A significant proportion of trauma survivors develop posttraumatic stress disorder (PTSD) (
1–
4). The estimated lifetime prevalence of PTSD in the U.S. population is about 7% (
1,
2). Chronic PTSD is tenacious and disabling (
5–
7). The likelihood of recovery decreases significantly during the year after trauma exposure (
1). Developing interventions to prevent PTSD is a pressing public health need (
8).
Effective prevention of PTSD requires accurate case identification, efficacious interventions, accessible services, and acceptance of care by trauma survivors at risk. Better understanding of these elements is crucial for service planning and delivery. Several indicators of the risk of chronic PTSD have been identified, including the presence of acute stress disorder (
9), the intensity of early symptoms (
10), and comorbid depression (
11,
12).
Controlled studies, reviews, and meta-analyses have established the efficacy of early, trauma-focused, exposure-based cognitive behavioral therapy in preventing PTSD (
9,
13–
15). The efficacy of cognitive therapy (
9), problem-based care (
16), and pharmacological interventions (
15,
17–
20) has not been established. Studies have also documented significant barriers to receipt of early care among civilians and military personnel (
3,
21–
23). Studies of individuals self-referred to treatment have recommended active outreach to trauma survivors who are at risk of PTSD (
3,
21,
22). In line with that recommendation, a “screen and treat” approach, which was used after London's 2005 terrorist attacks (
23), was found to generate more accurate treatment referrals than self-referral or a referral by a general practitioner. Barriers to care in outreach programs have not been evaluated. The long-term effect of refusing treatment shortly after trauma exposure is unknown.
This article reports service utilization data from a large study of systematic prevention of PTSD by means of early treatment. The study reported here evaluated the acceptance of clinical care, the accuracy of early assessments, and the consequences of declining an offer of care after careful assessment. Briefly, the research team reached out to all adults who were admitted over four years to a general hospital emergency department after they had experienced an event generally regarded as traumatic. Those who had a qualifying traumatic experience and early symptoms were offered clinical assessment and treatment. To evaluate the accuracy of referral for care and the effect of declining it, follow-up data were obtained for all those who participated in the initial assessment regardless of and blind to their acceptance of clinical assessment or treatment.
Methods
Participants
Candidates for the study were survivors of potentially traumatic events who were between the ages of 18 and 70 and who were admitted to the emergency department at Hadassah University Hospital in Jerusalem between June 2003 and October 2007. Patients were eligible for the study if they resided within an hour's drive of Jerusalem and could attend treatment. Potential participants were not included if they sustained an injury that required more than seven days of hospitalization, had loss of consciousness on admission to the emergency department, or had medical or surgical conditions that interfered with their ability to participate or provide informed consent.
Eligible participants received a telephone call from three to 21 days from being seen in the emergency department. Participants who were not reached after ten attempts were classified as “not reached.” Participants who were reached but who declined to take the call were classified as “declined.” Participants in the telephone interviews were invited to undergo a clinical assessment if they had experienced a traumatic event that met
DSM-IV PTSD criteria A1 and A2: an event that involved actual or threatened death or serious injury or a threat to the physical integrity of self or others (A1); to which the person's response involved intense fear, helplessness, or horror (A2). To be invited, individuals also had to be sufficiently fluent in Hebrew, Arabic, or English to reliably answer questionnaires and interact in clinical assessments and to have acute stress disorder symptoms or symptoms of acute stress disorder without either the dissociation or the avoidance criterion (
24–
27).
Individuals who underwent the clinical assessment were invited for treatment if they met DSM-IV diagnostic criteria for acute PTSD (except for the one-month duration) or met these criteria without the dissociation or avoidance criterion. They were not invited if they reported a current or past psychotic disorder or bipolar disorder or if they had current substance abuse or dependence, required urgent clinical attention for another condition (such as suicidal ideation), had chronic PTSD, or were receiving mental health treatment elsewhere.
Hadassah University Hospital's Institutional Review Board approved and monitored the study. Participants provided oral assent for telephone interviews and written informed consent for clinical assessments, randomization, and treatment. The study's
ClinicalTrials.gov registration is NCT00146900.
Instruments
Interviewer administered instruments.
