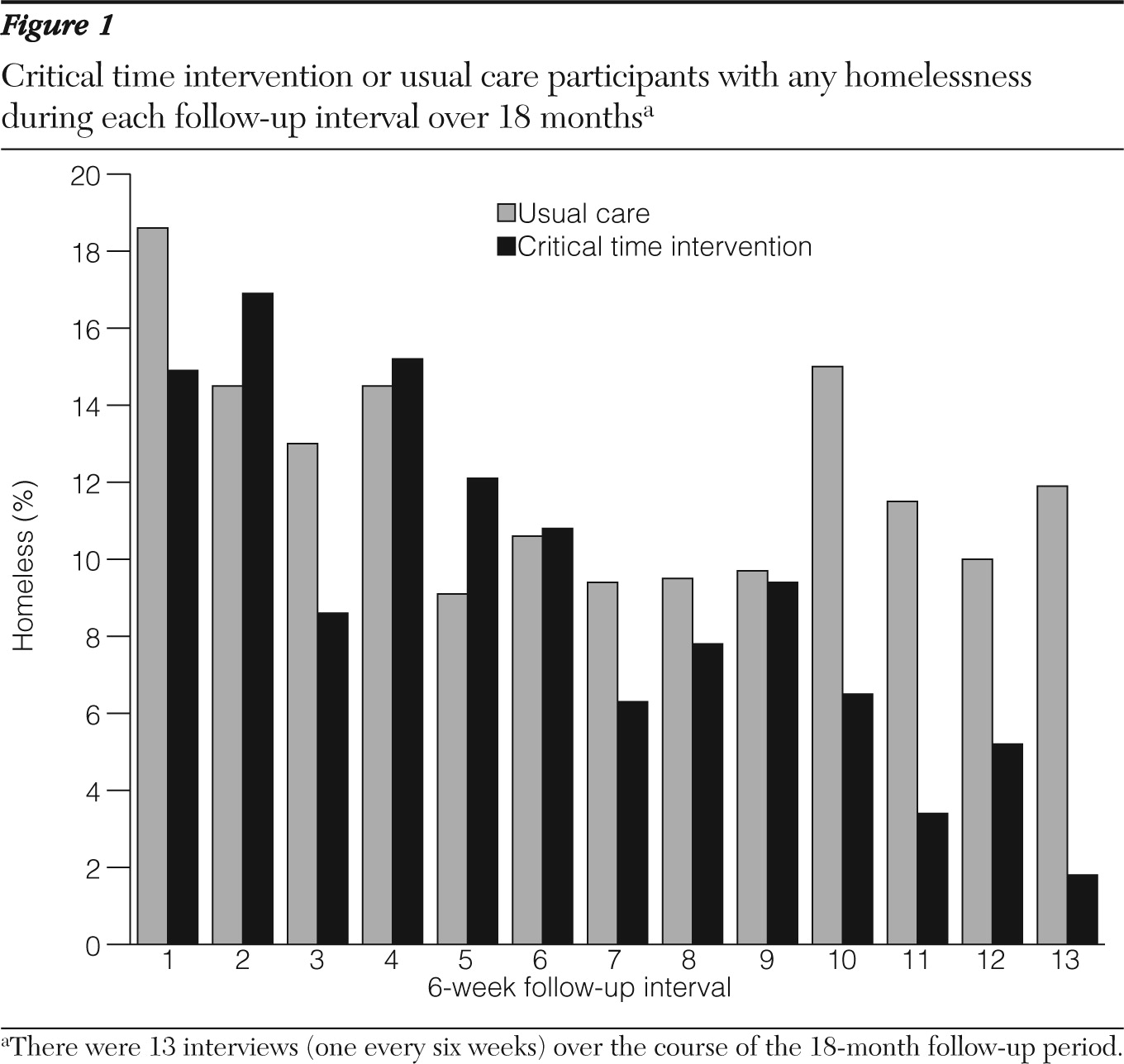
Figure 1 shows the proportion of participants in each condition who experienced at least one homeless night during each of the follow-up intervals. Among those with complete follow-up data, three of the 58 (5%) participants assigned to the CTI group experienced homelessness during the final three follow-up intervals, whereas 11 of 59 (19%) participants assigned to the control group experienced homelessness during this period. Using logistic regression to model the impact of assignment to CTI on homelessness during the final three follow-up intervals while controlling for baseline homelessness, we found that the odds of homelessness by treatment assignment was .22 (95% confidence interval [CI]=.06–.88). Thus assignment to CTI was associated with a statistically significant fivefold reduction in the odds of homelessness compared with assignment to usual care only. We then repeated these analyses, adjusting for sex, race-ethnicity, and age, and the results were unchanged.
Secondary analyses
Next we compared the total number of nights homeless for each group during the final three observation intervals. Those assigned to CTI had a total of six homeless nights during this period, whereas those assigned to the control group had 20 homeless nights. In the Poisson regression model that adjusted for baseline homelessness, this difference was statistically significant at p<.001.