The Clinician-Administered PTSD Scale (CAPS) (
28) was used to assess for a diagnosis of PTSD; the scale also indicates the severity of PTSD symptoms. Possible scores range from 0 to 136, with higher scores indicating more severe symptoms. To make a diagnosis of PTSD, a symptom was rated as present when its frequency score was 1 or higher and its severity score was 2 or higher (
29).
The Structured Clinical Interview for DSM-IV (SCID-IV) (
30) evaluated the presence of current and lifetime
DSM-IV axis I disorders other than PTSD. The Post-traumatic Stress Symptom Inventory-Interviewer's Version (PSS-I) (
31) and the Acute Stress Disorder Symptom Scale (ASDS) (
32) were used in telephone interviews to assess PTSD and acute stress disorder. To enable administration by telephone, these instruments were modified to provide a yes-no answer to each symptom criterion. Thus the PSS-I total score (range 1–17) represents the number of PTSD symptoms endorsed.
During telephone interviews the K6 (
33) was administered to evaluate nonspecific psychological distress. Possible scores range from 6 to 30, with higher scores indicating more distress. To evaluate global illness severity the Interviewers' Clinical Global Impression scale (CGI-I) and the Participants' Clinical Global Impression scale (CGI-P) were used (
34). Scores on both range from 1, normal, to 7, severely ill.
Self-report instruments.
Self-report instruments included the self-administered version of the PSS (PSS-SR) (
35) and the Beck Depression Inventory (BDI) (
36). Scores on the PSS-SR range from 0 to 51, with higher scores indicating higher levels of PTSD symptoms. Scores on the BDI range from 0 to 56, with higher scores indicating higher levels of depression.
Procedure
Telephone interviews.
Computerized records of emergency department trauma admissions were screened for inclusion and exclusion criteria within 24 hours of admission, and research interviewers were provided with a list of telephone numbers. In the first telephone interview, the interviewer explained the purpose of the study and obtained oral consent for participating in the interview. The interviewer ascertained the occurrence of a traumatic event that met DSM-IV PTSD criterion A. The interview was terminated if such an event had not taken place. When criterion A was met, the interviewer administered the instruments described above (“long interview”). Long-interview participants who met the study's inclusion criteria were invited to undergo the clinical assessment. If the interviewer was in doubt about referral, the case was discussed at a weekly consensus meeting for final decision.
All participants who had experienced a traumatic event that met DSM-IV criterion A and a randomly selected 10% of those who had not experienced an event that met criterion A received a second telephone interview. The second interview took place after termination of treatment (for treatment participants) and at a similar time for those who did not attend treatment. The mean±SD time from the emergency department visit to the second interview was 224.9±39.1 days. The second interview replicated the long interview format of the first telephone interview. The interviewers were blind to whether the interviewees had participated in clinical assessments and treatment.
Clinical assessments.
The initial clinical assessment took place a mean of 19.8±5.2 days from the emergency department. The clinician explained the study, obtained written informed consent, and administered the study's instruments. Participants who met the inclusion criteria described above received an explanation of the study's four treatment arms: exposure-based cognitive-behavioral therapy, cognitive therapy, a blind condition in which either a selected serotonin reuptake inhibitor or a placebo was prescribed, and a waitlist condition. Participants in the waitlist condition received late exposure-based CBT five months after the traumatic event. Participants were then randomly assigned to a treatment arm, and an appointment for the first treatment session was scheduled.
Randomization to treatment.
We used equipoise-stratified randomization (
37) for the randomized controlled trial. This method allowed a participant to decline up to two undesired treatment modalities (including the waitlist) without being excluded from the study. Ultimately, no consenting participant was excluded from receiving treatment at this stage.
Statistical analyses
Descriptive statistics were used to account for proportions of participants at each step. Repeated-measures analysis of variance (ANOVA) was used to evaluate the consequences of participants' and interviewers' decisions to continue or stop participation in the study.
Results
Acceptance of telephone interviews
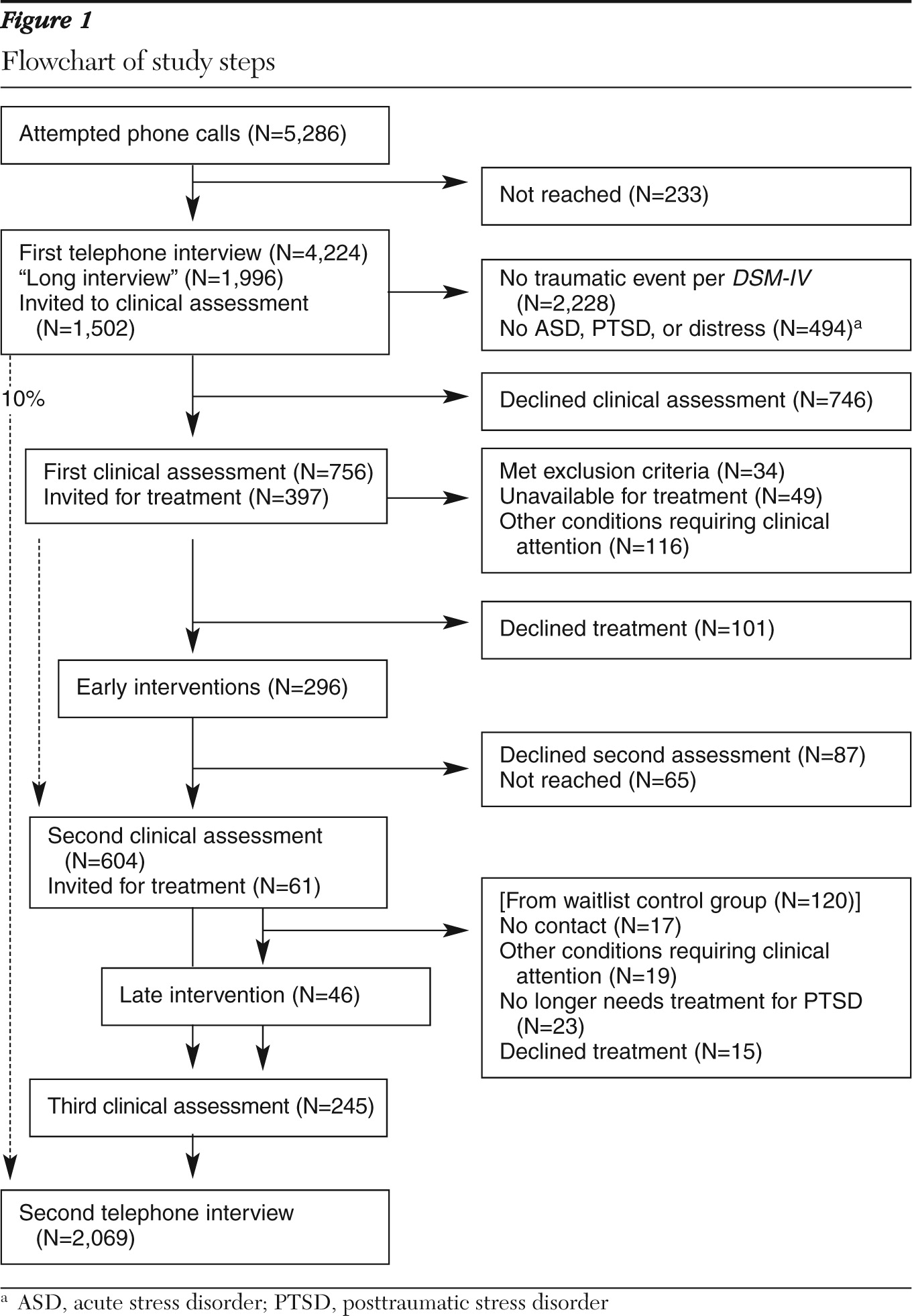
We made calls to 5,286 individuals and reached 5,053 (96%). A total of 310 potential participants (6%) declined the first telephone interview, and 519 (11% of the remaining 4,743) did not meet the study's inclusion criteria, which left 4,224 valid participants (
Figure 1). Individuals who refused the initial interview were older than those who agreed to be interviewed (t=3.09, df=5,051, p<.005).
Presence of DSM-IV traumatic event
During the initial telephone interview, interviewers determined that for 2,228 participants (53%) the traumatic event did not meet DSM-IV criterion A. In most cases (N=2,014, 91%) the determination was made because the interviewee did not endorse the criterion of intense fear, helplessness, or horror. Compared with the interviewees who experienced events that did not meet criterion A, the 1,996 who experienced such events were more likely to be women (54% compared with 43%; χ2=56, df=1, p<.005) and to be survivors of motor vehicle accidents or terrorist actions (for all trauma types, χ2=466, df=3, p<.005).