We then compared the outcomes of participants assigned to CTI who received three or more predischarge contacts by the CTI worker with those who received fewer than three such contacts. In order to obtain an unbiased estimate of the impact of receiving this version of the intervention while controlling for all possible confounders, we used an instrumental variables approach (
16). We used a two-stage logistic model with homelessness during the last three intervals as the outcome, group assignment as the instrument, and receipt of three or more predischarge contacts as the treatment, again adjusting for baseline homelessness. In this analysis, we found that receipt of CTI with three or more predischarge contacts was associated with a statistically significant tenfold reduction in the odds of homelessness compared with assignment to usual care only (odds ratio [OR]=.10, CI=.03–.35). We repeated these analyses separately for men and women and found similar results.
Finally, we examined the impact of the intervention on homelessness over the full 18-month follow-up period. We first used logistic regression to model the impact of assignment to CTI on a dichotomous measure of homelessness over the 18 months, again controlling for baseline homelessness. For the CTI group, the OR was .28 (CI=.78–1.02), indicating that assignment to CTI was associated with a substantial reduction in the odds of homelessness compared with assignment to usual care, although the result was at the borderline of statistical significance. We then compared the total number of homeless nights accrued by participants in both groups. Among those assigned to CTI there were 1,812 total homeless nights, and among those assigned to the control group, there were 2,403 homeless nights. Poisson regression to control for baseline homelessness showed that this difference was statistically significant at p<.001.
Discussion
This is one of very few randomized trials of a carefully specified intervention designed to produce a lasting reduction in the risk of recurrent homelessness among persons with severe mental illness after discharge from inpatient psychiatric treatment. Our results support the findings of prior studies suggesting that CTI is an effective strategy for assisting formerly homeless individuals during the period of transition from institutional to community living. The magnitude of the protective effect was substantial, ranging from a fivefold reduction in homelessness risk in the ITT analysis to a tenfold reduction in the as-treated analysis. As in our previous trial (
10), the results were consistent with our view that a targeted, time-limited intervention applied during a high-risk period can have a salutary impact that endures beyond the point at which the intervention ends.
Despite its significant strengths, the study has several limitations. First, as noted above, we were not able to deliver the full intervention to all participants assigned to the experimental condition. This may account for the different pattern of results obtained relative to our original trial. In this study (as illustrated in
Figure 1), it took some time for outcomes between experimental and control groups to differ. We attribute this finding to the fact that a significant number of participants in the CTI group did not establish an adequate connection with the CTI worker before leaving the transitional residence, which then delayed the effect of the intervention. This is consistent with the stronger observed effect among participants who had more predischarge contact with the CTI worker.
Second, although the length of follow-up was relatively long by the standards of much clinical research, the degree to which the impact of CTI endures over a still longer period is unknown. Finally, homelessness was defined as the primary outcome and therefore was the sole domain we examined in this first report. We have, however, collected data relevant to a number of other important outcomes that will be investigated in subsequent analyses. We must also acknowledge the death of two study participants (one from cancer and one from pneumonia) who were assigned to the usual care group. We found no evidence that these adverse outcomes, both of which were reported in a timely way to the IRB, were directly related to or bear on the results of the study.
Conclusions
We have now shown through randomized trials in two different contexts that CTI had a substantial, lasting impact on reducing the risk of recurrent homelessness among persons with severe mental illness after their reentry to community living—results consistent with others' findings of a similar enduring effect in a nonrandomized trial (
11). Although the need for comprehensive, long-term support for persons with severe mental illness is undeniable, this work suggests that targeted, relatively brief interventions applied at critical transition points may enhance the effectiveness of long-term supports for persons with severe mental illness living in the community.
In this study, we applied such an intervention at one such time point; however, we believe that there are other “critical times” at which such interventions may also be effectively deployed, for example among persons with severe mental illness being discharged from jail or prison (
17). CTI might also be further adapted for transitions that, although not involving institutional discharge, nevertheless pose significant challenges to establishing effective and enduring supports (
18). For instance, approaches based on similar principles may be relevant for persons transitioning from more intensive service models, such as assertive community treatment, to less intensive ongoing sources of support (
19) or for new mental health consumers first entering the service system. Future research will be needed to determine whether and how the CTI model can be successfully used in these and other circumstances.
Acknowledgments and disclosures
This study was supported by grant R01MH59716 from the National Institute of Mental Health (D. Herman, principal investigator) and contributed personnel from the New York State Office of Mental Health. The authors thank James Bopp for facilitating implementation of the study. They also thank the CTI workers: Pablo Zapon, M.D., Leonida Gamboa, B.A., and Jorge Santiago, M.S.W. Alan Felix, M.D., Rufina Lee, Ph.D., and Maureen Hayes, Ph.D., provided clinical supervision. Research interviewing was carried out by Guillermo DiClemente, Ph.D., Laila Swydan, M.S.W., and Jennifer Manuel, Ph.D.
The authors report no competing interests.