Acceptance of clinical assessment
On the basis of the criteria described above, we invited 1,502 participants to undergo the initial clinical assessment. Half (N=746, 50%) did not attend the assessment: 306 (41%) explicitly declined during the first telephone interview, 194 (26%) did not show up at the scheduled assessment despite three telephone reminders, 97 (13%) canceled the assessment because they reported feeling better, 89 (12%) could not attend for logistical reasons (such as distance from the treatment site or work obligations), 37 (5%) did not attend because of physical problems related to their injury, and 23 (3%) started treatment elsewhere.
Compared with persons who declined the initial clinical assessment, those who underwent the assessment had significantly higher levels of PTSD symptoms as measured by the PSS-I (p<.001). They also had higher CGI-P and CGI-I scores (p<.001 for both) and higher K6 scores (p<.001).
To evaluate the effect of injury on the acceptance of clinical assessment, we compared participants who were admitted to the hospital for treatment of their injury (N=183) with those who were released to their homes from the emergency department (N=1,319). Admitted individuals were significantly more likely to attend the initial clinical assessment than those who were not admitted (58% and 49%, respectively, p<.04) (data not shown).
Clinical assessment and treatment referral
Axis I disorders.
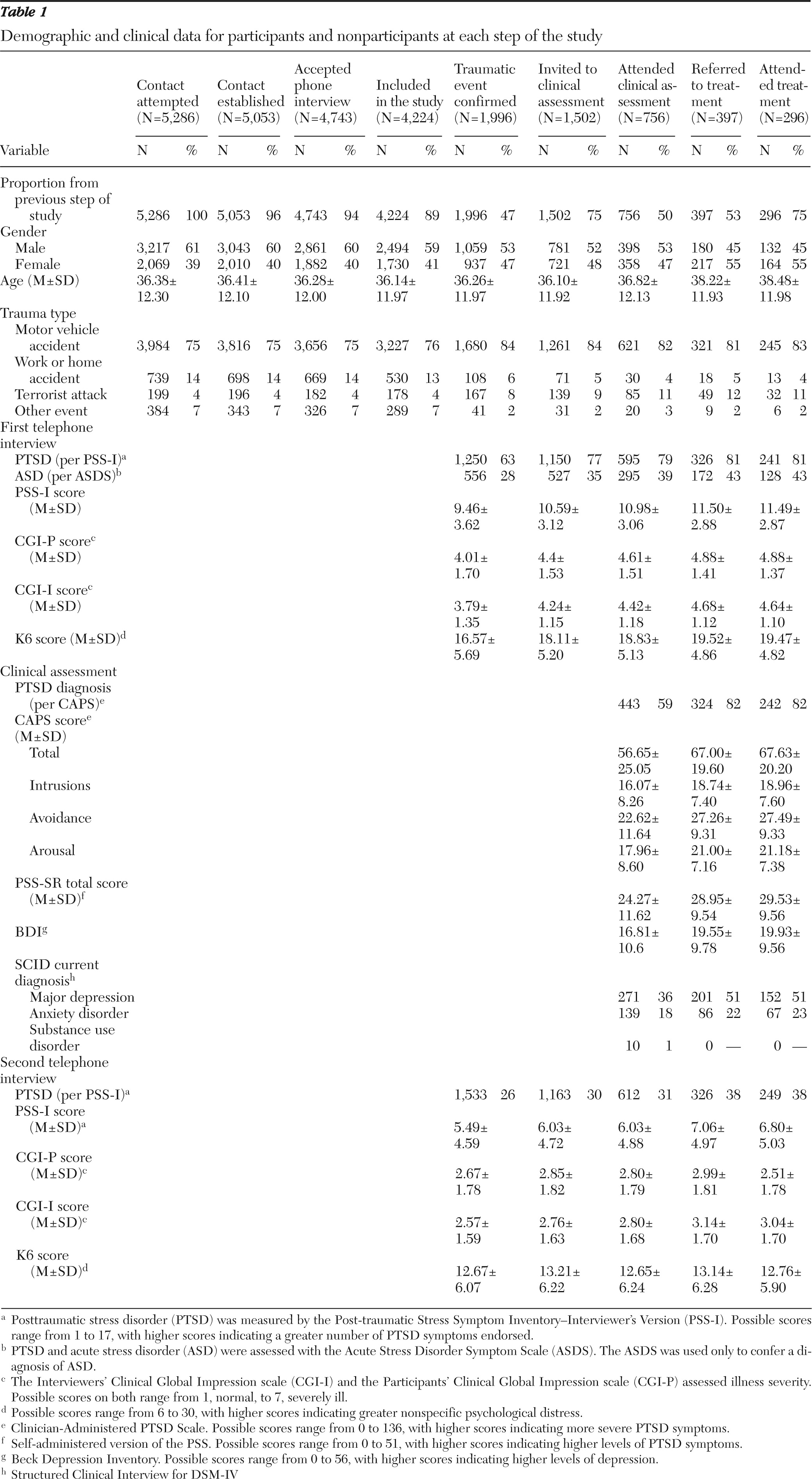
Of the 756 participants who underwent the initial clinical assessment, 443 (59%) were given a diagnosis of PTSD (except for the duration criterion) (
Table 1). A diagnosis of current major depression was given to 271 participants (36%), and of this group 255 (89%) also had a PTSD diagnosis. A total of 139 participants (18%) had an anxiety disorder other than PTSD, and 91 persons in this group (66%) also had a PTSD diagnosis. Other disorders diagnosed at the initial clinical assessment were substance use disorders (ten participants, two of whom also had a PTSD diagnosis), somatoform disorder (N=10, seven with PTSD), eating disorders (N=2, both with PTSD), and other axis I disorders (N=5, two with PTSD). Overall, 64% (N=285) of the 443 participants given a PTSD diagnosis at the initial clinical assessment had a comorbid axis I disorder.
Treatment eligibility and referral.
Of 756 persons who underwent the initial clinical assessment, 34 (5%) met the study's exclusion criteria (15 with chronic PTSD, 13 with language problems, and six unable to understand instructions). In addition, 49 (7%) were unavailable for treatment (43 were soldiers, and six had started treatment elsewhere), and 116 had other conditions requiring urgent clinical attention. Among the remaining 557 persons, 160 (29%) did not have the required acute PTSD. Thus 397 persons were invited for treatment. The CAPS scores of those who were invited for treatment were similar to the CAPS scores of participants in a previous controlled trial of early cognitive-behavioral therapy (67.0±19.0 and 70.6±17.7) (
13). Compared with the group not invited for treatment, the group invited for treatment had a larger proportion of women (39% and 55%, respectively) and of persons who had experienced terrorist attacks (23% and 58%) (p<.005 for both). The prevalence of other axis I disorders did not differ significantly between groups.
Acceptance of treatment
Of the 397 participants invited for treatment, 296 (75%) attended treatment. Those who attended did not significantly differ from those who did not attend on any study variable except injury severity; those who attended treatment had scores indicating greater injury severity (4.20±1.57 compared with 3.60±1.60, p<.005).
Second telephone interview
We attempted to contact 2,069 participants for a second telephone interview: 1,853 of those originally included in the initial “long telephone interview” and 216 of those initially excluded because they did not experience a traumatic event. Of these, we reached 2,015 (97%), and 1,794 (89%) agreed to be interviewed. Those who agreed and those who declined did not differ significantly in age, gender, trauma type, and symptom scores at the first telephone interview.
Effect of declining assessment and treatment
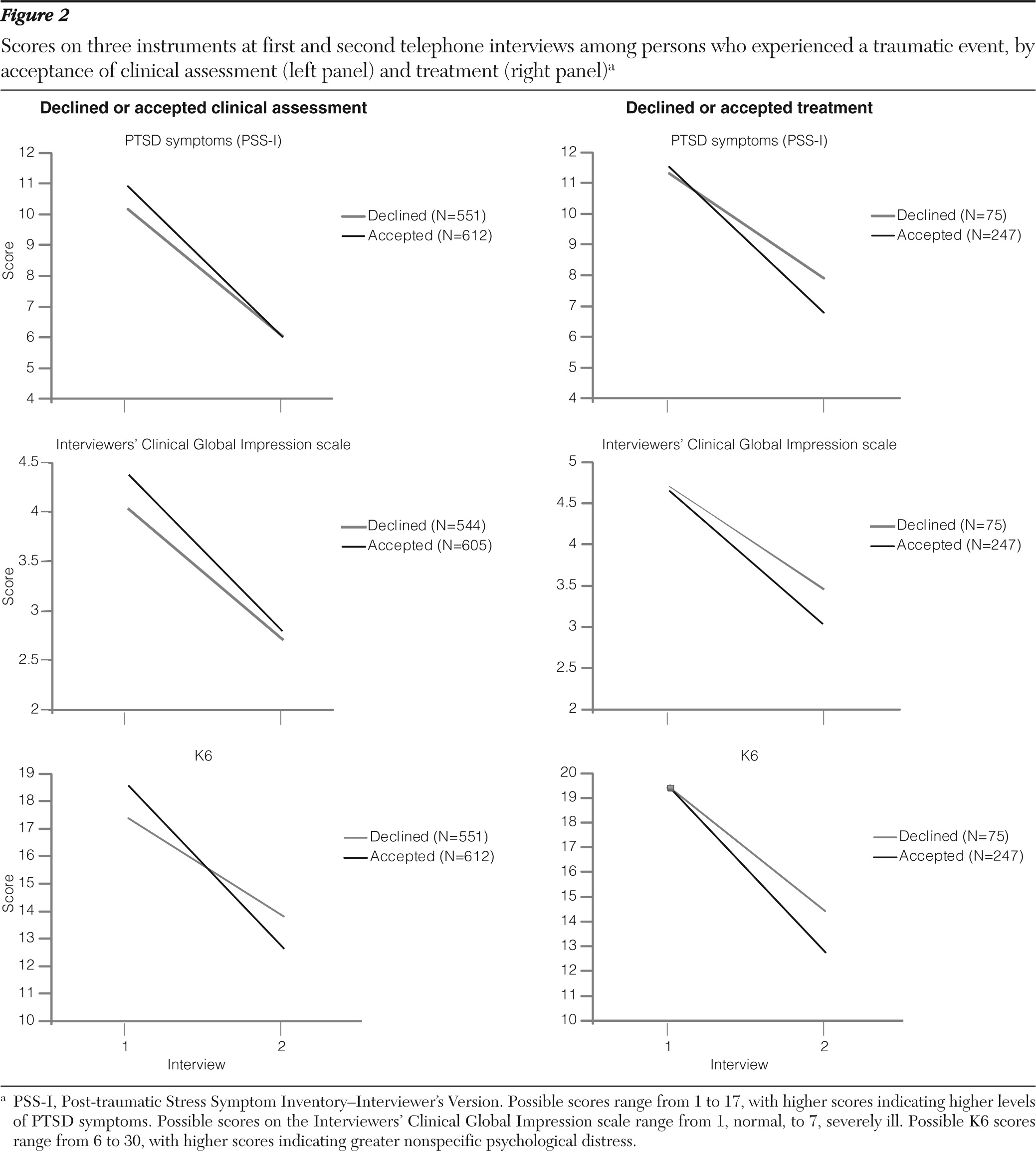
Persons who agreed to undergo the initial clinical assessment experienced a steeper decline in PTSD symptoms between the first and second telephone interviews (
Figure 2). Repeated-measures ANOVAs used assessment acceptance status (accepted or declined the initial clinical interview) as the grouping factor and PSS-I scores at the first and second telephone interviews as the within-subjects factor. These analyses indicated a significant main effect of time (F=1,101.62, df=1 and 1,161, p<.001) and a significant group-by-time interaction (F=7.56, df=1 and 1,161, p<.01). The main effect of group showed a trend toward significance (F=3.75, df=1 and 1,161, p=.053).
The differences remained statistically significant after the analysis controlled for initial K6 and both CGI scores (F=6.92, df=1 and 1,152, p<.01). The PSS-I scores at the first telephone interview were significantly higher for those who agreed to the initial assessment than for those who declined (10.92 and 10.17, respectively), indicating greater symptom severity. At the second telephone interview, however, the scores for these two groups did not differ significantly (6.03±4.88 and 6.04±4.54, respectively). Group-by-time interactions were also found for K6 scores (F=38.42, df=1 and 1,139, p<.001), CGI-I scores (F=10.02, df=1 and 1,147, p<.002), and CGI-P scores (F=17.30, df=1 and 1,154, p<.001).
To control for the effect of receiving treatment, we conducted an ANOVA without the 296 participants who attended treatment. The result indicted a significant main effect of time (F=969.30, df=1 and 1,001, p<.001) and a significant group-by-time interaction (F=6.30, df=1 and 1,001, p<.02). The main effect of group was not significant.
As in the analysis above, individuals who accepted treatment after the assessment had steeper declines in symptoms than those who did not (
Figure 2). Repeated-measures ANOVAs showed a significant main effect of time (F=164.40, df=1 and 324, p<.001) and a significant group-by-time interaction (F=4.74, df=1 and 234, p.<.02). The main effect of group was not significant. PSS-I scores at the first telephone interview were 11.58±2.85 for those who accepted treatment and 11.32±2.92 for those who declined. At the second telephone interview, PSS-I scores were 6.80±5.01 and 7.92±4.78, respectively.
Interviewers' error
Not identifying trauma.
After the first telephone interview, 2,228 persons were judged not to have experienced a traumatic event. A random sample of 216 (10%) were assessed via a second telephone interview, and eight (4%) were given a diagnosis of PTSD. However, three of them (1%) had experienced another traumatic event since the first telephone interview, leaving a net prediction error of 2%. Among participants judged to have experienced a traumatic event at the first telephone interview, the prevalence of PTSD was 26% (N=398).
Not referring for clinical assessment.
Among the 365 participants who were not referred for clinical assessment after the first telephone interview, 40 (11%) were given a diagnosis of PTSD at the second telephone interview. Seven of this group (2%) had experienced another traumatic event since the first telephone interview, leaving a net prediction error of 9%. Notably, among persons who were not referred for clinical assessment, PTSD symptoms increased significantly between the first and second telephone interviews as measured by the PSS-I (7.56±3.52 to 11.20±2.69, t=5.28, df=44, p<.001).
Not referring to treatment.
Of the 140 participants who were not referred for treatment after the assessment, four (3%) were given a diagnosis of PTSD, including one (1%) who had experienced another traumatic event (a net prediction error of 2%).
Discussion
The findings of this study indicate that among persons who were experiencing symptoms after a traumatic event, acceptance of early assessment and treatment was limited, even with systematic outreach. Telephone-based assessments were more readily accepted (96%) than in-person clinical assessments (50%). One out of four symptomatic survivors of a traumatic event declined an offer of treatment after seeing a clinician. Those who accepted assessment and treatment showed a steeper decline in PTSD symptoms between the first and second (posttreatment) interviews. Both a short screening that used DSM-IV PTSD criterion A and clinical assessment at one month had low false-negative errors.
Avoidance of early care is not limited to military personnel in a war zone (
3) or to survivors of mass trauma (
22,
23) or to survivors of traumatic events who must seek help on their own (when outreach is not offered). In contrast to a previous study (
21), participants who declined assessments in this study were less symptomatic than those who accepted assessment.
These results should be interpreted within the context of the study. The design reflects an attempt to alleviate some of the previously described barriers to care (
3,
21–
23) by proactive outreach, early assessment, and prompt treatment referral. Goldberg and Huxley (
38) described three successive “filters” to obtaining mental health care: the individual's own propensity to recognize a problem and seek help (“illness behavior”), providers' detection of an illness, and referral to mental health care. Within that framework, this study provided detection of illness regardless of illness behavior and offered readily available treatment without the usual help seeking. Consequently, participants' decisions to accept treatment in this program were not constrained by the need to seek help or by service availability and thus can be seen as closely reflecting their unconstrained choices. Notwithstanding, the majority of those with identified risk opted not to receive treatment for PTSD.
Our sample consisted of survivors of brief traumatic events who were seen in an emergency department for diagnosis and treatment of an injury. Most were previously healthy. Notably, our sample was taken from the daily stream of persons seen in an emergency department, which allowed us to sequentially screen, evaluate, and treat. Among civilians, incidents such as road traffic accidents and assaults are the major sources of new PTSD (
2,
3). In addition, because patients were told that assignment to treatment would be random, the desirability of treatment may have been affected. However, allowing participants to decline up to two treatment modalities without being excluded from the study presented them with an array of options that resembles—or might be an improvement on—the “usual care” option.
The cost of declining care
A replication of the U.S. National Comorbidity Study found that the failure of persons with mood and anxiety disorders to make prompt initial treatment contact is a “pervasive aspect” of these disorders; the authors postulated that “interventions to speed initial treatment are likely to reduce the burdens and hazards of untreated disorders” (
39). In support of this observation, our study found less improvement among participants who declined assessment or treatment compared with those who accepted it. Interpreted parsimoniously, this finding suggests that declining care does not reflect inner strength or resilience.
Interviewers' prediction error
The low prevalence of PTSD among participants who were excluded for not meeting the DSM-IV traumatic event criterion (PTSD criterion A) is encouraging, given the short time that was allocated for that assessment to make that determination (about five minutes of the “short interview”). This finding suggests that DSM-IV criterion A2 (the person's response involved intense fear, helplessness, or horror) can be used shortly after an event to effectively identify survivors at low risk for PTSD.
In contrast, the prevalence of PTSD (11%) among persons who were not referred for a clinical assessment was far from negligible. Our observations indicated that many developed new PTSD symptoms between the first and second telephone interview and thus could not be identified as being at risk shortly after the traumatic event. Thus we conclude that the results of a single assessment ten days after a traumatic event should not be used to restrict access to treatment.
In terms of detecting PTSD the best decision node was the clinical assessment. This is likely due to the combined effect of later timing (one month after the emergency department visit), depth (structured clinical interviews), and a prior screening (the initial telephone interview). The improved detection rate, therefore, reflects the merit of sequential evaluations.
Burden on services
The 296 participants who attended treatment represent 6% of those initially reached by telephone, 15% of those who experienced a confirmed traumatic event, and 20% of those who were invited for a clinical assessment. During the four years of the study, on average 7.4 patients began new treatment episodes each month, which is well within the capacity of a dedicated clinical service. Even if the number of patients accepting treatment were twice as high, the workload would remain within a reasonable limit.
The burden of screening and evaluation was significant. Data from administrative records indicated that to bring one patient to treatment required an average of 6.93 hours of telephone interview time and 5.09 hours of clinical assessment time. Collecting research data (for example, via questionnaires and structured interviews) clearly increased the time allocated to screening and evaluation. However, the main source of this burden is the unavoidable inclusion in early assessments of persons who experience early symptoms and spontaneously recover. Prevention programs must make a difficult choice: either allocate significant resources to assessment or provide expensive treatment to persons who are not properly evaluated, some of whom who may not need such treatment.
A limitation of this study was the inclusion of adult civilians who experienced short and salient events after which they were seen in an emergency department of one hospital. Many psychologically traumatized individuals do not refer themselves to medical emergency services or to other treatment facilities (
39). These individuals, along with victims of prolonged adversities, such as family violence or abuse, were not represented in our sample. Finally, this study did not use qualitative methods to explore reasons for declining care. Future studies should go beyond identifying who declines care to shed light on why care is declined.
Conclusions
This study extended findings of previous studies of short screening instruments (
25,
40) for use with persons who have experienced traumatic incidents. This work demonstrated the efficacy of using the
DSM-IV PTSD A2 criterion for identifying survivors at low risk of PTSD. Among those not meeting criterion A2, the low endpoint prevalence of PTSD (about 2%) suggests that shortly after a traumatic event, failure to meet this criterion is associated with a very low risk of developing PTSD.
This study traced the boundaries of a comprehensive outreach program and outlined its significant burden on services. Systematic outreach may be justified during extreme events, such as mass casualty trauma or terror attacks, when the high odds of survivors' developing PTSD (
41) reduce the proportion of initial interviewees who recover and therefore may justify allocation of significant resources to screening and evaluation.
The findings illustrate a limitation to the provision of clinically appropriate care—that is, the difficulty of bringing survivors of traumatic events to clinicians. Participants' greater willingness to accept a telephone interview (compared with an in-person interview) suggests that more attention should be paid to telephone-based or media-based CBT (
42) versus treatment within medical facilities.
Finally, participants who had chronic PTSD and those who had co-occurring conditions that required urgent attention were excluded from the study. At eight months, however, 58% of persons with prior PTSD in this study and 56% of those with a serious co-occurring disorder had PTSD. Survivors with complex conditions who are unable to begin early treatment constitute a risk group and should be followed.
Acknowledgments and disclosures
This work was supported by a generous contribution from the Jerry Lee Foundation, a service development grant from the Jewish Federation of New York, grant R43-MH071652 from the National Institute of Mental Health, and an investigator-initiated research grant from Lundbeck Pharmaceuticals Ltd.
Dr. Shalev received an investigator-initiated grant from Lundbeck Pharmaceuticals Ltd. for this study and for a multicenter study (“Prevention of PTSD by Escitalopram”). The other authors report no competing interests.